Robotic-assisted minimally invasive transforaminal lumbar interbody fusion: A meta-analysis of perioperative and postoperative outcomes
Seif B. Altahtamouni, Loay A. Salman, Ahmad R. Al-Qudimat, Omar Fawaz Alnori

TL;DR
This study compares robotic-assisted minimally invasive spinal surgery with traditional methods and finds it reduces blood loss and hospital stays, though it takes longer.
Contribution
The study provides a meta-analysis of robotic-assisted minimally invasive TLIF outcomes, comparing them to conventional approaches.
Findings
Robotic-assisted surgery significantly reduces blood loss compared to open and conventional minimally invasive methods.
Hospital stays are shorter with robotic-assisted surgery, though operative time is longer.
Postoperative pain and functional outcomes show improvement trends but are not statistically significant.
Abstract
Degenerative lumbar spinal diseases are a leading cause of disability worldwide, often requiring surgical intervention when conservative management fails. Transforaminal lumbar interbody fusion (TLIF) is a commonly employed procedure to stabilize the spine and alleviate symptoms. This systematic review and meta-analysis aimed to test the safety and efficacy of robotic-assisted minimally invasive transforaminal lumbar interbody fusion (RA MIS-TLIF) in managing degenerative lumbar spinal diseases. Our primary objective was to compare the robotic approach with the conventional open or minimally invasive approach for TLIF regarding patients’ perioperative and postoperative outcomes. PubMed, Cochrane Library, Scopus, and Embase were searched from inception until October 2023. The selection criteria included only English-language articles focused on human participants aged 18 years and older…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
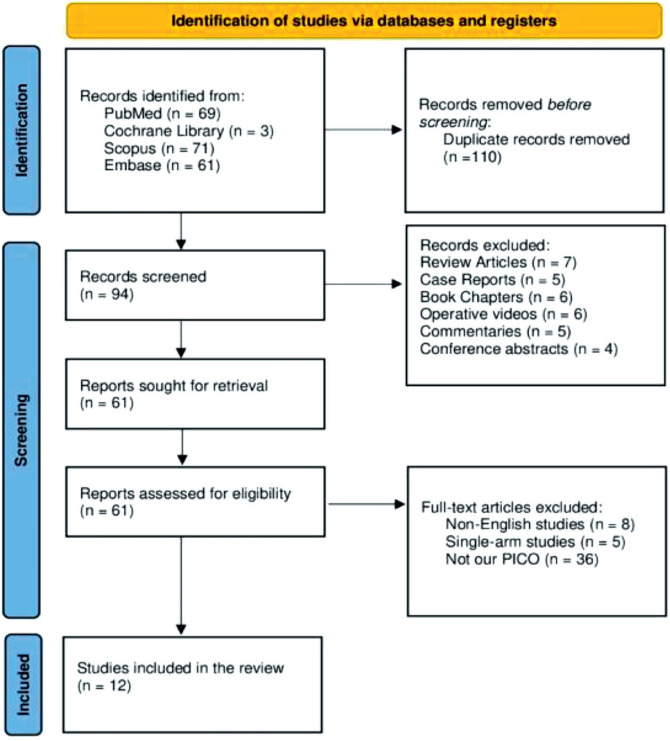 Figure 1
Figure 1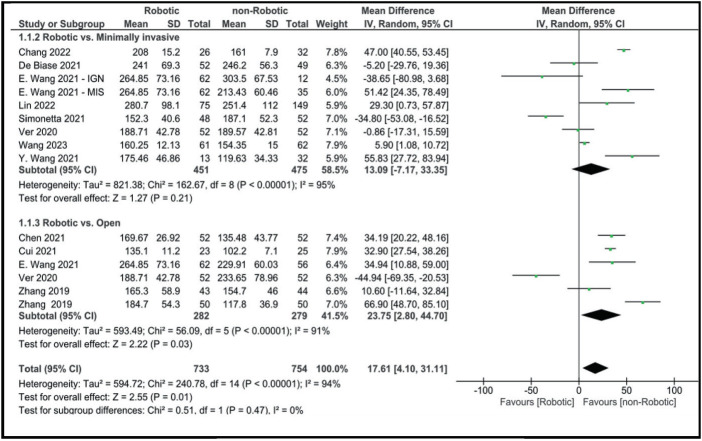 Figure 2
Figure 2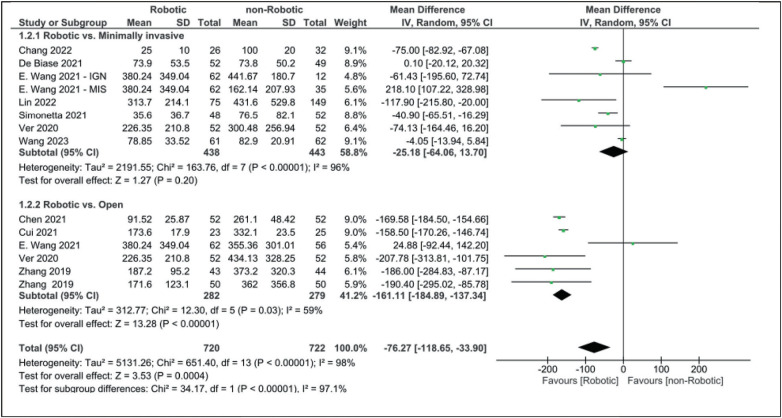 Figure 3
Figure 3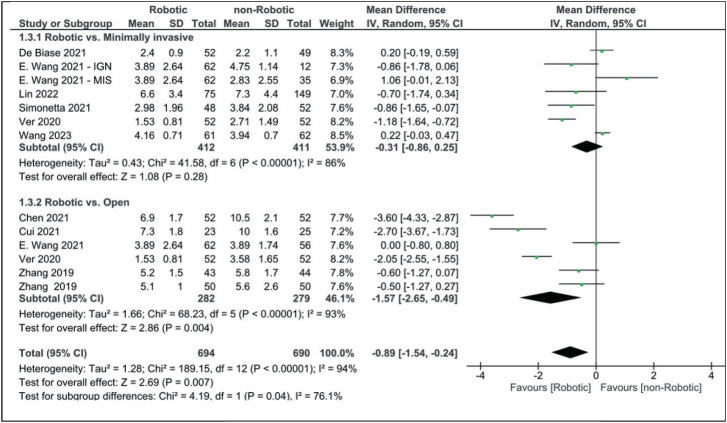 Figure 4
Figure 4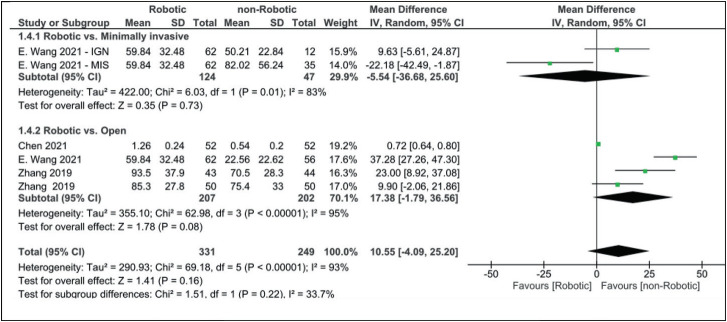 Figure 5
Figure 5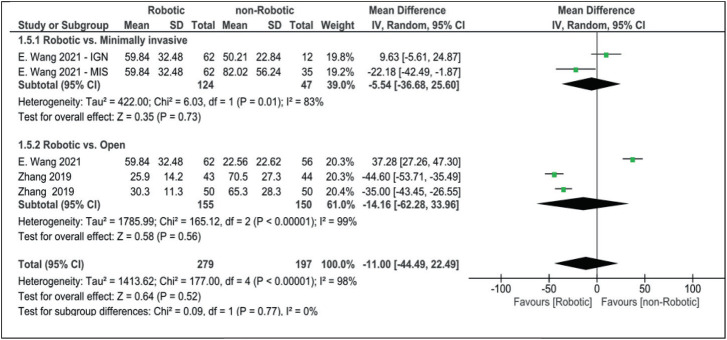 Figure 6
Figure 6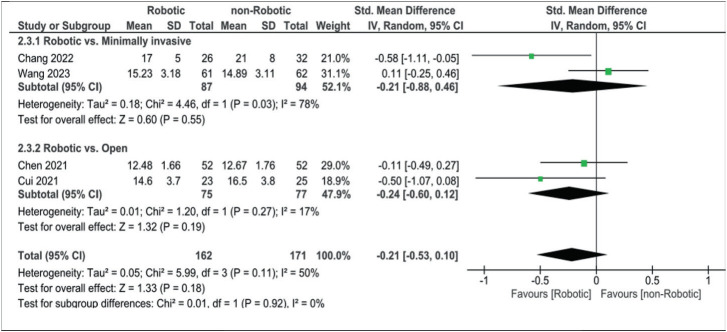 Figure 7
Figure 7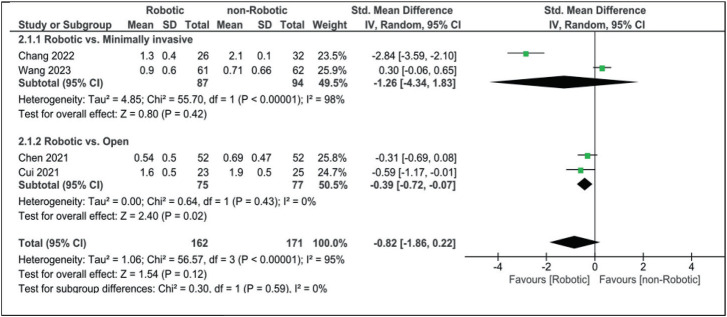 Figure 8
Figure 8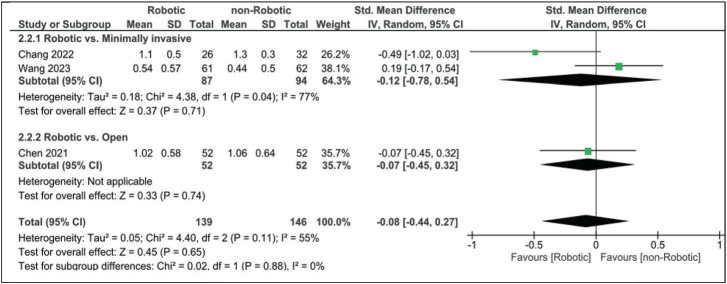 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Management of metastatic bone disease
1. INTRODUCTION
In recent years, lumbar degenerative diseases have been a significant concern in the medical field, which can be linked to the increased number of elderly populations worldwide.^1^ In 1982, Harms et al introduced open transforaminal lumbar interbody fusion (TLIF).^2^ Despite being widely used, the open technique introduced a series of challenges. Extensive paraspinal muscle detachment during a long midline incision can result in more soft tissue injury and longer hospital stays.^3^ As minimally invasive spinal surgery emerged, Seng C et al introduced minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) in 2002.^4^ This new technique aimed to minimize complications, blood loss, and hospitalization while achieving comparable outcomes to the open technique.^4–7^ However, MIS-TLIF showed inferiority to open TLIF in terms of operative time, learning curve, and higher risk of screw malposition and perforation, which can be attributed to the entry point’s indirect visual access.^8–12^ Moreover, MIS-TLIF was found to expose both patients and surgeons to excessive radiation due to the use of intraoperative fluoroscopy in most cases.^7,13–15^
To overcome the increased risk of screw malposition, new technologies, such as the use of an intraoperative navigation system in combination with the minimally invasive approach, have emerged.^16^ The use of navigation systems, including intraoperative computed tomography (CT) and 3D C-arm systems, enhanced the accuracy of pedicle screw placement compared to the traditional MIS-TLIF.^17–19^ Robotic guidance in spine surgery gained FDA approval in 2004 and has since gained attention among spine surgeons.^20–22^ Since then, several studies have demonstrated the advantages of robotic-assisted spine surgery, such as increased accuracy, decreased blood loss, and reduced radiation exposure to patients and surgeons.^23–25^ A meta-analysis by Fan et al found that the pedicle screw placement using the robotic technique was more accurate than the free-hand pedicle screw insertion.^26^
Although research in robotic-assisted surgery has advanced significantly, few studies have investigated patient outcomes in robotic-assisted minimally invasive transforaminal lumbar interbody fusion (RA MIS-TLIF). This meta-analysis aimed to test the safety and outcomes in patients with lumbar degenerative diseases who underwent RA MIS-TLIF.
2. MATERIALS AND METHODS
This systematic review was conducted in a stepwise manner in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and checklist.^27^ The protocol for this review was registered in PROSPERO (International Prospective Register of Systematic Reviews) under CRD42023488139.
2.1 Search Strategy
A thorough search was conducted through PubMed, Cochrane Library, Scopus, and Embase. The search process took place from inception until October 17, 2023. A combination of keywords and Medical Subject Headings (MeSH) Terms with two Boolean operators was used to extract relevant articles: Robotic OR robotic-assisted OR robot-assisted OR robotic-assisted OR robot-assisted OR “Robotic Surgical Procedures” [Mesh] AND minimally invasive transforaminal lumbar interbody fusion OR MI-TLIF OR TLIF OR transforaminal lumbar interbody fusion OR minimally invasive TLIF.
2.2 Inclusion/Exclusion Criteria
Articles included were retrospective or prospective studies that were highly relevant to the aim of this article, with the robotic approach being the primary investigated surgery type. The criteria used for the selection included articles written in the English language only, studies conducted on humans aged 18 years and above, and studies with clearly documented and measurable outcomes. Review articles, case reports, book chapters, videos, commentaries, and conference abstracts were excluded. Studies irrelevant to our research question, including single-arm studies, were also excluded. The selection of the studies to be included in the final evaluation and review was based on relevance and the above inclusion/exclusion criteria.
2.3 Study Selection and Data Extraction
Study selection was done by two independent reviewers (SBA and LAS) who screened the titles and abstracts to identify relevant articles. Potentially relevant articles were then subjected to full-text screening according to the PICO (population, intervention, comparator, and outcomes) question (Table 1) and based on relevance to the inclusion criteria, and only highly relevant articles were selected for the final evaluation. Year of publication, author, study design, sample size, participants’ age and body mass index, surgery type, and follow-up periods were extracted from the selected studies. Additionally, study outcomes were extracted for statistical analysis, including operative time, estimated blood loss, length of hospital stay, radiation time, radiation dose, and postoperative pain scores.
2.4 Quality Assessment/Appraisal
The methodological quality of the selected studies was critically assessed using the Methodological Index for Nonrandomized Studies (MINORS).^28^ The MINORS tool is a valid instrument for assessing the quality of comparative and non-comparative nonrandomized studies. It consists of 12 domains, with the first eight being for noncomparative studies. Each domain can be awarded 0, 1, or 2, with a maximum score of 24 and 16 for comparative and noncomparative studies, respectively.
2.5 Statistical Analysis
Review Manager (RevMan) 5.4 was used to conduct this statistical analysis. All data were continuous and reported as mean and standard deviation. The mean difference was used with operative time, estimated blood loss, length of hospital stays, and radiation time and dose, where the standardized mean difference was used in pain scores analysis. All data were analyzed using the inverse-variance method with a 95% confidence interval (CI). Heterogeneity was tested using the chi-square test and the I^2^ index. The random-effects model was used due to the heterogeneity found between the included articles (I^2^ >50٪).
RESULTS
3.1 Search Results
Our systematic search yielded a total of 204 articles. Of these, 110 duplicates were removed. The title and/or abstract of the remaining 94 articles were screened, and 33 were excluded. Sixty-one articles underwent full-text screening. Non-English studies, single-arm studies, and studies unrelated to our PICO question were excluded. Twelve eligible studies were included in this meta-analysis (Figure 1).
3.2 Study Characteristics
Twelve observational articles, including 1,385 patients, were included in this review (Table 2). Six studies were conducted in China, five in the United States, and one in Taiwan. Six articles compared robot-assisted minimally invasive lumbar interbody fusion with conventional minimally invasive interbody fusion, four compared the robotic approach with the conventional open approach, one compared robotic with minimally invasive, open, and image-guided navigation (IGN), one compared robotic to conventional and instrument-tracking minimally invasive surgery, and one compared robotic with either open or minimally invasive surgery.
3.3 Risk of Bias Assessment
Table 3 presents the scoring process for each study using the MINORS criteria. The studies included were scored between 17 and 22. Each study was evaluated against 12 domains and assigned a score between 0 and 2 for each domain, where 0 indicated that the domain was not reported, 1 indicated that the domain was reported but inadequately, and 2 indicated that the domain was reported and adequately. No studies were excluded from the analysis based on the MINORS criteria.
3.4 Perioperative Outcomes
According to our analysis, operative time was longer in the robotic approach than in the non-robotic approach (MD: 17.61 [95% CI, 4.10–31.11]; Figure 2). Operative time was also shorter in open surgery, with a mean difference of 23.75 (2.80, 44.70).
Compared to minimally invasive surgery, operative time was shorter than the robotic approach, although the results did not reach statistical significance (MD: 13.09 [95% CI, −7.17 to 33.35]). Blood loss was markedly higher in both open (MD: −161.11 [95% CI, −184.89 to −137.34]) and minimally invasive surgery (MD: −25.18 [95% CI, −64.06 to 13.70]) when compared to robotic-assisted surgery (Figure 3).
When comparing robotic and non-robotic surgeries, blood loss is less in robotic surgery with marked statistical significance (MD: −76.27 [95% CI, −118.65 to −33.90]). Patients who have undergone robotic-assisted surgery spent less time in the hospital than those who have undergone open (MD: −1.57 [95% CI, −2.65 to −0.49]) or minimally invasive surgery (MD: −0.31 [95% CI, −0.86 to 0.25]). The mean difference between robotic and non-robotic surgery in terms of hospital stay length was −0.89 (−1.54, −0.24), which appears to be reaching statistical significance (Figure 4).
Robotic-assisted surgery radiation time appeared to be longer than in minimally invasive surgery but shorter than the open approach, with a mean difference of −5.54 (−36.68, 25.60) and 17.38 (−1.79, 36.56), respectively (Figure 5).
Our analysis for radiation time did not reach statistical significance (robotic vs. non-robotic MD: 10.55 [95% CI, −4.09 to 25.20]). Only three articles examined the difference in the administered radiation dose between the robotic and non-robotic approaches. The radiation dose was slightly lower in the robotic group (MD: −11.00 [95% CI, −44.49 to 22.49]), although it did not reach statistical significance (Figure 6).
3.5 Postoperative Outcomes
Four articles commented on postoperative outcomes using the Oswestry Disability Index (ODI), visual analog scale (VAS) for low back pain, and VAS for leg pain. For ODI, our analysis revealed a standardized mean difference of −0.21 (−0.53, 0.10) when comparing robotic-assisted surgery with all non-robotic approaches, −0.24 (−0.60, 0.12) when comparing it to open alone, and −0.21 (−0.88, 0.46) when comparing it to minimally invasive surgery alone (Figure 7).
VAS for low back pain was slightly better in the robotic group than in both open and minimally invasive surgery groups (robotic vs. open SMD: −0.39 [95% CI, −0.72 to −0.07] and robotic vs. minimally invasive SMD: −1.26 [95% CI, −4.34 to 1.83]). When comparing robotics with non-robotic in general, VAS was still better among the robotic group (SMD: −0.82 [95% CI, −1.86 to 0.22]), although it did not reach statistical significance (Figure 8).
As for VAS for leg pain, results did not reach statistical significance, with slight differences between both groups (robotic vs. open SMD: −0.07 [−0.45, 0.32], robotic vs. minimally invasive SMD: −0.12 [−0.78, 0.54], and robotic vs. non-robotic SMD: −0.08 [−0.44, 0.27]; Figure 9).
4. DISCUSSION
We conducted a systematic review and meta-analysis of 12 observational studies involving 1385 patients to gain insight into the use of robotic-assisted surgery in patients suffering from lumbar degenerative diseases in terms of patients’ perioperative and postoperative outcomes. We found that robotic-assisted transforaminal lumbar interbody fusion (RA MIS-TLIF) shows promising results in terms of operative time, intraoperative blood loss, length of hospitalization, and radiation time and dose, with comparable postoperative outcomes to both open and minimally invasive TLIF.
Lumbar interbody fusion can be carried out using different approaches. Transforaminal interbody fusion is among the most common approaches, including open or minimally invasive surgery. Several studies have shown the superiority of MIS-TLIF over open TLIF. For example, hardware placement in MIS-TLIF is found to be more accurate than in open TLIF, which in turn can minimize soft tissue damage, perform bilateral decompression through a unilateral approach, and maintain stabilization of the posterior spinal segment.^41^ By minimizing damage and being more accurate with hardware placement and dissection, MIS-TLIF can help patients undergo less collateral trauma during surgery, resulting in improved surgical outcomes.^35^
Recently, the use of robotic systems with MIS-TLIF in treating lumbar degenerative diseases has become widely studied in the literature.^32,39,42–45^ This new approach has been adopted to assess surgeons in pedicle screw placement and make spine surgeries more efficient and safer.^46,47^ Another reason for the emergence of robotic-assisted surgery is the presumed ability to reduce radiation exposure for patients and surgeons, which is a major concern with minimally invasive surgeries.^48^ RA MIS-TLIF allows surgeons to be more accurate and precise,^42^ and without the need to expose anatomical markers to determine an entry point, direction, and length of pedicle screws, which decreases muscle damage.^31^ These factors can reflect early ambulation after surgery, which lowers the rate of complications related to prolonged bed rest.^31^ Furthermore, due to its high precision, the revision rate following RA MIS-TLIF can be lower than other surgical approaches.^49^
Although some studies reported no difference between the RA technique and freehand technique in terms of operative time,^50^ most studies found an increase in operative time in the RA technique.^51–53^ A systematic review by Ghasem et al found increased operative time during surgeries that used robotic guidance.^54^ An increase in operative time in the RA MIT-TLIF surgery compared to either open or minimally invasive surgery in previous articles aligns with our findings (MD: 17.61 [95% CI, 4.10–31.11]). This increase in operative time can be explained by several reasons, including the need for more intraoperative preparation and usage of the robot system and the initial learning curve for the procedure.^29^ On the other hand, estimated blood loss along with the length of hospital stay was found to be significantly lower in the robotic group in our analysis (MD: −76.27 [95% CI, −118.65 to −33.90] and MD: 0.89 [−1.54 to −0.24], respectively). This can be explained by the lack of dissection while using the robotic arm, which allows the surgeon to only incise the skin and fascia, limiting further tissue damage.^55^ Previous studies have also demonstrated that RA MIS-TLIF can induce fast recovery, lowering hospital stays and costs.^56,57^ In our analysis, VAS scores for leg and lower back pain, in addition to ODI scores after at least 12 months, were comparable between robotic and non-robotic approaches. However, some studies show that patients in robotic groups showed better scores one month after surgery.^30^
Despite the high hopes of robotic-assisted spine surgery, its limitations and obstacles must be recognized. One of the leading concerns is the economic aspect. Robotic systems are expensive, require ongoing maintenance, and are operated by surgical teams needing special training. These costs may impede accessibility and uptake, especially in low-resource settings or smaller sub-sector facilities.^58,59^ Longer operative time might also be associated with higher costs related to health care resources and lower operating room efficiency, especially at the start of implementation.^54^ Additionally, the learning curve for robotic-assisted surgery remains a significant hurdle. Although several reports have suggested that surgeons’ learning curve for robotic-assisted procedures may not be too steep,^31,32^ up to 20 to 40 cases have been reported to be necessary to ensure enough procedural success.^59–64^ Such variability could affect surgery’s performance in the early learning curve. Of note, even though robotic systems are generally thought to decrease the radiation the surgical team is exposed to, we could not find any statistical difference in our meta-analysis in radiation time or dose between the robotic approach and traditional devices. Hence, the assumed advantage in this area may not be universal among all clinical setups or robotic systems.^25,30,39,50^
4.1 Limitations
To our knowledge, this is the first meta-analysis testing patients’ outcomes after robotic-assisted surgeries for lumbar degenerative diseases. Our study has limitations, including the retrospective and prospective design of the included studies, which inherently introduce a degree of bias to our analysis. The small sample size across all studies also limits the accuracy of our results. Another important limitation is the heterogeneity in the results of the studied variables, which lowered the degree of evidence. Furthermore, the introduction of subgroups did not reduce the heterogeneity.
5. CONCLUSION
This meta-analysis shows promising results for the use of robotic-assisted surgery in the management of lumbar degenerative diseases in terms of operative time, estimated blood loss, and length of hospital stay, with slightly better results regarding radiation time and dose and comparable postoperative outcomes to both minimally invasive and open transforaminal lumbar interbody fusion.
AVAILABILITY OF DATA, CODE, AND MATERIALS
Available upon request.
ETHICS APPROVAL
No ethical approval is required.
AUTHOR CONTRIBUTIONS
All authors contributed to the study’s conception and design. Material preparation, literature review, data collection, and quality assessment were performed by SBA and LAS. Statistical analysis was performed by SBA. The first draft of the manuscript was written by SBA, and all authors commented on previous versions of the manuscript. All authors read and approved of the final manuscript.
CONFLICT OF INTEREST
The authors have no relevant financial or non-financial interests to disclose. The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fehlings MG Tetreault L Nater A Choma T Harrop J Mroz T The aging of the global population: the changing epidemiology of disease and spinal disorders Neurosurgery 2015 Oct;77 Suppl 4:S 1–510.1227/NEU.000000000000095326378347 · doi ↗ · pubmed ↗
- 2Harms J Rolinger H[A one-stage procedure in the operative treatment of spondylolistheses: dorsal traction-reposition and anterior fusion (author’s transl)]Z Orthop Ihre Grenzgeb 1982 May-Jun;120343–710.1055/s-2008-10516247113376 · doi ↗ · pubmed ↗
- 3Grob D Surgery for degenerative lumbar disease: transforaminal lumbar interbody fusion Eur Spine J 2009 Dec;18(12):1991–210.1007/s 00586-009-1222-319937352 PMC 7571503 · doi ↗ · pubmed ↗
- 4Seng C Siddiqui MA Wong KP Zhang K Yeo W Tan SB Five-year outcomes of minimally invasive versus open transforaminal lumbar interbody fusion: a matched-pair comparison study Spine (Phila Pa 1976)2013 Nov;38(23):2049–5510.1097/BRS.0b 013e 3182 a 8212 d 23963015 · doi ↗ · pubmed ↗
- 5Goldstein CL Macwan K Sundararajan K Rampersaud YR Comparative outcomes of minimally invasive surgery for posterior lumbar fusion: a systematic review Clin Orthop Relat Res 2014 Jun;472(6):1727–173710.1007/s 11999-014-3465-524464507 PMC 4016464 · doi ↗ · pubmed ↗
- 6Wong AP Smith ZA Stadler JA 3rd Hu XY Yan JZ Li XF Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF): surgical technique, long-term 4-year prospective outcomes, and complications compared with an open TLIF cohort Neurosurg Clin N Am 2014 Apr;25(2):279–30410.1016/j.nec.2013.12.00724703447 · doi ↗ · pubmed ↗
- 7Tian NF Wu YS Zhang XL Minimally invasive versus open transforaminal lumbar interbody fusion: a meta-analysis based on the current evidence Eur Spine J 2013 Aug;22(8):1741–910.1007/s 00586-013-2747-z 23572345 PMC 3731475 · doi ↗ · pubmed ↗
- 8Sclafani JA Kim CW Complications associated with the initial learning curve of minimally invasive spine surgery: a systematic review Clin Orthop Relat Res 2014 Jun;472(6):1711–710.1007/s 11999-014-3495-z 24510358 PMC 4016470 · doi ↗ · pubmed ↗