Comprehensive geriatric assessment and primary care based interventions for managing frailty in older adults: An evidence map
Smiteerekha Sahoo, Tanveer Rehman, Md Shaney Ali, Haimanti Bhattacharya, Kavitha AK, Rasmiranjan Nayak, Ashok Kumar Mahakuda, Sanghamitra Pati, Jaya Singh Kshatri

TL;DR
This study maps evidence on primary care interventions for managing frailty in older adults, finding that multicomponent approaches in community settings are most effective.
Contribution
The study provides an evidence map highlighting multicomponent interventions and identifies gaps in evidence from low- and middle-income countries.
Findings
Multicomponent interventions combining physical, nutritional, and cognitive strategies are effective in managing frailty.
Community and home-based interventions are most commonly used but evidence quality varies significantly.
Most studies are from high-income countries, limiting generalizability to low- and middle-income settings.
Abstract
•Multicomponent interventions were associated with higher effectiveness in managing frailty.•Community and home-based interventions were found to be extensively used among different studies.•Prominence of low rated evidence and lack of evidence from Low- and middle-Income countries (LMICs) was found. Multicomponent interventions were associated with higher effectiveness in managing frailty. Community and home-based interventions were found to be extensively used among different studies. Prominence of low rated evidence and lack of evidence from Low- and middle-Income countries (LMICs) was found. Frailty is a geriatric syndrome leading to adverse health outcomes, but can be managed through targeted interventions and potentially reversed. Primary care settings play a pivotal role in identifying and addressing frailty. This review aims to assess the effective primary care interventions…
Click any figure to enlarge with its caption.
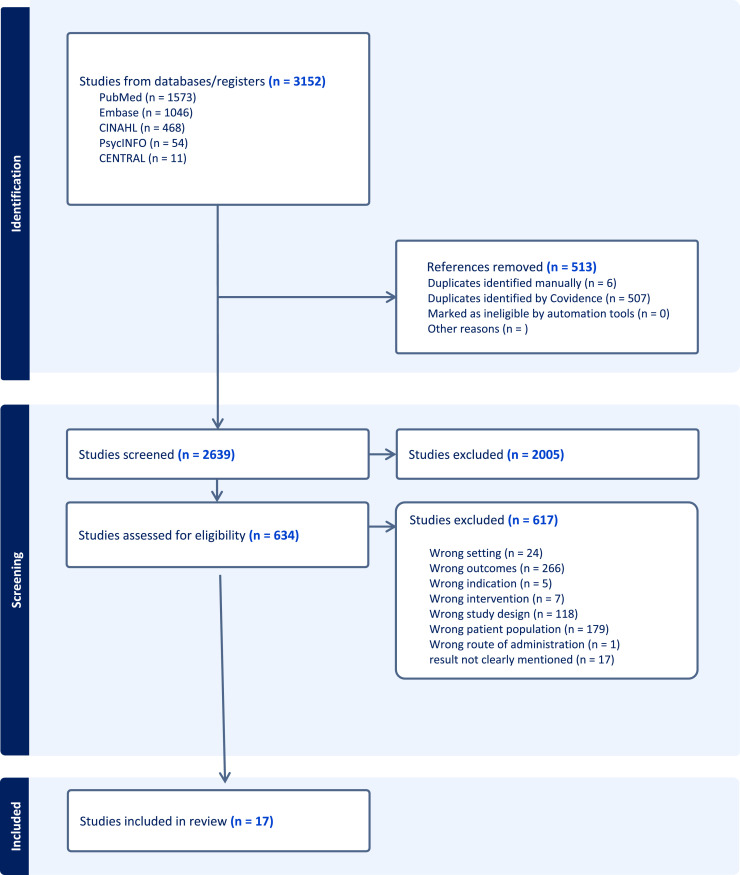 Figure 1
Figure 1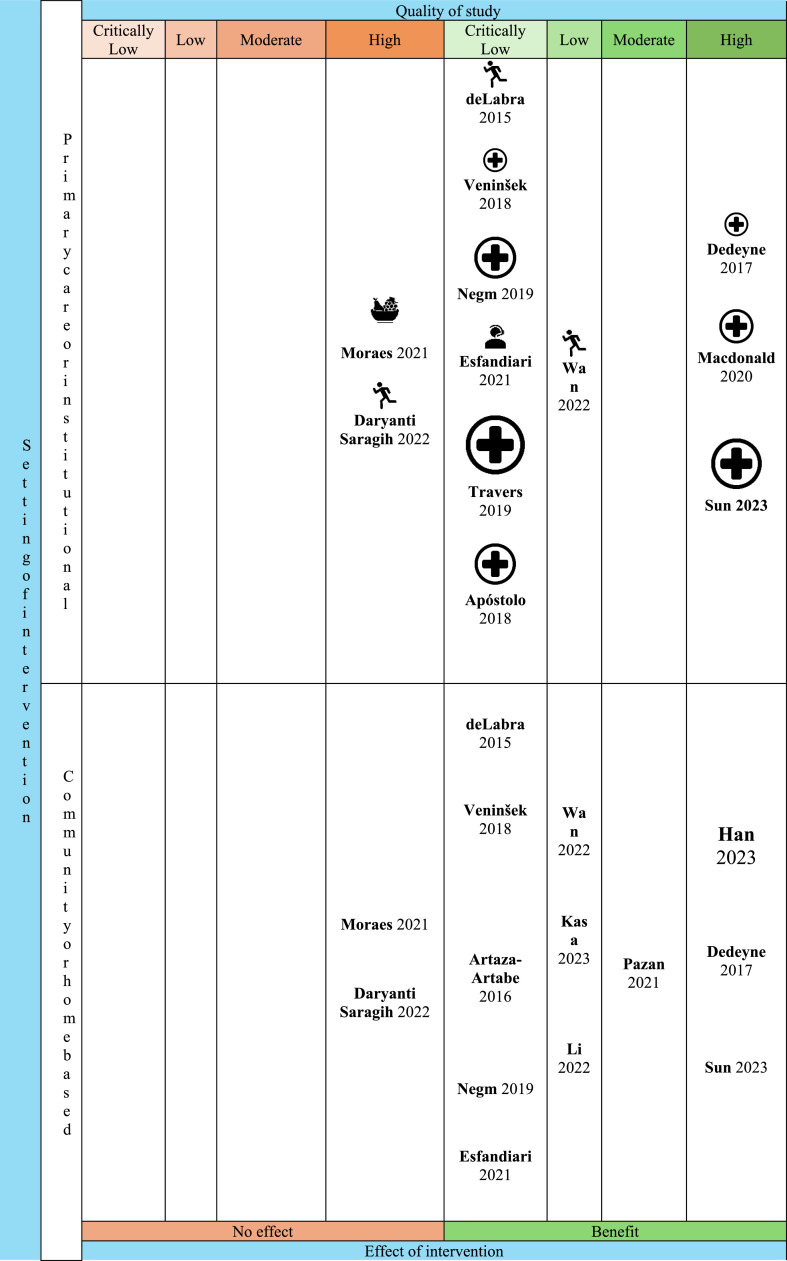 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Chronic Disease Management Strategies · Nutrition and Health in Aging
Introduction
1
Frailty is a common condition in older adults, marked by heightened vulnerability and deterioration across several physiological systems [1]. This condition greatly affects the health, autonomy, and overall quality of life of older adults, frequently resulting in negative outcomes such as falls, hospital admissions, institutional care, and even death. Worldwide, frailty is responsible for nearly 19 % of the total Disability-Adjusted Life Years (DALYs) in people aged 70 and above, highlighting its significant role in the global disease burden [2].
The prevalence of frailty differs significantly across various regions and settings, impacting between 4.0 % and 59.1 % of older adults living in the community-dwelling older adult [3], with prevalence ranging from 19.0 % to 75.6 % among those in nursing homes or hospital settings [4]. The challenge is even greater in low- and middle-income countries (LMICs), where older populations face a significantly higher rate of frailty due to unequal healthcare access, socioeconomic inequalities, and the combined impact of communicable and non-communicable diseases [5,6]. In LMICs, frailty prevalence can reach as high as 35.9 % % in certain age groups, compared to 9.9 −13.6 % % in high-income countries (HICs) [7]. This disparity poses significant challenges for healthcare systems in LMICs, where resources are already stretched thin [8].
Although frailty is a serious condition, it is not an unavoidable outcome of aging. With appropriate and timely interventions, frailty can be delayed, reduced, or even reversed. Among the most effective strategies are physical exercise and nutritional support, including protein-enriched diets [9,10]. Physical exercise, particularly resistance and strength training, improves muscle mass, physical performance, and mobility. Nutritional programs, particularly those targeting malnourished older adults, have demonstrated improvements in functional outcomes and quality of life [11]. A multi-dimensional approach, incorporating medical, psychological, and social assessments, allows for the identification and management of frailty in a comprehensive and organized manner [12]. Studies report a 22 % improvement in functional independence among older adults undergoing Comprehensive Geriatric Assessment-based interventions [13]. Addressing social isolation and mental health through community engagement programs and counselling services has shown promising results in enhancing overall well-being and resilience among older adults. However, the effectiveness of these interventions varies by population and context, underscoring the need for tailored approaches. A holistic strategy combining physical, nutritional, and social interventions has demonstrated the greatest potential in managing frailty [14,15].
Primary care is ideally placed to tackle frailty, as it serves as the initial point of contact for the majority of older adults within the healthcare system. Using validated screening tools such as the Fried Phenotype Scale, Frailty Index, FRAIL scale, Edmonton Frailty Scale, and Clinical Frailty Scale, frailty can be identified early [16]. By integrating physical, nutritional, and psychosocial interventions into routine care, primary care practices can provide personalized and accessible solutions to manage frailty effectively [17]. Primary care settings are ideal for implementing community-driven initiatives, particularly important in LMICs where access to specialized care is limited [18]. Embedding frailty management into routine primary care practices enhances accessibility, implementation, and sustainability [[19], [20], [21]]. Despite its potential, significant gaps remain in the adoption and implementation of frailty interventions within primary care settings [22]. Fewer than a majority of primary care providers routinely screen for frailty, and even fewer incorporate tailored interventions into practice [16]. Therefore, our goal was to address these gaps by identifying and assessing primary care-based interventions for managing frailty in older adults aged 60 and above. We systematically reviewed existing interventions and summarized their effectiveness in enhancing both clinical outcomes and patient-reported experiences.
Materials and methods
2
Protocol registration
2.1
This protocol of this study was preregistered on the Open Science Framework (OSF) and is under an embargo to prevent scooping. It will be made public upon acceptance or publication. A view-only link will be made available with the journal editor to facilitate peer review and collaboration.
Study design
2.2
Following the framework of evidence gap maps, we constructed an evidence map that integrates user-friendly visual figures, interactive graphs, and searchable databases to enhance the utility of the findings. Similar approaches have been used in health by the International Initiative for Impact Evaluation (3ie), which has developed several EGMs focusing on interventions such as anaemia programs in low- and middle-income countries and performance measurement and management in primary care delivery systems [23].
Eligibility criteria
2.3
We included systematic reviews (with or without meta-analysis) that focused solely on Randomized Controlled Trials involving older adults (aged 60 years or older). Interventions implemented in primary care, community-based, or home-based settings, aimed at addressing frailty and measuring outcomes related to its reduction or improvement, were considered. Studies involving hospitalized or bedridden individuals were excluded, as were reviews that focused on specific patient groups, such as surgical patients, oncology cases, or those receiving palliative care.
Search strategy
2.4
A comprehensive literature search was performed in the following databases: MEDLINE (via PubMed), Embase, CINAHL, PsycINFO, and the Cochrane CENTRAL library. We utilized various search terms related to "Frailty" and "Systematic review" / "Meta-analysis" alongside appropriate headings. The search was conducted to include articles published up until September 11, 2024. Detailed search strategies for each database are provided as supplementary material. (Supplementary File 1)
Study selection
2.5
Following a calibration exercise, two reviewers (RN, AM) independently screened the search results to identify potentially eligible records based on title and abstract. Then, two reviewers (HB, AK) independently verified eligibility by reviewing the full-text articles of the selected records. In the event of disagreements, consensus was achieved through discussion or by involving a third reviewer (JSK). The article selection process was managed using Covidence© (www.covidence.org). Throughout the screening process, a team of experienced researchers (JSK, TR) ensured consistency among reviewers and offered assistance as needed.
Data extraction
2.6
Data was systematically extracted using a pre-designed spreadsheet to capture key details of each review, including characteristics of included systematic reviews (e.g., population demographics, geographical location), study settings (e.g., primary care, community-based, or home-based), types of interventions (e.g., physical, nutritional, pharmacological, e-health, or multi-component) and measured outcomes (e.g., frailty reduction, physical function), with comparators, effect sizes, and statistical significance of outcomes. The completed data extraction forms are available as supplementary files.
Assessment of the quality of included reviews
2.7
The methodological quality of the systematic reviews was evaluated using the AMSTAR 2 checklist, which emphasizes seven critical domains (listed below) that can significantly impact the validity of a review and its conclusions, along with nine noncritical domains [21].
- •Protocol registered prior to the commencement of the review (item 2)
- •Adequacy of the literature search (item 4)
- •Justification for excluding individual studies (item 7)
- •Risk of bias from studies included in the review (item 9)
- •Appropriateness of meta-analytic methods (item 11)
- •Consideration of risk of bias when interpreting the review results (item 13)
- •Assessment of the presence and potential impact of publication bias (item 15)
Based on these criteria, the study quality in the results of each review was rated as high, moderate, low, or critically low [21]. A "high" rating indicated that there was no or only one non-critical weakness, providing a thorough and accurate summary of the available studies. A "moderate" rating was given when there were multiple non-critical weaknesses but no critical flaws, resulting in a reasonably accurate summary. Reviews with one critical flaw, regardless of the presence of non-critical weaknesses, were rated as "low," suggesting potential concerns regarding reliability [21]. Reviews with more than one critical flaw were deemed to have "critically low" study quality, making them unreliable for accurate synthesis of the evidence.
Evidence map
2.8
The evidence map categorized interventions based on:
- •Setting:
- ○Primary Care or Institutional Settings: Formal healthcare institutions such as clinics or hospitals.
- ○Community or Home-Based Settings: Interventions delivered outside institutional settings.
- •Outcomes:
- ○No Effect: Interventions that did not demonstrate a statistically significant impact on frailty outcomes
- ○Benefit: Interventions that yielded significant improvements in frailty-related outcomes.
The map used intuitive icons to represent the types of interventions, including physical (e.g., exercise programs), nutritional (e.g., protein supplementation), pharmacological, E-Health or Telemedicine and multicomponent interventions.
Results
3
The database searches yielded a total of 3152 studies. After deduplication and title/abstract screening, 634 studies underwent full-text evaluation, leading to the exclusion of 617 studies for various reasons, as depicted in the PRISMA flow chart (Fig. 1). In the end, 17 studies fulfilled all eligibility criteria and were included in the final analysis.Fig. 1PRISMA diagram for evidence gap map synthesis.Fig 1
Table 1 outlines the characteristics of the included systematic reviews. There were six high-rated reviews based on the AMSTAR 2 critical domains checklist [[24], [25], [26], [27], [28], [29]]. There was one moderate-rated review that exhibited non-critical weaknesses, such as limited reporting detail on funding and heterogeneity of results of studies included, but it was still considered reasonably reliable [30]. Moreover, three Low-rated reviews presented critical flaws, potentially compromising the accuracy and comprehensiveness of their findings [[31], [32], [33]]. The remaining seven reviews were critically low-rated and possessed multiple critical weaknesses, indicating they should not be relied upon for decision-making [19,[34], [35], [36], [37], [38], [39]]. Further investigation into the specific items contributing to these ratings is warranted to understand each review's strengths and weaknesses fully. The reviews consisted of trials ranging from 4 included studies by Han and colleagues to 56 included studies by Sun and team [25,29]. Seven of these reviews conducted meta-analyses. The evidence reviewed was relatively recent, with search years spanning from 2015 to 2023. Most studies were conducted in HICs, reflecting a geographical bias in the available research.Table 1. Primary care-based interventions for managing frailty among older adults.Table 1. Sl. No.Study IDStudies IncludedParticipantsMeta-AnalysisYear of SearchCountriesStudy Quality1deLabra 201591067No2015HICs; LMICsCritically Low2Li 2022133176Yes2021HICs; LMICsLow3Dedeyne 201781122No2016HICsHigh4Han 20234205No2023HICsHigh5Macdonald 2020314794Yes2019HICsHigh6Veninšek 201827151No2017HICsCritically Low7Artaza-Artabe 20163250,056No2016HICs; LICsCritically Low8Moraes 2021191564Yes2019HICs; LMICsHigh9Kasa 202362297No2022HICsLow10Negm 2019215262Yes2016HICsCritically Low11Esfandiari 2021121819Yes2020HICsCritically Low12Daryanti Saragih 2022151294Yes2021HICs; LMICsHigh13Wan 2022121123Yes2022HICsLow14Travers 20194615,690No2017HICs; LMICsCritically Low15Pazan 2021254954No2019HICsModerate16Sun 2023569530Yes2021HICs; LICsHigh17deLabra 2015215275No2015HICsCritically LowAbbreviations used: HMICs: High- and Middle-Income Countries; LICs: Low-Income Countries; LMICs: Low- and Middle-Income Countries.
Types of interventions
3.1
Table 2 provides an overview of the various interventions for frailty management, classified into five primary categories: physical, nutritional, pharmacological, e-health/telemedicine, and multicomponent approaches. Physical interventions (n = 4) primarily involved exercises designed to enhance muscle strength, balance, flexibility, and cardiovascular health. These interventions aimed to improve overall physical fitness and contribute to a reduction in frailty. Nutritional interventions (n = 1) focused on dietary supplementation, such as protein and vitamins, to address nutritional deficiencies and promote muscle strength, immune support, and general health—all critical components in managing frailty. Pharmacological interventions (n = 1) utilized medications or supplements to manage deficiencies, optimize health conditions, and address chronic illnesses that exacerbate frailty. E-health and telemedicine interventions (n = 2) leveraged digital tools, including mobile health applications, telemonitoring, telephone counselling, and video-guided home exercises. These digital approaches provided remote support and continuous care, making frailty management accessible even to those unable to attend in-person care. Lastly, multicomponent interventions (n = 9) combined various strategies, including physical exercises, nutritional support, cognitive and social engagement, comprehensive health assessments, and home safety modifications. These holistic approaches were the most extensively studied and demonstrated the most promising results for comprehensive frailty management.Table 2. Summary of findings for frailty management.Table 2. Sl. No.Study IDStudies IncludedParticipantsDescription of InterventionEffectiveness on Frailty Reduction (findings of SR)Outcome MeasuresMeta-Analysis Summary1deLabra 201591067Physical comprehensive training (leg extensions, hip flexions, double-arm pull downs, bicep curls).No impactFried’s frailty criteriaN/A2Li 2022133176Physical activity, exercise, fitness.SignificantCHS criteriaMD = −0.73 (95 % CI: −1.05 to −0.41)3Dedeyne 201781122Multidomain interventions: exercise, nutrition (protein, vitamins, milk fat, advice), hormones, cognitive, or psychosocial interventions.SignificantCHS criteriaN/A4Han 20234205E-health interventions: telephone counselling, home video exercise, telemonitoring, mobile health programs.No impactFried Frailty CriteriaN/A5Macdonald 2020314794Exercise with/without nutrition supplementation or education, comprehensive geriatric assessment.No impactFried Frailty CriteriaRR = 0.62 (95 % CI: 0.48 to 0.79)6Veninšek 201827151Multicomponent training: physical activity, vitamin D, home modification, cognitive training, nutrition.SignificantFrailty IndexN/A7Artaza-Artabe 20163250,056Protein intake, nutritional supplementation, vitamin D, exercise.No impactFried phenotypeN/A8Moraes 2021191564Nutritional education, protein/energy supplements, specific diets with other interventions.SignificantCHS criteriaOR = 2.30 (95 % CrI: 0.72 to 7.01)9Kasa 202362297Multicomponent intervention: face-to-face activities, telephone support, exercise, nutrition, cognitive training.No impactFrailty IndexN/A10Negm 2019215262Physical activity, nutrition supplementation, protein, comprehensive geriatric assessment.SignificantFrailty IndexSMD = −0.92 (95 % CI: −1.55 to −0.29)11Esfandiari 2021121819Remote health programs: phone, smartphone, tablet, computer, DVD.SignificantFried theoretical frameworkSMD = 0.31 (95 % CI: 0.15 to 0.47)12Daryanti Saragih 2022151294Resistance band exercises.SignificantFried phenotype scoreSMD = −0.29 (95 % CI: −0.55 to −0.03)13Wan 2022121123Baduanjin (Chinese exercise): warmup, main exercise, stretching.No impactFried phenotype scoreSMD = −1.46 (95 % CI: −2.39 to −0.53)14Travers 20194615,690Physical activity, health education, nutrition, home visits, hormone supplementation, counselling.No impactFried Frailty CriteriaN/A15Pazan 2021254954Pharmacological interventions or medication optimization.SignificantFried Frailty CriteriaN/A16Sun 2023569530Non-pharmacological interventions: mind-body exercise, mixed physical training, resistance, aerobic, cognitive training.No impactSUCRA criteriaSMD = 0.34 (95 % CI: 0.23–0.45)17Apóstolo 2018215275Home/group-based physical exercise, nutrition consultation, computerized balance training, protein-calorie/micronutrient supplementation.No impactCHS criteriaN/A
Effectiveness of interventions
3.2
The effectiveness of the interventions was evaluated based on their ability to reduce frailty, with outcomes classified as either beneficial or having no effect. Among the 17 studies reviewed, 15 reported significant benefits in reducing frailty, with multi-component interventions showing the most notable impact. Only two interventions demonstrated no significant effect, indicating the potential need for further optimization or more targeted implementation of specific approaches.
Settings of interventions
3.3
The interventions were delivered in two primary settings: primary care or institutional settings, and community or home-based settings. Primary care and institutional settings included formal healthcare environments such as clinics and hospitals. In contrast, community and home-based settings involved interventions implemented in familiar, everyday environments, which enabled personalized care and enhanced adherence. Most interventions were conducted in community or home-based settings, emphasizing the importance of accessible and convenient care integrated into daily living environments.
Gaps in evidence
3.4
The evidence map (Fig. 2) offers a comprehensive overview of interventions aimed at reducing frailty in older adults. It categorizes these interventions according to their type, setting, effectiveness, and the quality in the findings. While multi-component interventions consistently showed strong effectiveness, further evidence is especially needed to comprehend the impact of pharmacological and e-health interventions in LMIC settings.Fig. 2. Distribution of intervention effects across settings and quality of study (AMSTAR-2). The vertical axis delineates the intervention setting as either "Primary care or institutional" (upper section) or "Community or home based" (lower section). The horizontal axis represents the "Effect of intervention," ranging from "No effect" (left, orange shaded region) to "Benefit" (right, green shaded region). Each study is positioned within a grid cell according to its quality rating (Critically Low, Low, Moderate, High) and observed effect. The study label, showing the first author and publication year, is displayed next to an icon representing the intervention type (Physical, Nutritional, Pharmacological, E-health, Multicomponent). Icon size reflects total participants in the study to visually indicate study weight. Icon interpretation: Physical intervention Nutritional intervention Pharmacological Intervention E-health/Telemedicine Intervention Multicomponent Intervention.Fig 2
Quality of evidence
3.5
The quality of the included systematic reviews was evaluated using the AMSTAR 2 tool, revealing considerable variability in methodological rigor. Six reviews were rated as high quality of study, indicating reliable evidence with no or only one non-critical weakness. Three reviews received a moderate quality of study rating, with more non-critical weaknesses but no critical flaws. One review was rated as low quality of study due to a critical flaw, raising concerns about its reliability. The remaining seven reviews were rated as critically low quality of study, highlighting multiple critical flaws and significant limitations in their methodological soundness.
Discussion
4
Our study systematically mapped evidence on primary care-based interventions for managing (reducing or improving) frailty among older adults, identifying five categories of interventions: physical, nutritional, pharmacological, e-health, and multicomponent approaches. Multicomponent interventions emerged as the most effective, combining strategies to address the multifactorial nature of frailty. Interventions delivered in community or home-based settings were prominent, emphasizing accessibility. The findings highlight significant evidence gaps, particularly in LMICs, and underscore variability in the quality of the evidence.
The effectiveness of multicomponent interventions, integrating physical, nutritional, and cognitive components, was a key finding. These interventions align with literature from high-income settings, where studies have consistently demonstrated their ability to improve mobility, muscle strength, and reduce frailty-related outcomes [40,41]. However, a notable challenge is disentangling the individual contributions of each component within multicomponent approaches, making it difficult to optimize specific strategies. In LMICs, barriers such as limited healthcare resources and infrastructure necessitate research on simplified yet effective models of multicomponent interventions to ensure feasibility and scalability.
Community and home-based interventions featured prominently across the studies, highlighting their effectiveness and potential for improving accessibility and adherence [42]. Consistent with similar studies, these interventions leverage familiar environments to foster participant engagement and ensure continuity of care [36,43]. However, in LMICs, where home-based care is constrained by resource limitations and a lack of trained personnel, the scalability of such interventions remains a concern. Addressing these gaps through capacity-building efforts and leveraging technology, such as telemedicine, can enhance the reach of frailty interventions in underserved settings.
Physical and nutritional interventions were widely studied and consistently shown to reduce frailty [44], as seen in Liu et al. (2022), where strength and balance exercises significantly improved mobility and reduced fall risks [45,46]. However, inconsistencies arose in LMIC contexts, where challenges such as inadequate funding, poor nutritional security, and limited access to exercise facilities hinder implementation [33]. This shows a ‘know-do’ gap and implementation research is needed to fill this and adapt these interventions to the local context. Health system and policy research promoting multicomponent, community-based interventions could improve health outcomes for aging populations, particularly in resource-constrained settings. Scaling these interventions through programs like telemedicine and home-based care can bridge the healthcare access gap in rural and underserved regions [38].
The quality of evidence varied considerably, with many studies being rated as critically low according to the AMSTAR 2 tool. This finding aligns with previous reviews highlighting a lack of standardized methodologies in frailty research. While high-quality studies strengthen the evidence for the effectiveness of interventions, the predominance of lower-quality studies highlights the need for more rigorous research designs, improved reporting standards, and systematic evaluations. Enhanced methodological rigor will enable more reliable synthesis and stronger policy recommendations.
A key strength of this study is its use of evidence mapping, offering a clear and visual representation of the intervention landscape for frailty in primary care and community settings. The systematic approach to data extraction and quality assessment ensures the reliability of identifying effective interventions. Only systematic reviews were included in the mapping, ensuring that evidence already synthesized was considered. The quality of the studies varied, with many being rated as critically low. Most of the studies were conducted in high-income countries, limiting their applicability to low- and middle-income countries (LMICs). Furthermore, the diversity of interventions resulted in variability in outcomes.
Future research should focus on developing context-specific interventions for LMICs, with an emphasis on scalability and sustainability. Standardizing frailty definitions and outcome measures will enhance comparability and support more robust meta-analyses. Additionally, leveraging digital health innovations, such as telemedicine and mobile health applications, presents promising opportunities to expand access to frailty care, particularly in resource-constrained settings. Policymakers and health systems must prioritize the integration of evidence-based frailty interventions into primary care frameworks, as this approach has the potential to significantly reduce the burden of frailty and improve the quality of life for aging populations worldwide.
Conclusion
5
Multicomponent interventions combined with community-based care have proven effective in reducing frailty in high-income countries (HICs). Future initiatives should focus on adapting and scaling evidence-based multicomponent interventions in resource-limited settings to improve frailty outcomes and enhance the quality of life for older adults worldwide.
Funding
Multi Frame- funding: Intramural of ICMR.
Author contributions
The concept and design were handled by S.P., S.S., J.S.K., and T.R.: S.P., S.S., J.S.K., and T.R. monitored analysis and critical revision of the manuscript for important intellectual content; H.B, KAK., A.M., and M.S.A,R.N. were responsible for conceptualization, formal analysis, methodology, writing original draft preparation.
Ethical approval
Institutional review board statement
Multi Frame IEC number: Reference ICMR/IHEC-2024/015, Date:13/06/2024.
Data availability statement
All data from the study are available as an additional file.
CRediT authorship contribution statement
Smiteerekha Sahoo: Writing – original draft, Validation, Investigation, Formal analysis, Data curation. Tanveer Rehman: Writing – review & editing, Writing – original draft, Validation, Software, Methodology, Investigation, Conceptualization. Md Shaney Ali: Writing – review & editing, Validation. Haimanti Bhattacharya: Writing – review & editing, Investigation, Formal analysis. Kavitha AK: Resources, Methodology, Investigation, Data curation. Rasmiranjan Nayak: Validation, Methodology, Investigation. Ashok Kumar Mahakuda: Validation, Methodology, Investigation. Sanghamitra Pati: Writing – review & editing, Supervision, Conceptualization. Jaya Singh Kshatri: Writing – review & editing, Supervision, Resources, Methodology, Conceptualization.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
Jaya Singh Kshatri reports financial support was provided by Indian Council of Medical Research. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fried L.P.Ferrucci L.Darer J.Williamson J.D.Anderson G.Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care J Gerontol A Biol Sci Med Sci 5920042552631503131010.1093/gerona/59.3.m 255 · doi ↗ · pubmed ↗
- 2Beard J.R.Officer A.Carvalho I.A.The World report on ageing and health: a policy framework for healthy ageing Lancet 3872016214521542652023110.1016/S 0140-6736(15)00516-4PMC 4848186 · doi ↗ · pubmed ↗
- 3Collard R.M.Boter H.Schoevers R.A.Oude Voshaar R.C.Prevalence of frailty in community-dwelling older persons: a systematic review J Am Geriatr Soc 602012148714922288136710.1111/j.1532-5415.2012.04054.x · doi ↗ · pubmed ↗
- 4Liu W.Puts M.Jiang F.Zhou C.Tang S.Chen S.Physical frailty and its associated factors among elderly nursing home residents in China BMC Geriatr 2020202943280709810.1186/s 12877-020-01695-5PMC 7433121 · doi ↗ · pubmed ↗
- 5Fried L.P.Tangen C.M.Walston J.Frailty in older adults: evidence for a phenotype J Gerontol A Biol Sci Med Sci 562001 M 146M 1561125315610.1093/gerona/56.3.m 146 · doi ↗ · pubmed ↗
- 6Seligman B.Agarwal A.Bloom D.E.Frailty among older Indians: state-level factors Popul Ageing 172024149163
- 7Melo R.C.Cipolli G.C.Buarque G.L.A.Prevalence of frailty in Brazilian older adults: a systematic review and meta-analysis J Nutr Health Aging 2420207087163274456610.1007/s 12603-020-1398-0 · doi ↗ · pubmed ↗
- 8Clegg A.Young J.Iliffe S.Rikkert M.O.Rockwood K.Frailty in elderly people Lancet 38120137527622339524510.1016/S 0140-6736(12)62167-9PMC 4098658 · doi ↗ · pubmed ↗