The Efficacy of Injectable Atelocollagen in Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-Analysis
Mohamed Zahed, Ziad El Menawy, Mahmoud Elmesalmi, Nour Elnaggar, Farouk Ahmed, Mahmoud Odeh, Rawad M Azaz, Seifeldin H Amer, Mahmoud M Mourad, Ahmad Ali

TL;DR
This study reviews the effectiveness of using injectable atelocollagen during arthroscopic rotator cuff repair, finding no significant benefits but a trend toward better healing.
Contribution
The paper provides a systematic review and meta-analysis of atelocollagen's role in rotator cuff repair, highlighting trends despite non-significant results.
Findings
Atelocollagen showed a non-significant lower retear rate compared to controls.
Pain and functional outcomes showed no significant improvement with atelocollagen.
Shoulder range of motion differences were also non-significant.
Abstract
A rotator cuff (RC) tear can result in shoulder dysfunction and pain. Arthroscopic repair has been used for complete or advanced partial tears. However, the rates of retear and non-healing remain a challenge postoperatively. We aim to investigate the efficacy of injecting atelocollagen in combination with arthroscopic repair in patients with complete or partial RC tears. We performed an electronic search using PubMed, Scopus, Web of Science, and the Cochrane Library up to the 7th of October 2025. Randomized controlled trials (RCTs) and cohort studies that evaluate atelocollagen as an adjunct to arthroscopic repair of RC tears were included. Primary outcomes were retear rate (Sugaya IV-V) and pain (visual analog scale (VAS)), and functional outcomes (American Shoulder and Elbow Surgeons score (ASES) and Korean Shoulder Score (KSS)) at 12 months. Additionally, we evaluated the overall…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
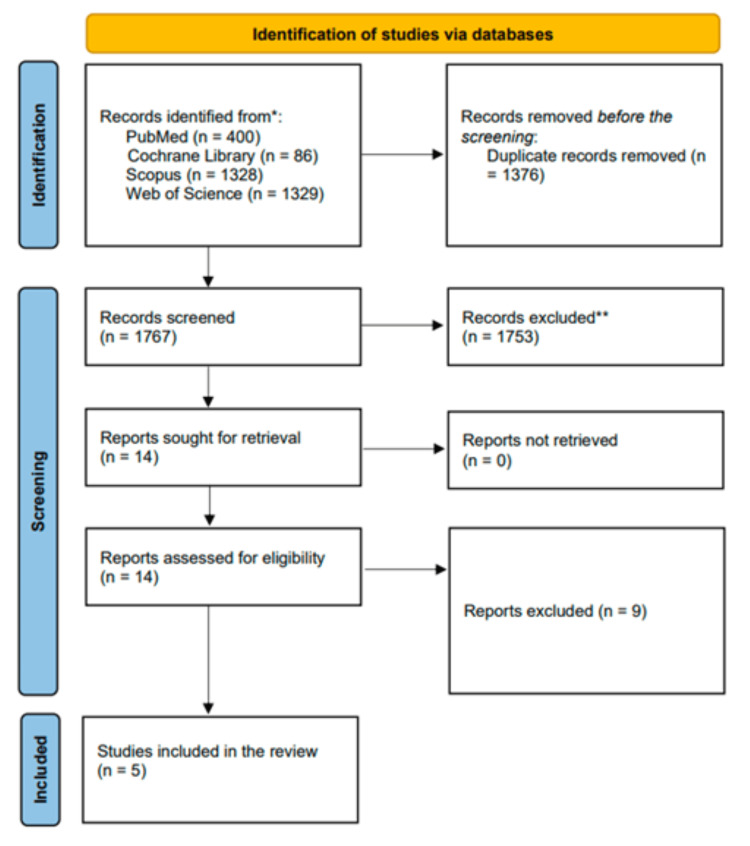 Figure 1
Figure 1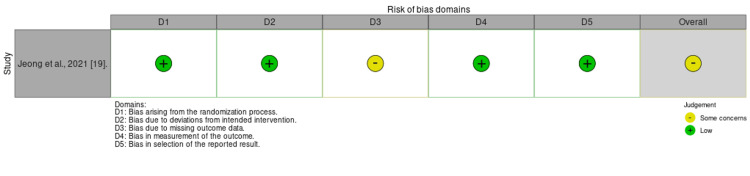 Figure 2
Figure 2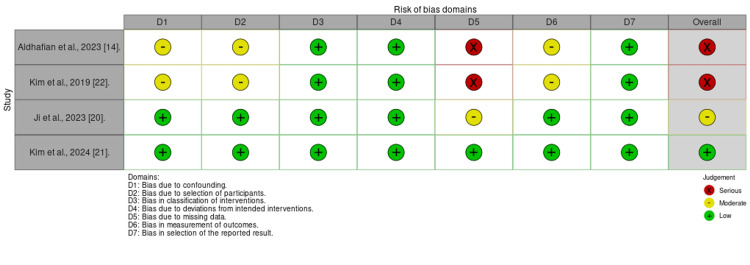 Figure 3
Figure 3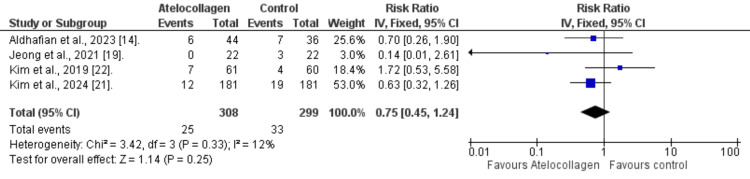 Figure 4
Figure 4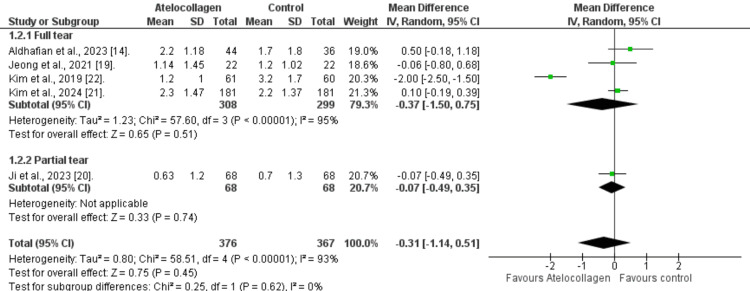 Figure 5
Figure 5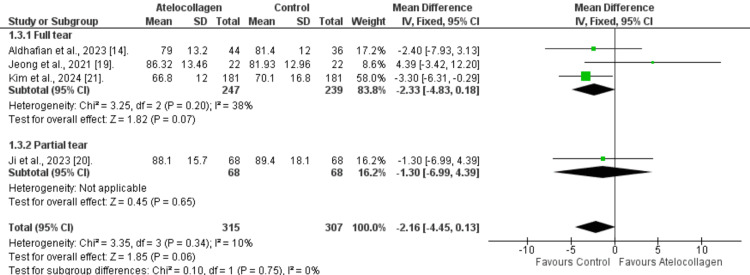 Figure 6
Figure 6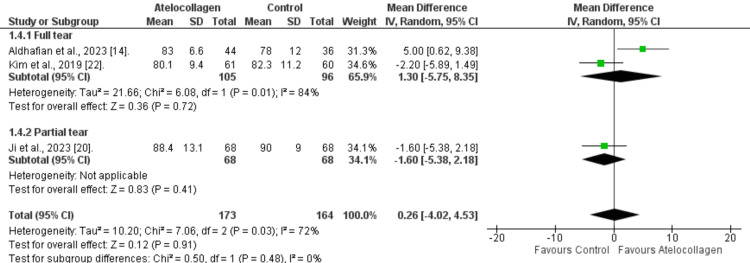 Figure 7
Figure 7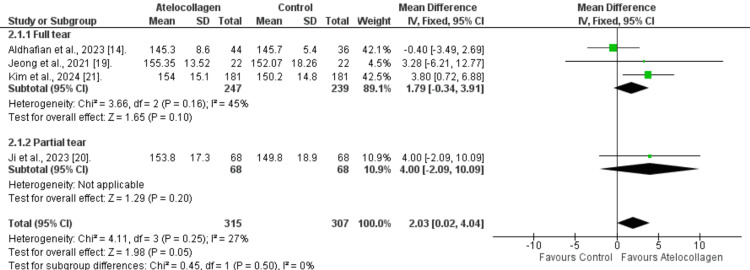 Figure 8
Figure 8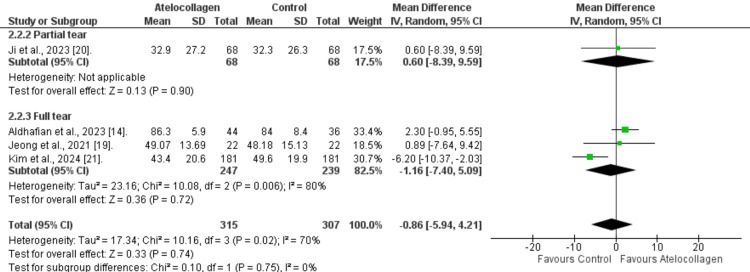 Figure 9
Figure 9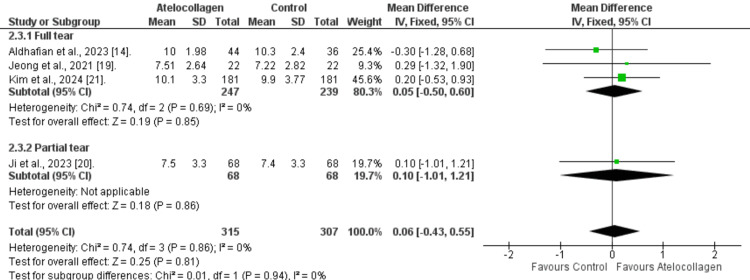 Figure 10
Figure 10| Study (author, year) | Country | Study design | Sample size (intervention/ control) | Tear type | Atelocollagen form | Comparator | Follow-up duration (months, mean ± SD) | Imaging modality |
| Aldhafian et al., 2023 [ | South Korea | Retrospective cohort | Group 1: 36 (arthroscopic repair only) Group 2: 44 (Atelocollagen) Group 3: 49 (ADM Allograft) | Full-thickness supraspinatus tears (<5 cm), repairable | Injectable/Gel-Type Type I Atelocollagen, 1 mL intraoperative injection at tendon-bone interface | Standard arthroscopic repair without augmentation | I: 20.0 ± 6.3, C: 21.6 ± 5.1 | MRI (2 and 12 months post-op) |
| Jeong et al., 2021 [ | South Korea | Prospective RCT | 22 (Atelocollagen + HA) / 22 (Control, No Injection) | Full-thickness rotator cuff tears (repairable, type I) | Injectable Type I atelocollagen (3 mL, co-administered with 3 mL HA) | Standard arthroscopic repair without atelocollagen or HA | 12.1 ± 1.5 (I), 11.8 ± 0.8 (C) | MRI at 12 months (3.0T, Sugaya classification) |
| Ji et al., 2023 [ | South Korea | Retrospective cohort | 68 / 68 | High-grade partial articular supraspinatus tendon avulsion (PASTA) lesions (Ellman grade 3) | Injectable / Gel-type porcine Type I Atelocollagen (1 mL, 3 mg/mL) | Transtendon repair without augmentation | ≥ 24 months (minimum 2 years) | MRI (6 months, 1 year) |
| Kim et al., 2019 [ | South Korea | Retrospective cohort | 61 / 60 | Full-thickness supraspinatus tear (± infraspinatus/subscapularis) | Injectable/Gel-type Type I porcine atelocollagen (RegenSeal, 3 mL) applied intraoperatively at bone-tendon interface | Standard arthroscopic rotator cuff repair without atelocollagen | 26.7 months (mean), MRI at 6.4 months | MRI (1.5 T) using the Sugaya classification for patients. |
| Kim et al., 2024 [ | South Korea | Retrospective propensity score-matched comparative study | 181 / 181 | Small- to medium-sized full-thickness rotator cuff tears (DeOrio&Cofield classification) | Injectable atelocollagen (3 mL, Coltrix Tendoregen, Ubiosis) injected at bone-tendon interface | Arthroscopic rotator cuff repair without atelocollagen injection | 22.5 ± 9.0 (I) / 21.8 ± 9.6 (C) | MRI (3.0-T, postoperative at 6 months) |
| Study | Group | Mean age (years) | Male (%) | Tear size (cm, A–P × M–L) | Goutallier stages, grade 0:1:2:3:4 | Affected shoulder (right:left) | Symptom duration (months) | Surgical technique | ||
| Subscapularis | Supraspinatus | Infraspinatus | ||||||||
| Aldhafian et al., 2023 [ | Intervention | 63.0 ± 8.0 | (20) 45.5 % | A–P = 1.9 ± 0.9 M–L = 2.1 ± 0.9 | 8:23:11:2:0 | 5:23:15:1:0 | 6:27:10:1:0 | NA | Not reported | Predominantly double-row suture bridge (some single-row Mason-Allen); biceps tenotomy/tenodesis for associated biceps pathology as needed |
| Control | 63.2 ± 8.3 | (10) 27.8 % | A–P = 1.5 ± 0.7 M–L = 2.0 ± 0.9 | 2:28:6:0:0 | 1:10:20:3:2 | 3:12:20:1:0 | NA | |||
| Jeong et al., 2021 [ | Intervention | 58.8 ± 5.4 | (10) 45.5% | Not specified (complete repair, type I,<5 cm) | NA | NA | NA | 17:05 | Not reported | Arthroscopic double-row transosseous equivalent (type I repair covering full footprint) |
| Control | 58.4 ± 6.5 | (12) 54.5% | NA | NA | NA | 14:08 | ||||
| Ji et al., 2023 [ | Intervention | 61.4 ± 9.2 | (27) 39.7% | A–P = 1.8 ± 0.68, M–L = 1.2 ± 0.50 | NA | NA | NA | 36:32 | ≥6 months failed conservative treatment | Arthroscopic transtendon suture-bridge repair ± atelocollagen injection |
| Control | 61.9 ± 7.9 | (29) 42.6% | A–P = 1.8 ± 0.80, M–L = 1.1 ± 0.49 | NA | NA | NA | 30:38 | |||
| Kim et al., 2019 [ | Intervention | 59.8 ± 7.3 | (26) 42.6% | A–P = 1.93 ± 1.16, M–L = 2.46 ± 1.16 | 20:37:4:0:0 | 6:48:7:0:0 | 2:44:14:0:0 | NA | 20.5 ± 45.3 (I) / 9.5 ± 14.6 (C) | Arthroscopic suture-bridge repair with acromioplasty; injectable gel-type atelocollagen placed between bone and tendon |
| Control | 57.8 ± 8.1 | (31) 51.7 % | A–P = 1.96 ± 1.19 M–L = 2.43 ±1.35 | 17:43:0:0:0 | 12:41:6:0:1 | 12:32:13:2:1 | NA | |||
| Kim et al., 2024 [ | Intervention | 59.8 ± 9.0 | (92) 50.8% | A–P = 1.05 ± 0.56, M–L = 1.25 ± 0.72 | 119:54:5:1:2 | NA | 135:42:3:1 | NA | ≥3 months failed conservative treatment | Arthroscopic double-row suture bridge repair (DR-SB); 3 mL injectable atelocollagen at bone-tendon interface; biceps tenodesis/tenotomy as indicated |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Elbow and Forearm Trauma Treatment
Introduction and background
Rotator cuff (RC) tear is a common orthopedic condition, affecting up to one-fifth of the general population [1]. It can cause shoulder pain and impair its range of motion (ROM), manifesting more often in the elderly [2]. Arthroscopic repair has been used as the gold standard surgery for the management of RC tears [3]. However, the retear rate and non-healing of the tendon-bone interface remain a challenge postoperatively [4].
Various biologics and scaffold materials were explored alone or in combination with surgery to provide a biomechanical and biochemical regenerative environment, including platelet-derived growth factors, stem cells, and atelocollagen [5,6]. Collagen is a fundamental structural protein in mammalian connective tissues, forming a major component of the skin, bones, tendons, ligaments, and cartilage [7]. It is made from a triple helix of three polypeptide chains, called tropocollagen [8]. Atelocollagen is produced by enzymatic removal of the N- and C-terminal telopeptides from type-1 collagen, which are responsible for the component's immunogenicity [9]. Therefore, it is a good candidate as a biological scaffold for RC tear repair, with potential to enhance cell adhesion, proliferation, and extracellular matrix formation [10].
Atelocollagen can be produced in several forms, including injectable gels, sponges, and membrane scaffolds [11]. Studies have investigated the injection of atelocollagen into complete or partial RC tears, either alone or in combination with arthroscopic repair [12]. Kim et al. (2020) investigated atelocollagen at 0.5ml and 1ml doses as a conservative management for 94 patients with partial RC tear [13]. By magnetic resonance imaging (MRI), they found a decrease in tear size at six months in favor of atelocollagen groups. Moreover, they found a statistically significant improvement in the Constant Shoulder Score (CSS), the American Shoulder and Elbow Surgeons score (ASES), and the visual analog scale (VAS) pain score in the intervention groups at the final visit.
Furthermore, the use of atelocollagen in combination with arthroscopic repair has been explored by Aldhafian et al., who included 129 patients with a complete RC tear and compared arthroscopic repair alone with arthroscopic repair combined with atelocollagen or acellular dermal matrix (ADM) injection [14]. They observed improvements in the three groups at 12 months in VAS, ASES, and CSS. However, the difference among them was not statistically significant.
These conflicting findings regarding the beneficial effects of atelocollagen, alone or in combination with arthroscopic repair, in RC tears prompted us to conduct this meta-analysis. We aim to pool studies that include patients with partial or full RC tears undergoing arthroscopic repair with atelocollagen injection vs. surgery alone, and to evaluate their clinical and radiological outcomes.
Review
Methods
We performed this study following the methodologies outlined in the Cochrane Handbook of Systematic Reviews of Interventions [15]. Additionally, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were meticulously followed for a standardized reporting [16].
Literature Search
Our systematic search was done across various electronic databases, including PubMed, Scopus, Web of Science (WOS), and the Cochrane Library, up to 7 Oct 2025. Our search strategy consisted mainly of the following keywords: (rotator cuff OR rotator cuff tear OR rotator cuff repair OR rotator cuff injury OR supraspinatus tear OR infraspinatus tear OR subscapularis tear OR teres minor tear OR shoulder tendon tear) AND (collagen OR atelocollagen OR collagen augmentation OR collagen scaffold OR collagen implant OR collagen injection OR biologic augmentation).
Inclusion Criteria
We included randomized controlled trials (RCTs) and prospective and retrospective cohort studies that enrolled patients diagnosed with partial- or full-thickness RC tears by preoperative imaging or intraoperative arthroscopy. Moreover, studies must have used injectable or gel-type atelocollagen as an intervention in combination with arthroscopic rotator cuff repair. On the other hand, the control group was patients undergoing arthroscopic repair alone and on conservative management.
Exclusion Criteria
Studies that used patch-type or sheet-type atelocollagen were excluded. Additionally, we excluded studies that did not perform arthroscopy. Moreover, we extended our exclusion criteria to include non-human or in vitro studies, only abstracts, cross-sectional designs, case reports, case series, non-English studies, and inaccessible full-text articles.
Screening and Study Selection
The articles retrieved from the database search were uploaded to the Rayyan software, where we removed duplicates and screened titles and abstracts to identify relevant articles. Secondly, we conducted a full-text screening of the initially included articles to ensure they met our eligibility criteria. Citation analysis was performed last to identify additional relevant publications. Two authors were individually responsible for the screening process, with a third serving as a tiebreaker in the event of a conflict.
Quality Assessment
We evaluated the risk of bias (ROB) using the appropriate tool for each study design. We used the Revised Cochrane Risk of Bias (RoB 2) tool for RCTs, which assesses five key domains: randomization process, deviations from the protocol, missing data, outcome measurement, and results selection [17]. Additionally, cohort studies were assessed using the Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I) tool, which evaluates seven aspects related to confounding, participant selection, intervention selection and deviation, missing data, measurement of outcomes, and selection of the reported result [18]. Each domain was assessed according to the respective criteria of each tool to assign an overall judgment.
Data Extraction
Our summary sheet was based on extracting key characteristics from each study, including: study identification, country, study design, sample size, type of tear, form of atelocollagen used, comparator, follow-up duration, and imaging modality. Additionally, we collected patients' demographics, including mean age, sex distribution, tear size (anterior-posterior × medial-lateral, cm), Goutallier grade of fatty infiltration for each rotator cuff muscle, affected shoulder side, symptom duration, and surgical technique. Furthermore, the primary outcomes extracted were retear rate at final follow-up, defined radiologically as Sugaya classification types IV-V, and clinical outcomes, including pain intensity measured by the VAS at the endpoint and shoulder function at 12 months, assessed using the ASES score and the Korean Shoulder Score (KSS). Secondary outcomes included shoulder ROM parameters at 12 months, including forward flexion (or elevation), external rotation at the side, and internal rotation (measured as the highest vertebral level reached behind the back).
Statistical Analysis
Our analysis was conducted using the Review Manager software (RevMan 5.4). Categorical data were reported as risk ratios (RRs) and 95% confidence intervals (CIs), whereas continuous outcomes were reported as mean differences (MDs) and 95% CIs. Additionally, we assessed statistical heterogeneity using the I-squared (I2) and Chi-squared (Chi2) statistics, a forest plot, and a random-effects model for heterogeneous outcomes. Furthermore, we performed a subgroup analysis by tear type.
Results
Literature Search
We identified 3143 articles during the initial screening, of which we removed 1376 duplicates. The remaining articles underwent title and abstract screening, yielding 14 articles that met our predetermined criteria. Consequently, we retrieved the full texts of these articles, resulting in five included studies for the meta-analysis [14,19-22]. More details on the literature search and selection process are shown in Figure 1.
PRISMA flow diagram detailing the screening process of the included studiesReferences: [14,19–22]PRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of the Included Studies and Baseline Demographics
The five included studies were conducted in South Korea between 2019 and 2024, including one RCT and four retrospective cohort studies (Table 1). Across all studies, patients with partial- or full-thickness RC tears were treated with arthroscopic repair and intraoperative injection of gel-type I atelocollagen at the tendon-bone interface, in volumes ranging from 1 to 3 mL. In contrast, the control group did not receive collagen augmentation. All patients were adults, with a mean age of 58 to 63 years. Most studies report small- to medium-sized full-thickness supraspinatus tears in the right shoulder, with follow-up durations of 12 to 27 months. Moreover, patients' tears were within the range of repairable cuff pathology, with a mean tear length of 1-2 cm in the anteroposterior direction and 1-2.5 cm in the mediolateral direction. Additionally, minimal to moderate muscle atrophy was evident, with grades 0-2 predominating in the Goutallier classification (Table 2).
Quality of the Included Studies
According to the ROBINS-I tool, two studies were at serious risk, one at moderate risk, and one at low risk. Additionally, the fifth study was found to have some concerns under the ROB 2 criteria. Further demonstration is shown in Figures 2 and 3.
ROB summary for the RCT assessed using the RoB 2 toolReference: [19]ROB - risk of bias; RCT - randomized controlled trial
ROB assessment for cohort studies using the ROBINS-I tool References: [14,20–22]ROB - risk of bias; ROBINS-I - Risk Of Bias In Non-randomized Studies - of Interventions
Clinical Outcomes
Retear rate (radiologic outcome): Across four studies, the rate of retear in the atelocollagen group was lower than in the control group (25/308 vs. 33/299), having a 25% relative reduction. However, no statistically significant difference was found (RR=0.75 (95% CI: 0.45-1.24; p=0.25), Figure 4. Additionally, minimal heterogeneity was observed among the included studies (I²=12%).
Retear rate References: [14,19,21,22]
Pain assessment (VAS): The atelocollagen group showed a lower VAS score, but the difference was not statistically significant (MD=-0.31, 95% CI: -1.14 to 0.51, p=0.45; Figure 5). Additionally, marked heterogeneity was detected in the overall pooled results (I²=93%, p<0.00001). To resolve this heterogeneity, we subcategorized the VAS by the tear type. Patients with full-thickness tears also show a non-significant difference between groups (MD=-0.37, 95% CI: -1.50 to 0.75, p=0.51). Additionally, comparable results were found for the partial-thickness tear subgroup reported by Ji et al. (2023; MD=-0.07, 95% CI: -0.49 to 0.35, p=0.74).
Forest plot comparing VAS pain score References: [14,19-22]VAS - visual analog scale
Functional Scores at 12 Months
ASES score: The pooled analysis of four included studies revealed a non-significant difference in ASES score at 12 months between the atelocollagen and the control group (MD=-2.16, 95% CI: -4.45 to 0.13, p=0.06; Figure 6). Additionally, we found low heterogeneity among studies (I²=10%, p=0.34). Furthermore, full-thickness or partial-thickness tear subgroups were also statistically insignificant (MD=-2.33, 95% CI: -4.83 to 0.18, p=0.07, and MD=-1.30, 95% CI: -6.99 to 4.39, p=0.65, respectively).
Twelve-month comparison of the ASES score forest plotReferences: [14,19-21]ASES - American Shoulder and Elbow Surgeons
KSS score: Across three studies, the KSS score was comparable between the atelocollagen and the control groups (MD=0.26, 95% CI: -4.02 to 4.53, p=0.91; Figure 7). High heterogeneity was noticed over the pooled result (I²=72%, p=0.03). Moreover, the full-thickness or partial-thickness tear subgroups show statistical insignificance (MD=1.30 (95% CI: -5.75 to 8.35, p=0.72), and MD =-1.60 (95% CI: -5.38 to 2.18, p=0.41), respectively).
KSS score forest plot at 12 monthsReferences: [14,20,22]KSS - Korean Shoulder Score
Range of Motion (ROM) at 12 Months
Forward flexion:* *The atelocollagen group demonstrated a comparable improvement in flexion ROM (MD=-1.03°, 95% CI: -6.91 to 4.86°, p=0.73) (Figure 8). Also, significant heterogeneity was present (I²=82%, p=0.0007). Additionally, insignificance was noticed in the subgroups (MD=-2.62°, 95% CI: -9,39 to 4.14°, p=0.45 for full-thickness tear and MD=4.00°, 95% CI: -2.09 to 10.09°, p=0.20 for partial-thickness tear).
Forest plot of forward flexion comparison at 12 monthsReferences: [14,19-21]
External rotation: Slightly greater external rotation was observed, favoring the control group (MD=-0.86°, 95% CI: -5.94 to 4.21°). However, we did not observe statistical significance (p=0.74) (Figure 9). Additionally, significant heterogeneity was found (I²=70%, p=0.02). Subgroup analysis was also insignificant (MD=-1.16°, 95% CI: -7.40 to 5.09°, p=0.72 and MD=0.60°, 95% CI: -8.39 to 9.59°, p=0.90) for full-thickness and partial tear, respectively.
Forest plot of external rotation comparison at 12 monthsReferences: [14,19-21]
Internal rotation: A slightly greater internal rotation was observed in favor of the atelocollagen group, despite being insignificant statistically (MD=0.06, 95% CI: -0.43 to 0.55, p=0.81) (Figure 10). Additionally, the overall pooled results showed very low heterogeneity (I²=0%, p=0.86). Subgroup analysis also revealed no significant differences for either full-thickness tears (MD=0.05, 95% CI: -0.50 to 0.60, p=0.85) or partial-thickness tears (MD=0.10, 95% CI: -1.01 to 1.21, p=0.86).
Forest plot of internal rotation comparison at 12 monthsReferences: [14,19-21]
Discussion
In this study, we explored the potential benefits of atelocollagen augmentation in patients with repairable RC tears who are undergoing arthroscopic surgery. Across five included studies, we observed trends toward lower retear rates and higher VAS scores in favor of the atelocollagen group, although these differences did not reach statistical significance. This was also observed in the functional outcomes, including ASES and KSS scores at 12 months, which showed a potential benefit but were not statistically significant. Regarding shoulder mobility, we did not observe a substantial difference between the groups in forward flexion, external rotation, or internal rotation. Furthermore, subgroup analyses by tear type did not show an effect on the overall outcome, consistent with findings across different tears.
Although the pooled outcomes for retear rate, pain relief, and functional recovery were not statistically significant, the consistent trend of improvement with atelocollagen is clinically encouraging. The retear events, in particular, were found to be a major barrier to these operations, with retear risks of 20% and 40% even for small-to-medium tears [23]. Therefore, the observed trend toward reduced rates with atelocollagen (25% relative reduction) warrants continued investigation and larger trials to confirm, particularly given the homogeneity of the included studies on this outcome.
Additionally, the slightly inferior ROM results in the atelocollagen group can be explained by the transient postoperative stiffness resulting from atelocollagen's role in collagen deposition and remodeling at the tendon-bone interface [10]. Our findings, if longitudinally proved, could also suggest long-term durability despite the early restricted ROM.
Moreover, other qualities of atelocollagen support its potential therapeutic role. This is reflected in its excellent biocompatibility and minimal antigenicity, resulting from the removal of telopeptides and its purified type 1 collagen nature [10,24]. Moreover, we did not observe any adverse effects in the atelocollagen group across the included studies, reinforcing its potential as a long-term complement to conventional arthroscopic repair.
A critical aspect of our analysis was the distinction between full and partial-thickness tears. Ji et al., the only study with a partial tear population, reported slightly greater forward flexion and abduction at final follow-up (p<0.05), as well as increased tendon thickness on MRI at 6 and 12 months postoperatively [20]. However, the functional scores were comparable between the two groups, which suggests that atelocollagen can improve tendon healing quality, even when early functional outcomes appear equivalent. Moreover, the improvement in shoulder mobility could be explained by their inclusion of partial-thickness PASTA lesions, which may heal more readily and demonstrate early functional improvement, given the preservation of the native tendon.
Another key subgroup relied on Jeong et al., the only included RCT, which compared the combination of hyaluronic acid and atelocollagen to no injection [19]. They reported better results with the combination in terms of VAS and ASES scores, forward elevation, and external and internal rotation, although the differences were not statistically significant. Additionally, they did not find any retear events in the atelocollagen group, vs. 9.5% in the no-injection group. The discrepancy between these findings, our pooled analysis, and some of the included studies may have stemmed from the synergistic effect of hyaluronic acid, which could have aided in reducing inflammation and organizing the extracellular matrix during the healing process. Additionally, the study design, as the only RCT, may have reduced confounding and optimized the effect of standardized surgical and rehabilitation protocols on healing.
Other biologics were investigated to enhance tendon-to-bone healing in patients with RC tears. In this regard, Gill et al. recently conducted a meta-analysis of the combination of platelet-rich plasma (PRP) with arthroscopic repair across 22 studies, which matched our population and control [25]. They reported a significant reduction in pain at both 6 and 12 months (MD=0.34 (0.10-0.59) and MD=0.24 (0.03-0.44), respectively). This superiority in comparison with ours may have stemmed from the longer follow-ups, particularly given that our VAS was mainly measured shortly post-operatively. This was noted in their three-month VAS scores, which were not significant, as ours were (MD=-0.11 (-1.14, 0.93)). However, both biologics are thought to exert their pain relief through a shared mechanism. While PRP exerts its analgesic effects through the release of protease-activated receptor four peptides, atelocollagen is also believed to possess analgesic and anti-inflammatory properties similar to those of PRP [10,26]. Additionally, the fact that all the included studies injected atelocollagen at the tendon-bone interface intraoperatively, rather than in the subacromial space, may also have contributed to the pain reduction.
Similar to our findings, they did not find a significant difference between the PRP and control groups in ASES scores at 12 months. Moreover, the benefits of PRP were clearly evident in the reduction in retear rate observed at 25 months (MD=15.03). Compared with these findings, our pooled analysis of the retear rate suggests a trend toward favoring atelocollagen, although the difference is not statistically significant. However, the number of included studies and the limited statistical power in our analysis can explain this difference.
Acellular collagen matrix patch (ACMP) was also explored in conjunction with arthroscopy and found to outperform arthroscopy alone in retear rate and ASES, as reported in a meta-analysis of five RCTs (p<0.05) [27]. The mechanistic approach of each intervention can explain the difference between our study and theirs. While atelocollagen provides biochemical support, ACMP offers mechanical and structural support. Moreover, the majority of our studies were cohort studies, unlike the RCTs' inclusion criteria, which could have influenced the outcomes.
Another report by Warren et al. investigated the bioinductive patch across 13 clinical studies and found significant improvements in ASES and VAS pain scores, with final ASES scores increasing from approximately 45-50 preoperatively to 83-96 postoperatively and VAS decreasing from five to seven to around one [28]. Moreover, the overall retear rate was notably lower (8.3% for full-thickness and 1.1% for partial-thickness repairs) compared to standard arthroscopic repair. The results of this study could also be attributed to the nature of the bioinductive patch, which provides mechanical reinforcement and serves as a biological scaffold. At the same time, atelocollagen is a biochemical stimulus that enhances cellular healing without providing structural support or strength.
To our knowledge, this is the first systematic review and meta-analysis to investigate the efficacy of atelocollagen administration in arthroscopic RC tears. We included studies with comparable surgical techniques, follow-up durations, and outcome measures, thereby providing some homogeneity among the included studies. However, we acknowledge several limitations. First, the low sample size stemming from limited evidence may have reduced the statistical power. Therefore, it prevented the detection of subtle but clinically meaningful differences between the groups. Second, including only one RCT may have introduced selection and performance biases. Third, the differences in tear sizes may have decreased the direct comparability among studies. Fourth, all included studies were performed in South Korea, limiting our ability to generalize the findings to other populations and care settings. Finally, variations in dosage and form, as well as inconsistencies in rehabilitation protocols, may have impacted the net outcome.
Conclusions
This systematic review and meta-analysis evaluated the efficacy of injectable atelocollagen as an adjunct to arthroscopic rotator cuff repair in patients with partial- or full-thickness tears. While our pooled analysis did not demonstrate statistically significant differences, consistent trends favoring atelocollagen were observed across retear rates, postoperative pain, and functional outcomes. The lack of statistical significance may be attributed to the limited available studies, small sample sizes, and heterogeneity in surgical protocols. Despite these limitations, the directional consistency of findings, combined with atelocollagen's biological properties supporting tendon-bone healing through enhanced cell adhesion and extracellular matrix formation, suggests potential clinical utility. Large-scale, multicenter randomized controlled trials with standardized protocols and longer follow-up periods are essential to definitively establish the clinical benefits of atelocollagen in rotator cuff repair and identify patients most likely to benefit from this intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence and risk factors of a rotator cuff tear in the general population J Shoulder Elbow Surg Yamamoto A Takagishi K Osawa T Yanagawa T Nakajima D Shitara H Kobayashi T 1161201920101954077710.1016/j.jse.2009.04.006 · doi ↗ · pubmed ↗
- 2Management of rotator cuff tears in the elderly population Maturitas Micallef J Pandya J Low AK 91412320193102768410.1016/j.maturitas.2019.01.016 · doi ↗ · pubmed ↗
- 3Long-term results of arthroscopic rotator cuff repair: initial tear size matters: a prospective study on clinical and radiological results at a minimum follow-up of 10 years Am J Sports Med Randelli PS Menon A Nocerino E 265926694720193141189910.1177/0363546519865529 · doi ↗ · pubmed ↗
- 4Biological augmentation strategies in rotator cuff repair Med Glas (Zenica) Özdemir E Karaguven D Turhan E Huri G 1861911820213326958210.17392/1305-21 · doi ↗ · pubmed ↗
- 5Current biological strategies to enhance surgical treatment for rotator cuff repair Front Bioeng Biotechnol Zhang C Wu J Li X Wang Z Lu WW Wong TM 657584920213417895710.3389/fbioe.2021.657584 PMC 8226184 · doi ↗ · pubmed ↗
- 6Biologics for rotator cuff repair: a critical analysis review JBJS Rev Smith KM Le AD Costouros JG Dragoo JL 06201810.2106/JBJS.RVW.17.0018530362970 · doi ↗ · pubmed ↗
- 7Enigmatic insight into collagen J Oral Maxillofac Pathol Deshmukh SN Dive AM Moharil R Munde P 2762832020162760182310.4103/0973-029X.185932 PMC 4989561 · doi ↗ · pubmed ↗
- 8Structure, stability and folding of the collagen triple helix Collagen Engel J Bächinger HP 733Springer 2005