A Study of the Clinico-Etiological Profile of Splenomegaly Among Children in a Tertiary Care Hospital
Kuppireddy Lakshmisindhu, Modalavalasa Sravanadurga, Noolu Ramalingeswara, Lanka Gowthami

TL;DR
This study examines the causes and clinical features of spleen enlargement in children at a hospital in coastal Andhra Pradesh, finding infections as the most common cause.
Contribution
The study provides region-specific insights into pediatric splenomegaly in coastal Andhra Pradesh, where prior data is limited.
Findings
Infections were the leading cause of splenomegaly in 55.7% of cases, with malaria, enteric fever, and tuberculosis being the main contributors.
Most children (85.2%) responded well to medical treatment, with only 4.3% requiring splenectomy and 1.7% mortality.
Male children and those under six years old were most commonly affected, with Grade III splenomegaly being the most frequent.
Abstract
Background Splenomegaly, or enlargement of the spleen, is a clinical sign rather than a standalone diagnosis, often indicating underlying systemic disease. In children, it may present due to a broad spectrum of conditions ranging from infections to hematologic, metabolic, or neoplastic disorders. The present study aimed to identify the etiological spectrum of splenomegaly among children admitted to the pediatric ward of a tertiary care hospital. The present study also sought to analyze the clinical profile, associated systemic findings, grading patterns, and assess treatment response and outcomes, thereby identifying region-specific trends that may guide early diagnosis and management strategies. Despite earlier studies addressing pediatric splenomegaly in different Indian populations, data from this coastal Andhra Pradesh region remain limited. Variations in endemic infection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
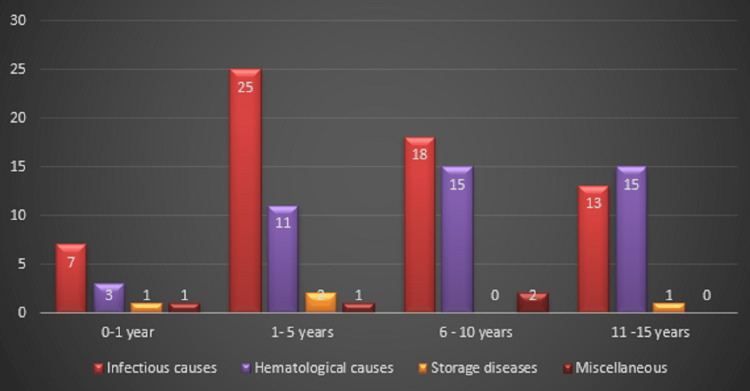 Figure 1
Figure 1| Grade | Clinical feature |
| Grade 0 | Spleen not palpable even on deep inspiration. |
| Grade 1 | Spleen palpable below costal margin, usually on deep inspiration |
| Grade 2 | Spleen palpable, but did not extend beyond a horizontal line midway between the costal margin and the umbilicus, measured along a vertical line dropped from the left nipple. |
| Grade 3 | Spleen palpable more than halfway to umbilicus, but not below a line horizontally running through it. |
| Grade 4 | Palpable below umbilicus but not below a horizontal line halfway between umbilicus and pubic symphysis. |
| Grade 5 | Extending lower than class IV |
| Grade | Clinical feature |
| Mild splenomegaly | 1-3 cm below left costal margin |
| Moderate splenomegaly | >3-7 cm below left costal margin |
| Massive (gross) splenomegaly | >7 cm below left costal margin |
| Age group | Male | Female | Total (n = 115) | Percentage (100%) |
| One month to one year | 8 | 4 | 12 | 10.43 |
| One to five years | 24 | 15 | 39 | 33.92 |
| Six to 10 years | 27 | 8 | 35 | 30.44 |
| 11-15 years | 14 | 15 | 29 | 25.21 |
| Symptom | Present study (n = 115) |
Kamble et al. [ |
Bricks et al. [ |
| Fever | 80 (70%) | 93 (75%) | 39 (43.8%) |
| Abdominal distension/pain | 34 (30%) | 34 (27.4%) | 13 (14.6%) |
| Bleeding tendencies | 11 (10%) | 7 (5.64%) | - |
| Jaundice | 9 (8%) | 39 (31.45%) | 14 (15.7%) |
| Weight loss/fatigue | 6 (5%) | - | 21 (24%) |
| Clinical sign | Present study (n = 115) | Kamble et al. [ | Bricks et al. [ | Major associated etiologies in present study |
| Pallor | 58 (50.4%) | 120 (97%) | 47 (53%) | Hematological disorders |
| Hepatomegaly | 42 (36.5%) | 111 (90%) | 89 (100%) | Infectious causes and storage disorders |
| Lymphadenopathy | 30 (26.1%) | 29 (23.38%) | 9 (10%) | Infectious and hematological causes |
| Icterus | 10 (8.7%) | 39 (31.45%) | 8 (9%) | Hepatic and hemolytic disorders |
| Bleeding manifestations | 12 (10.4%) | 7 (5.64%) | - | Hematological disorders and infections |
| Etiological category | Diseases | Number of cases (n = 115) | Percentage (100%) |
| Infections | - | Total = 64 | Total = 55.7 |
| Malaria | 23 | 20 | |
| Enteric | 18 | 15.7 | |
| Viral | 17 | 14.8 | |
| Tuberculosis | 6 | 5.2 | |
| Hematological | - | Total = 44 | Total = 38.3 |
| Hemolytic anemia | 32 | 28 | |
| Leukemia | 12 | 10.3 | |
| Storage disorders | 2 | 1.7 | |
| Miscellaneous | 5 | 4.3 | |
| Age group | Infectious (n = 63) | Hematological (n = 44) | Storage (n = 4) | Miscellaneous (n = 4) | Total (n = 115) |
| <1 year (12) | 7 (11.1%) | 3 (6.8%) | 1 (25.0%) | 1 (25.0%) | 12 (10.4%) |
| One to five years (39) | 25 (39.7%) | 11 (25.0%) | 2 (50.0%) | 1 (25.0%) | 39 (33.9%) |
| Six to 10 years (35) | 18 (28.6%) | 15 (34.1%) | 0 (0%) | 2 (50.0%) | 35 (30.4%) |
| 11-15 years (29) | 13 (20.6%) | 15 (34.1%) | 1 (25.0%) | 0 (0%) | 29 (25.2%) |
| Etiology | Present study (n = 115) |
Kamble et al. [ |
Champatiray et al. [ |
Bricks et al. [ |
| Infections | 64 (55.7%) | 20 (16.1%) | 75 (50%) | 49 (54.8) |
| Hematological | 44 (38.3%) | 100 (80.64%) | 54 (36%) | 32 (36.5) |
| Storage disorders | 2 (1.7%) | 1 (0.8%) | 2 (1.3%) | 3 (3.8) |
| Miscellaneous | 5 (4.3%) | 3 (2.4%) | 19 (12%) | 5 (4.9) |
| Grade of splenomegaly | Number of patients (n = 115) | Percentage (100%) |
| Grade I | 18 | 15.7 |
| Grade II | 23 | 20 |
| Grade III | 51 | 44.3 |
| Grade IV | 14 | 12.2 |
| Grade V | 9 | 7.8 |
| Grade | Present study (n = 115) |
Kamble et al. [ |
Gandhari et al. [ |
| Grades I-II (mild) | 41 (36%) | 46 (37.09%) | 15 (15%) |
| Grade III (moderate) | 51 (44%) | 41 (33.06%) | 62 (62%) |
| Grades IV-V (massive) | 23 (20%) | 37 (29.83%) | 23 (23%) |
| Outcome/response | Mild (n = 41) | Moderate (n = 51) | Massive (n = 23) | Total (n = 115) | Percentage (100%) | p-value |
| Resolved with medical treatment | 36 | 43 | 19 | 98 | 85.3% | 0.021 |
| Required surgery (splenectomy) | 0 | 3 | 2 | 5 | 4.3% | 0.032 |
| Recurrence/relapse | 5 | 5 | 0 | 10 | 8.7% | 0.437 |
| Mortality | 0 | 0 | 2 | 2 | 1.7% | 0.587 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Diagnosis and treatment of tuberculosis · Bartonella species infections research
Introduction
Splenomegaly is defined as an enlargement of the spleen beyond the normal limits for age and body habitus [1]. It can be detected clinically or through imaging modalities such as ultrasonography or a CT scan. As the body’s largest lymphoid organ, the spleen has a variety of immunologic functions, including acting as a sieve for the blood, removing blood cells, microorganisms, and immune complexes [1]. The spleen plays a critical role in hematological, immunological, and reticuloendothelial functions; thus, its enlargement often reflects systemic disease processes. An enlarged spleen is a frequent and important clinical sign [2]. A palpable spleen is often the earliest clinical sign of splenic enlargement and warrants further investigation, particularly if it remains palpable beyond 2 cm below the costal margin or increases progressively in size [3]. In pediatric patients, clinical assessment must account for physiological variations with age. Mild splenic enlargement may be considered normal in neonates and infants; progressive or massive enlargement requires thorough evaluation [4]. Even though a pathological spleen only becomes palpable once it reaches at least two to three times its normal size, it may be normally palpable in healthy neonates and children [5,6].
The etiology of splenomegaly in children is diverse, encompassing infections, hematological disorders, malignancies, storage diseases, portal hypertension, and autoimmune conditions [7]. The pattern varies according to age, geographic region, and endemic diseases. In developing countries, infectious causes such as malaria, enteric fever, and tuberculosis remain predominant. Hematological disorders, including thalassemia, sickle cell anemia, and leukemia, are the second most common causes in Indian children [4]. Storage disorders and autoimmune conditions are relatively rare but remain important differentials.
Recent epidemiologic research from India and Andhra Pradesh (2018-2024) highlights important shifts in the spectrum and prevalence of pediatric splenomegaly. Population-based studies from tertiary centers report a prevalence ranging from 1.4% to 2% among pediatric admissions, with most cases occurring in children under six years and a consistent male predominance. Infections, particularly malaria and viral illnesses, remain frequent, but there is increasing documentation of hematologic disorders such as thalassemia and sickle cell anemia as significant contributors, matching trends seen in regional studies and corroborating international comparisons. Despite these data, updated, localized epidemiologic data are sparse for Andhra Pradesh over the last decade. Factors, such as changing infectious disease patterns, the prevalence of inherited hemoglobinopathies, and sociodemographic shifts, may affect disease presentation and outcomes. Hence, this study aims to fill a critical knowledge gap by profiling causes, clinical features, and outcomes of pediatric splenomegaly specific to this region.
Given this diversity, understanding the regional and age-specific patterns of splenomegaly is crucial for effective diagnosis and management.
The primary objective is to determine the clinico-etiological profile of splenomegaly in children aged one month to 15 years admitted to a tertiary care hospital in coastal Andhra Pradesh. The secondary objectives are to analyze correlations between age, sex, and clinical presentation patterns; to assess associated systemic findings and categorize splenomegaly using both Hackett’s and conventional clinical grading systems; and to evaluate treatment response, recurrence, and outcome trends, thereby identifying prognostic indicators relevant to the region.
Materials and methods
Study design and setting
This was a hospital-based prospective observational study conducted in the Department of Pediatrics at a tertiary care teaching hospital, Great Eastern Medical School and Hospital, Srikakulam, over a period of 12 months (January 2024-December 2024).
Ethical approval
The study was approved by the Institutional Ethics Committee Great Eastern Medical School and Hospital (162/IEC/GEMS&H/2023), and informed consent was obtained from parents or guardians, in accordance with standard ethical practices and the Declaration of Helsinki. The Declaration emphasizes prioritizing participant well-being, obtaining informed consent, ensuring scientific validity, and providing additional protections for vulnerable groups such as children.
Study population
The study included a total of 115 children, aged one month to 15 years, who were admitted to the pediatric ward with clinically detectable splenomegaly on physical examination, and whose parents or guardians provided written informed consent for participation.
Children were excluded from the study if they had abdominal distension such that the spleen was not separately palpable, if they had a past history of splenectomy, or if their parents or guardians declined to provide consent.
Sample size
A sample of 115 children was obtained during the study period using a consecutive sampling method. All eligible patients presenting to the Department of Pediatrics with splenomegaly were included until the end of the 12-month study duration. Similar sample sizes and approaches were adopted in earlier regional studies on pediatric splenomegaly.
Data collection
All children underwent detailed history-taking and thorough clinical examination. Data collected included demographic information, presenting complaints, duration of illness, associated symptoms (fever, pallor, abdominal pain, jaundice, bleeding), and relevant clinical signs (hepatomegaly, purpura, growth parameters).
Hematological and other relevant investigations, like complete blood picture, peripheral smear, reticulocyte count, CRP, ESR, and abdominal ultrasonography, were performed for each child. Assessment done by two observers. Any discrepancy in grading between the two observers was resolved by joint re-examination and consensus, and the final grading was then confirmed for every patient by abdominal ultrasonography. Additional investigations were carried out as appropriate, including chest X-ray, liver function tests, renal function tests, dengue serology, malaria parasite card test, sickling test, hemoglobin electrophoresis, high-performance liquid chromatography (HPLC), serum LDH, Mantoux test, Widal test, HIV serology, bone marrow examination, skull X-ray, blood grouping, blood culture, and CT scan of the chest and abdomen. Investigations followed recommendations outlined in earlier clinical assessment protocols for pediatric splenomegaly [4].
Grading of splenomegaly was performed through detailed clinical examination and supported by relevant radiological investigations. The degree of splenic enlargement was classified according to Hackett’s clinical grading system, as presented in Table 1 [8].
The grading of splenomegaly, based on the conventional classification described in Hutchinson’s Clinical Methods, is summarized in Table 2.
Study outcomes
The potential causes of splenomegaly in children were investigated, and the outcomes of the study group were assessed in terms of complete recovery, clinical improvement, or mortality, following methodologies used in similar pediatric studies [9-12].
Outcome assessment
Complete recovery was defined as the complete resolution of presenting symptoms and normalization of both clinical and laboratory parameters at follow-up. Clinically, this included the absence of fever, abdominal pain or distension, bleeding tendency, jaundice, and other constitutional symptoms. On physical examination, complete recovery was characterized by regression or non-palpability of the spleen on abdominal examination. Laboratory evidence of recovery included normalization of hemogram parameters such as hemoglobin, total and differential leukocyte counts, and platelet counts, along with resolution of the underlying etiology, for instance, parasite clearance in malaria, negative blood cultures in bacterial infections, or improvement in liver function tests in hepatic causes.
Clinical improvement was defined as a partial resolution of symptoms and reduction in spleen size, with or without complete normalization of laboratory findings. Clinically, this corresponded to relief in major presenting symptoms such as subsidence of fever, reduction in abdominal pain, and improvement in appetite. On examination, clinical improvement was evidenced by a decrease in spleen size by at least 2 cm below the costal margin compared to baseline. Laboratory parameters showed partial improvement in blood counts or organ function tests, though complete normalization was not always achieved.
Follow-up
A follow-up period of three months was instituted for all study participants to monitor clinical progress and treatment response. During follow-up visits, patients were reassessed for symptom resolution, spleen size reduction by physical examination, and relevant laboratory parameters to document complete recovery or clinical improvement.
Data analysis
The collected data were compiled in Microsoft Excel 2007 (Microsoft® Corp., Redmond, WA), verified for accuracy and consistency, and then analyzed using SPSS version 16.0 (IBM Corp., Armonk, NY). Comparisons between categorical variables were made using the chi-square test or Fisher’s exact test when appropriate. A p-value < 0.05 was considered statistically significant. The data were summarized using descriptive statistics such as proportions, means, and percentages, and the results were compared with findings from previous Indian and international studies.
Results
Demographic profile
Out of 115 children studied, a male preponderance was observed, consistent with findings from other Indian series [9-11]. The majority of cases, 51 (44%) occurred in children below six years of age, which aligns with observations by Gandhari et al. and Champatiray et al., who also reported higher prevalence in younger age groups [10,11].
The majority of children were below six years of age, and a male preponderance was observed, as shown in Table 3.
Clinical presentation
Fever constituted the most common presenting symptom, occurring in 80 children (70%), followed by abdominal pain in 34 children (30%) and jaundice in nine children (8%). Similar symptom profiles have been documented in prior pediatric splenomegaly studies in both Indian and global cohorts, as shown in Table 4 [9-12].
The most common clinical signs observed in children with splenomegaly were pallor and hepatomegaly, followed by lymphadenopathy and bleeding manifestations. Associated hepatomegaly was noted in 42 children (36.5%), reflecting the overlap of systemic infectious and hematological causes, as shown in Table 5.
Etiological profile
Infectious diseases were the predominant cause of splenomegaly, with malaria, enteric fever, and tuberculosis contributing the largest share, as shown in Table 6. This pattern is consistent with prior studies from endemic regions of India, which highlight infectious etiologies as the leading contributors [10,11]. Hematological disorders, including hemolytic anemia and sickle cell disease, accounted for a smaller but significant proportion, similar to reports by Rajanna et al. [2]. Storage disorders and other rare causes were identified in a minority of cases, in line with international data.
In the present study, the majority of cases (33.9%) were observed in the one to five years age group, followed by six to 10 years (30.4%) and 11-15 years (25.2%), while infants (<1 year) accounted for 10.4% of the total cases. Infectious causes predominated across all age groups, being most frequent in children aged one to five years (39.7%) and six to 10 years (28.6%). Hematological etiologies were more common among older children, particularly in the six to 10 years (34.1%) and 11-15 years (34.1%) groups. Storage and miscellaneous causes were relatively rare and distributed sporadically across age categories, with a slight clustering in the younger age group (<5 years), as shown in Figure 1.
Age-wise distribution of etiological groupsThe bar chart illustrates the relationship between age groups and underlying etiological categories. Infectious causes were predominant in younger children, particularly in the one to five years age group, while hematological causes were more frequent among older children (six to 15 years). Storage and miscellaneous causes were comparatively rare and evenly distributed across age groups.
Infectious and hematological causes exhibited an inverse relationship with age: infectious etiologies were more common in younger children, whereas the prevalence of hematological causes increased with advancing age, as illustrated in Table 7.
Table 8 presents a comparative analysis of the etiological profiles of splenomegaly as reported in this study, alongside findings from other published studies.
Distribution of patients according to the grading of splenomegaly
According to Hackett’s classification, Grade III splenomegaly was the most frequent clinical grade, observed in 51 (44.3%) patients, followed by Grade II in 23 (20%) and Grade I in 18 (15.7%) children. This distribution is similar to that reported in malaria-endemic regions, where moderate splenomegaly predominates, as shown in Table 9 [9,11].
Table 10 provides a comparison of splenomegaly grading observed in this study with the grading systems and findings reported in other studies.
Outcome and response to treatment
With appropriate management, 98 (85.2%) of children achieved complete recovery or significant improvement. These outcome rates are comparable to those reported in other Indian studies, where mortality ranged from 2-5% [9,11]. The recurrence rate was low, as shown in Table 11.
All patients completed the study follow-up without any dropouts, ensuring complete data capture for outcome analysis.
Discussion
Splenomegaly in children is a clinical manifestation of diverse systemic illnesses, predominantly of infectious and hematological origin in developing countries [10,11]. The present study was primarily designed to construct an etiological profile of pediatric splenomegaly in this region, with secondary aims focused on analyzing age- and sex-related associations, clinical grading correlations, and treatment outcomes.
Historically, congestive and hematological causes were considered the most frequent, but recent studies highlight infections as the leading etiology in endemic regions [10,11].
In this prospective study of 115 pediatric patients with splenomegaly, 51 (44.3%) were below six years of age, including 12 (10.4%) infants (<1 year) and 39 (33.9%) children aged one to five years, highlighting the substantial burden of splenomegaly in early childhood. Comparable findings were reported by Gandhari et al., with 48% of cases under six years, and Champatiray et al., with 45% in the same age group [10,11].
A male predominance was noted, with 73 (63.5%) males and 42 (36.5%) females (M:F ratio 1.7:1), consistent with other Indian studies [9-11]. This pattern may reflect greater exposure of males to infectious agents or sociocultural factors influencing healthcare access.
The most common presenting symptom in our cohort was fever, followed by abdominal pain, while pallor and hepatomegaly were the most frequent signs. This aligns with prior observations in similar pediatric populations [9-12].
Ultrasonography was performed in all cases in addition to clinical evaluation to confirm the spleen grade and to assist in etiological evaluation, aligning with current recommendations for the assessment of pediatric splenomegaly. Ultrasonography is an established, safe, fast, and reliable method for the measurement of spleen size [13]. Moderate (Grade III) splenomegaly was the most common presentation, followed by mild and massive grades.
Infectious etiologies were the predominant cause of splenomegaly, accounting for 64 (55.7%) cases. Among these, malaria was observed in 23 (20%), enteric fever in 18 (15.7%), and tuberculosis in six (5%) patients. These findings are comparable to those reported by Gandhari et al., where infections constituted 50% of cases, with malaria accounting for 25%, and by Champatiray et al., who reported 52% infectious causes, including malaria in approximately 29% of cases [10,11]. Similarly, Bricks et al. (47.2%) also demonstrated an infectious predominance [12]. In contrast, Kamble et al. reported hematological disorders - primarily hemolytic anemia and thalassemia - as the leading etiology, accounting for 80.6% of cases, highlighting regional variations in hemoglobinopathy prevalence [9].
International studies mirror these patterns: Suttorp et al. described hyper-reactive malarial splenomegaly in an adolescent, emphasizing immunological mechanisms, and Elmakki et al. highlighted tropical splenomegaly syndrome in endemic zones [4,14].In contrast, O’Reilly, in a series of 2,505 patients from the United States, reported hematologic, hepatic, and malignant causes as predominant, with infections forming a minority [15].
The significant association of hematological etiologies with higher grades of splenomegaly (χ² = 8.52, p = 0.004) aligns with the chronic nature of these disorders, causing sustained splenic enlargement. The pattern of infectious etiologies dominating younger ages and hematological conditions increasing with age supports age-specific diagnostic considerations, reinforcing the importance of thorough hematological workups in older children presenting with massive splenomegaly.
Most children, 98 (85.2%), responded favorably to medical management, underscoring the effectiveness of timely diagnosis and appropriate treatment, particularly for infectious causes. Splenectomy was required in 10 (8.7%) cases, primarily for refractory hematological disorders. Recurrence occurred in five (4.3%) patients, reflecting persistence or reactivation of underlying conditions such as malaria or hemoglobinopathies. Mortality was low, reported in two (1.7%) cases, likely attributable to improved diagnostic facilities, enhanced antimicrobial therapy, and better supportive care. These findings emphasize that pediatric splenomegaly generally carries a favorable prognosis when managed promptly and appropriately [9,12].
In summary, this study demonstrates that infectious diseases remain the predominant cause of pediatric splenomegaly in developing countries, particularly in children under six years.
Hematological causes of splenomegaly are relatively common in this region due to several interrelated factors. The high prevalence of hemoglobinopathies, including β-thalassemia, sickle cell disease, and other inherited disorders, particularly in Eastern India and Andhra Pradesh, leads to chronic hemolysis and subsequent splenic enlargement. Nutritional deficiencies, such as iron, folate, and vitamin B12 deficiencies, are also frequent and contribute to chronic anemia, stimulating extramedullary hematopoiesis and further splenomegaly. Endemic infections, including malaria, kala-azar, and enteric fever, may unmask or exacerbate underlying hematological conditions. In some communities, consanguineous marriages increase the likelihood of homozygous hemoglobinopathies, which often present with early-onset splenomegaly. Additionally, limited access to early diagnosis and screening delays recognition of these conditions, resulting in children presenting with moderate to massive splenomegaly. Together, these factors explain the relatively high frequency of hematological disorders as a secondary cause of pediatric splenomegaly in this population.
Hematological and storage disorders represent secondary contributors. Early recognition, appropriate investigations, and timely treatment are crucial to reducing morbidity and mortality.
Limitations
Limitations of the study include the relatively small sample size from a single tertiary care center, which may limit the generalizability of the findings to broader populations. Some diagnostic tests were performed based on clinical judgment, potentially introducing variability in etiological classification. The three-month follow-up, while adequate for assessing short-term outcomes, may not capture long-term sequelae or relapses.
Conclusions
This study shows that infectious diseases remain the leading cause of pediatric splenomegaly in developing regions, particularly in younger children, while hematological disorders are more common in older age groups and often associated with severe presentations. The findings reflect regional epidemiological patterns, with infections predominating in low-resource settings and non-infectious causes more frequent in higher-income areas. Accurate clinical grading and ultrasound assessment are essential for early diagnosis and appropriate management. Larger, multicentric studies are needed to validate these observations and refine context-specific strategies for improving outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Splenomegaly in malaria patients in a tertiary care institute: a study from central India Int J Med Res Rev Soni P Jalaly T 10320183
- 2Assessment of etiological factors and clinical outcome of splenomegaly among the children admitted under paediatric department, Siddipet district, Telangana state Int J Paediatrics Geriatrics Rajender PP Patruni M 252732020
- 3Splenomegaly Stat Pearls Chapman J Goyal A Azevedo AM Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 430907/
- 4Splenomegaly in children and adolescents Front Pediatr Suttorp M Classen CF 59202110.3389/fped.2021.704635 PMC 829875434307263 · doi ↗ · pubmed ↗
- 5Spleen size evaluation in children: time to define splenomegaly for pediatric surgeons and pediatricians P Lo S One Pelizzo G Guazzotti M Klersy C 013201810.1371/journal.pone.0202741 PMC 610719730138410 · doi ↗ · pubmed ↗
- 6Sonographic assessment of the normal limits of the spleen in healthy school children in South-East Nigeria Niger J Clin Pract Ezeofor SN Obikili EN Anyanwu GE Onuh AC Mgbor SO 4844881720142490947410.4103/1119-3077.134046 · doi ↗ · pubmed ↗
- 7A clinicohematological profile of splenomegaly Int J Res Med Sci Tangde A Sonwane B Bindu R 20102015
- 8Splenomegaly in patients with sideropenic anemias: clinical and hematologic significance J Hematol Khaled SAA Seifeldein GS 839352016