Relationship between Helicobacter pylori infection and remnant cholesterol: the mediating role of insulin resistance and inflammation
Yi Chen, Lingyan Shen, Ningning You, Jinshun Zhang

TL;DR
This study finds that Helicobacter pylori infection is linked to higher remnant cholesterol levels, with insulin resistance and inflammation playing key roles in this connection.
Contribution
The study identifies insulin resistance and inflammation as mediators linking H. pylori infection to elevated remnant cholesterol.
Findings
H. pylori infection is significantly associated with increased remnant cholesterol levels.
Insulin resistance and inflammation mediate the relationship between H. pylori and remnant cholesterol.
Persistent H. pylori infection leads to a marked increase in remnant cholesterol over time.
Abstract
Helicobacter pylori (H. pylori) represents a widespread chronic bacterial infection that has garnered increasing attention in recent years due to its extra-gastric effects. Remnant cholesterol (RC) is recognized as a non-traditional lipid marker and is a significant predictor of residual risk in atherosclerotic cardiovascular disease. This investigation aimed to analyze the correlation between H. pylori infection and RC levels, as well as to reveal the underlying mechanisms. The study population comprised individuals undergoing routine health examinations at the health examination center of Taizhou Hospital. All participants were subjected to urea breath tests, blood tests, and anthropometric measurements. The triglyceride-glucose (TyG) index was utilized to assess insulin resistance (IR) levels, while the erythrocyte sedimentation rate (ESR) was utilized as an indicator of chronic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
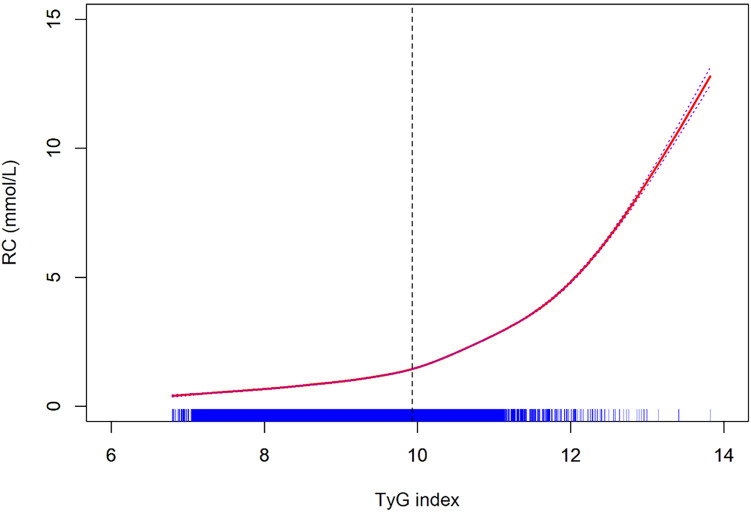 Figure 1
Figure 1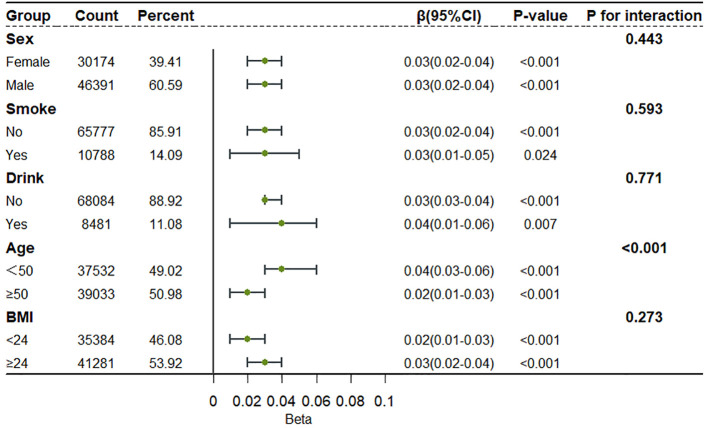 Figure 2
Figure 2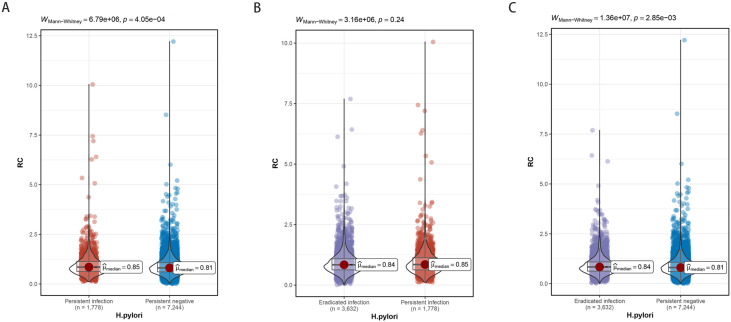 Figure 3
Figure 3| Variables | P-value | ||
|---|---|---|---|
| Sex (n, %) | <0.001 | ||
| Female | 21093 (40.2) | 9081 (37.7) | |
| Male | 31353 (59.8) | 15038 (62.3) | |
| Smoke (n, %) | 0.001 | ||
| No | 45210 (86.2) | 20567 (85.3) | |
| Yes | 7236 (13.8) | 3552 (14.7) | |
| Drink (n, %) | 0.054 | ||
| No | 46559 (88.8) | 21525 (89.2) | |
| Yes | 5887 (11.2) | 2594 (10.8) | |
| Age (years) | 49.08 ± 12.55 | 49.80 ± 12.47 | <0.001 |
| Creatinine (μmol/L) | 70.26 ± 19.04 | 71.04 ± 19.32 | <0.001 |
| Total cholesterol (mmol/L) | 5.20 ± 1.03 | 5.16 ± 1.02 | <0.001 |
| High density lipoprotein (mmol/L) | 1.43 ± 0.34 | 1.40 ± 0.32 | <0.001 |
| Low density lipoprotein (mmol/L) | 2.86 ± 0.76 | 2.82 ± 0.76 | <0.001 |
| Triglyceride (mmol/L) | 1.39 (0.96-2.08) | 1.45 (0.98-2.22) | <0.001 |
| Remnant cholesterol (mmol/L) | 0.83 (0.64-1.08) | 0.86 (0.66-1.09) | <0.001 |
| Diastolic blood pressure (mmHg) | 76.33 ± 11.83 | 76.91 ± 12.11 | <0.001 |
| Systolic blood pressure (mmHg) | 127.17 ± 17.86 | 128.34 ± 18.85 | <0.001 |
| Fasting blood glucose (mmol/L) | 5.43 ± 1.40 | 5.54 ± 1.65 | <0.001 |
| Glycated hemoglobin A1c (%) | 5.87 ± 0.90 | 5.94 ± 1.01 | <0.001 |
| TyG index | 8.72 ± 0.66 | 8.78 ± 0.70 | <0.001 |
| Erythrocyte sedimentation rate (mm/h) | 7 (3–13) | 7 (4–14) | <0.001 |
| Body mass index (kg/m2) | 24.38 ± 3.30 | 24.65 ± 3.32 | <0.001 |
| B (95%CI) | Standard error | P-value | |
|---|---|---|---|
| Model 1 | 0.029 (0.021, 0.036) | 0.004 | <0.001 |
| Model 2 | 0.029 (0.022, 0.036) | 0.004 | <0.001 |
| Model 3 | 0.007 (0.003, 0.011) | 0.002 | 0.002 |
| Model 4 | 0.005 (0.001, 0.010) | 0.002 | 0.016 |
| Mediation effect | Estimate | 95% CI lower | 95% CI upper | P-value |
|---|---|---|---|---|
| Total effect | 0.029 | 0.021 | 0.036 | <0.001 |
| Direct effect | 0.007 | 0.002 | 0.012 | 0.010 |
| Indirect effect | 0.022 | 0.017 | 0.026 | <0.001 |
| Proportion mediated | 0.758 | 0.631 | 0.929 | <0.001 |
| Mediation effect | Estimate | 95% CI lower | 95% CI upper | P-value |
|---|---|---|---|---|
| Total effect | 0.029 | 0.021 | 0.036 | <0.001 |
| Direct effect | 0.026 | 0.018 | 0.033 | <0.001 |
| Indirect effect | 0.003 | 0.002 | 0.004 | <0.001 |
| Proportion mediated | 0.104 | 0.074 | 0.146 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Microscopic Colitis · Steroid Chemistry and Biochemistry
Introduction
Helicobacter pylori (H. pylori) is a spiral-shaped, Gram-negative, microaerophilic bacterium characterized by multiple flagella, which predominantly colonizes the gastric mucosa in humans (Gu, 2017). It is one of the most common chronic bacterial infections worldwide (Engelsberger et al., 2024). Epidemiological data indicate that the global prevalence of H. pylori infection surpasses 50%, with even higher incidence rates reported in developing nations where sanitation is inadequate (Gravina et al., 2018). The World Health Organization has classified H. pylori as a Group 1 carcinogen, and it is definitively associated with various gastrointestinal diseases (Elshenawi et al., 2023). Recent research has increasingly highlighted that the pathological impact of H. pylori infection extends beyond localized gastrointestinal disturbances. H. pylori may induce systemic low-grade inflammatory responses, disrupt host immune regulatory functions, and impair metabolic signaling pathways, potentially impacting multiple distant organ systems (Bravo et al., 2018; He et al., 2022). In particular, its associations with cardiovascular and metabolic conditions, including atherosclerosis, non-alcoholic fatty liver disease, diabetes and lipid metabolism disorders, have attracted growing scholarly attention (Tsay and Hsu, 2018; Wang et al., 2020; Xie et al., 2023). These findings indicate that H. pylori is not solely a pathogenic element for gastric diseases but may also contribute to chronic systemic inflammation, posing a significant threat to the host’s metabolic homeostasis. However, the underlying mechanisms remain complex and necessitate further investigation.
Remnant cholesterol (RC) comprises the portion of cholesterol transported by intermediate-density lipoprotein cholesterol, very low-density lipoprotein (VLDL) cholesterol, and chylomicron remnants (Burnett et al., 2020). This cholesterol is not covered by the traditionally measured high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol, and it primarily resides in triglyceride-rich lipoprotein particles (Burnett et al., 2020; Wadström et al., 2023b). Recent researches have demonstrated that RC plays an independent and significant pathological role in the formation of atherosclerotic plaques and the incidence of cardiovascular events (Castañer et al., 2020; Xu et al., 2024; Li et al., 2025). Although LDL has traditionally been viewed as the primary atherogenic lipid factor, numerous clinical investigations have demonstrated that elevated RC levels are strongly correlated with residual risk for atherosclerotic cardiovascular disease, even when patients’ LDL levels are within target or optimal ranges (Sandesara et al., 2019; Heo and Jo, 2023).
Researches have indicated that individuals infected with H. pylori frequently exhibit dyslipidemia, potentially linked to mechanisms such as chronic low-grade inflammation, dysbiosis, and insulin resistance (IR) (Kim et al., 2016; Zhao et al., 2019; Martin-Nuñez et al., 2021; Qiu et al., 2025). The erythrocyte sedimentation rate (ESR) is a well-established nonspecific inflammatory marker that remains extensively used for monitoring chronic systemic inflammation due to its high sensitivity, low cost, and technical simplicity, making it effective in reflecting the body’s long-term inflammatory state (Erikssen et al., 2000; Corsonello et al., 2011). Similarly, the triglyceride-glucose (TyG) index, derived from fasting blood glucose (FBG) and triglyceride (TG) levels, has been proposed and widely adopted for the indirect assessment of IR (Lim et al., 2019; Tahapary et al., 2022). It offers significant advantages, including ease of use, low cost, good stability, and robust predictive capability, particularly demonstrating wide applicability in epidemiological studies and preliminary clinical screenings (Tao et al., 2022). While existing literature indicates a possible link between H. pylori and dyslipidemia, there remains a paucity of systematic research specifically examining the relationship between H. pylori and RC levels. Consequently, this study seeks to assess the potential association between H. pylori infection and RC levels utilizing a large population dataset, in addition to exploring the underlying mechanisms involved.
Methods
Study participants
This study encompassed individuals who participated in routine health examinations at the Taizhou Hospital Health Management Center between June 2017 and March 2024. We excluded individuals with incomplete clinical data, a history of malignancies, a history of gastrointestinal surgeries, severe cardiovascular or cerebrovascular conditions, those currently undergoing lipid-lowering medication treatment, and individuals experiencing acute infections. A total of 76,565 individuals participated in the study. Additionally, some individuals underwent multiple health examinations. Based on the status of H. pylori infection during the initial and final examinations (with a follow-up period exceeding one year), the participants were categorized into three groups: persistent infection (positive at both time points), persistent negative (negative at both assessments), and eradicated infection (transition from positive to negative), resulting in 12,654 individuals for further analysis. In this study, H. pylori was treated using the standard quadruple therapy regimen, which includes a proton pump inhibitor, a bismuth compound, and two antibiotics.
Clinical index collection
Demographic information and lifestyle data of the participants, encompassing age, sex, smoking and alcohol consumption history, as well as medical history, were collected by trained nurses from the Health Management Center using a structured questionnaire. Subsequently, height, weight, seated systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured according to standardized protocols. All participants provided fasting venous blood samples after fasting for a minimum of eight hours, which were promptly sent to the laboratory for analysis. The laboratory tests included creatinine (Cr), TG, HDL, LDL, total cholesterol (TC), FBG, glycated hemoglobin (HbA1c), and ESR. RC was calculated using the formula: RC = TC − HDL − LDL. Body mass index (BMI) was defined as weight (kg) divided by height (m) squared (Huxley et al., 2010). The TyG index was calculated using the formula: ln [TG (mg/dL) × FBG (mg/dL)/2] (Simental-Mendía et al., 2008).
Detection of H. pylori
Following an overnight fast, all participants underwent either the ^13^C or ^14^C breath test. The protocol for the ^13^C breath test involves the participant initially exhaling into a specialized collection bag after normal inhalation. Subsequently, the participant ingests a ^13^C-labeled urea capsule with water, ensuring that the capsule remains intact. After a 30-minute interval, the participant exhales into a second collection bag to complete the procedure, and the samples are then dispatched for analysis. In the case of the ^14^C breath test, participants directly ingest a capsule containing ^14^C-labeled urea with water. After remaining seated quietly for 15 minutes, they exhale slowly into a designated breath card. The samples are then forwarded for analysis.
Statistical analysis
Categorical variables were analyzed using chi-square tests and reported as frequencies and percentages. Continuous variables were evaluated using independent t-tests or Mann-Whitney tests to assess differences between groups. The relationships between variables were assessed using Spearman correlation tests. To investigate the association between H. pylori and RC, multivariable linear regression analysis was conducted after adjusting for potential confounders. A generalized additive model was employed to examine the association between the TyG index and RC. Furthermore, a mediation analysis was performed to explore the mediating effects of the TyG index and ESR on the relationship between H. pylori and RC. All statistical analyses were carried out using R software (version 4.4.1), with statistical significance determined at a threshold of P < 0.05.
Results
Study participants
Table 1 provides a comprehensive overview of the baseline characteristics of all participants. The cohort within the H. pylori group demonstrated a higher prevalence of males, smokers, and individuals who consumed alcohol. Furthermore, this group was characterized by an older age demographic and exhibited elevated levels of Cr, RC, SBP, DBP, HbA1c, FBG, TyG index, ESR, and BMI. Conversely, this group presented with reduced levels of TC, HDL, and LDL.
Multiple regression analysis
To examine the impact of H. pylori on RC, a multiple linear regression analysis was performed, incorporating variables such as smoking, drinking, TG, Cr, SBP, FBG, ESR, and BMI, alongside sex and age. The findings, presented in Table 2, indicate that H. pylori remains a significant risk factor for RC. The correlations among these factors are illustrated in Supplementary Figure S1.
Mediation analysis
To further clarify the role of IR and inflammation in the association between H. pylori and RC, we performed a mediation analysis. After controlling for gender and age, findings revealed that the TyG index acts as a mediator in the relationship between H. pylori and RC, with a mediation proportion of 75.8% (95% CI = 63.1%-92.9%) (Table 3). Similarly, the ESR was identified as a mediator in this association, with a mediation proportion of 10.4% (95% CI = 7.4%-14.6%) (Table 4). Moreover, an increase in the TyG index was correlated with elevated RC levels; notably, when the TyG index surpassed 9.93, a significant increase in RC levels was observed (Figure 1).
Non-linear relationship between TyG index and RC.
Subgroup analysis
To better understand the association between H. pylori and RC across different populations, subgroup analyses were undertaken. Participants were stratified based on to sex, smoking, drinking, age, and BMI. The results indicated that H. pylori serves as a risk factor for RC in various populations; however, a significant interaction effect between age and H. pylori was identified, with a more pronounced impact in younger individuals (Figure 2).
Subgroup analysis of the relationship between H. pylori infection and RC levels.
Longitudinal relationship between H. pylori and RC
The study cohort was observed over a median follow-up duration of 3.2 years. The persistent infection group showed significantly higher RC levels compared to the persistent negative group (Figure 3A). Although the eradicated infection group exhibited lower RC levels than the persistent infection group, this difference was not statistically significant (Figure 3B). Nonetheless, RC levels in the eradicated infection group were elevated in comparison to the persistent negative group (Figure 3C).
The effect of different H. pylori infection status on RC levels. (A) Persistent infection group compared with persistent negative group. (B) Eradicated infection group compared with persistent infection group. (C) Eradicated infection group compared with persistent negative group. Group differences were assessed using the Mann-Whitney tests, with test statistics and P values shown.
Discussion
Cardiovascular diseases contribute significantly to global mortality and disability, leading major economic burdens (Roth et al., 2020). Recently, RC has been recognized as a critical metabolic marker for evaluating cardiovascular residual risk, especially in individuals with multiple metabolic disorders or those at high cardiovascular risk, where its clinical assessment and intervention potential are significant (Huh et al., 2022; Wadström et al., 2023a). This study systematically examined the link between H. pylori infection and RC levels utilizing data from a large-scale health screening population for the first time. The results showed a significant association between H. pylori infection and higher RC levels, with this relationship holding statistical significance even after considering a range of potential confounders.
H. pylori is acknowledged as a persistent infectious agent, with its pathogenic mechanisms having been extensively investigated (Camilo et al., 2017; de Brito et al., 2019). It prompts the release of inflammatory substances like interleukin-6 and tumor necrosis factor-alpha, thereby activating a low-grade chronic inflammatory response (Cheng et al., 2017). This process may disrupt host immune homeostasis and metabolic pathways, potentially leading to dyslipidemia. The present study identified that people infected with H. pylori exhibit significantly elevated RC levels, while LDL and TC levels are reduced in these individuals. This finding may underscore the independent significance of RC as a non-traditional lipid marker in predicting cardiovascular residual risk. Mediation analysis findings showed that the TyG index is a crucial mediator linking H. pylori to RC levels, implying that IR could be the pivotal mechanism through which H. pylori impacts RC levels. Researches indicate that H. pylori can lead to a reduction in the phosphorylation of insulin signaling proteins, thereby hindering the activation of downstream proteins and inducing IR (Zhou et al., 2015; He et al., 2016). In IR states, the capacity of adipose tissue to respond to insulin and inhibit lipolysis is compromised, resulting in an increased release of free fatty acids (FFAs) (Avramoglu et al., 2006; Choi and Ginsberg, 2011). These FFAs are subsequently absorbed by the liver, where they are re-esterified into TG, thus promoting the synthesis and secretion of VLDL (Choi and Ginsberg, 2011). As the primary precursor of RC, an increase in VLDL provides a foundation for elevated RC levels. Furthermore, this study identified that the ESR mediates the relationship between H. pylori and RC levels, underscoring the role of systemic inflammation as a significant pathway in this association. Regarding lipoprotein metabolism, inflammation is posited to inhibit lipoprotein lipase activity, delay VLDL clearance, and enhance cholesteryl ester transfer protein activity, ultimately contributing to the accumulation of RC in TG-rich particles (Dallinga-Thie et al., 2010; Ginsberg et al., 2021; Yanai et al., 2022). Additionally, it has been proposed that H. pylori-induced intestinal dysbiosis may influence lipid metabolism through the gut-hepatic axis, a mechanism that warrants further investigation (Martin-Nuñez et al., 2021; Nabavi-Rad et al., 2022).
The subgroup analysis of this research further indicated that the relationship between H. pylori infection and RC levels was relatively consistent across various populations. However, it was notably more pronounced in younger individuals compared to older ones. This phenomenon may be attributed to the heightened sensitivity of metabolic systems and the increased activation of the immune system in younger individuals. Although some large observational studies have reported sex differences in the prevalence of H. pylori infection, their influence on downstream metabolic consequences remains inconclusive (Ibrahim et al., 2017). In the present study, the association between H. pylori infection and RC elevation was comparable in men and women, suggesting that metabolic pathways linking infection and lipid dysregulation may be largely sex-independent. Longitudinal analysis revealed that the elevation of RC levels was more significant among individuals with persistent H. pylori infection. Conversely, although RC levels exhibited a slight decrease in the group where the infection had been eradicated, they continued to show an upward trend compared to those with persistent negative status. This finding implies that the impact of H. pylori infection on RC may be delayed or partially irreversible. This observation aligns with previous reports indicating limited metabolic improvement following H. pylori eradication, underscoring the importance of early screening and intervention (Upala et al., 2017).
This research assessed the association between H. pylori infection and RC levels with a large population sample, utilizing mediation analysis to explore potential underlying mechanisms. Nonetheless, certain limitations persist. Firstly, despite controlling for various potential confounding factors, unmeasured residual confounders related to lifestyle and dietary patterns may still impact the results. Secondly, as this investigation is a single-center study, additional multi-center studies are required to enhance generalizability. Furthermore, the absence of typing data for H. pylori virulence factors, such as VacA and CagA, limits the ability to differentiate the effects of various strains on RC levels.
In summary, this study is the first to identify a significant positive association between H. pylori infection and RC levels within a large-scale population, and further revealed the potential mechanism of inflammation and IR in this association through mediation modeling. The above findings not only enrich the perspective of systemic metabolic effects of H. pylori, but also suggest that it may be an important modifier of residual cardiovascular risk. This provides a theoretical foundation for future investigations into H. pylori as a potential target for interventions in cardiovascular and metabolic diseases. Future studies should conduct prospective follow-up and randomized intervention trials in multi-center populations to assess the long-term effects of H. pylori eradication therapy on RC levels and downstream atherosclerosis risk, and to provide theoretical basis and evidence-based support for its incorporation into comprehensive cardiovascular disease management strategies.
Conclusion
Our research identified an association between H. pylori infection and increased levels of RC, with IR and inflammation acting as mediating factors in this relationship.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Avramoglu R. K. Basciano H. Adeli K. (2006). Lipid and lipoprotein dysregulation in insulin resistant states. Clinica chimica acta; Int. J. Clin. Chem. 368, 1–19. doi: 10.1016/j.cca.2005.12.026, PMID: 16480697 · doi ↗ · pubmed ↗
- 2Bravo D. Hoare A. Soto C. Valenzuela M. A. Quest A. F. (2018). Helicobacter pylori in human health and disease: Mechanisms for local gastric and systemic effects. World J. gastroenterology. 24, 3071–3089. doi: 10.3748/wjg.v 24.i 28.3071, PMID: 30065554 PMC 6064966 · doi ↗ · pubmed ↗
- 3Burnett J. R. Hooper A. J. Hegele R. A. (2020). Remnant cholesterol and atherosclerotic cardiovascular disease risk. J. Am. Coll. Cardiol. 76, 2736–2739. doi: 10.1016/j.jacc.2020.10.029, PMID: 33272367 · doi ↗ · pubmed ↗
- 4Camilo V. Sugiyama T. Touati E. (2017). Pathogenesis of Helicobacter pylori infection. Helicobacter 22 Suppl 1. doi: 10.1111/hel.12405, PMID: 28891130 · doi ↗ · pubmed ↗
- 5Castañer O. PintóX. Subirana I. Amor A. J. Ros E. HernáezÁ. . (2020). Remnant cholesterol, not LDL cholesterol, is associated with incident cardiovascular disease. J. Am. Coll. Cardiol. 76, 2712–2724. doi: 10.1016/j.jacc.2020.10.008, PMID: 33272365 · doi ↗ · pubmed ↗
- 6Cheng D. D. He C. Ai H. H. Huang Y. Lu N. H. (2017). The possible role of helicobacter pylori infection in non-alcoholic fatty liver disease. Front. Microbiol. 8, 743. doi: 10.3389/fmicb.2017.00743, PMID: 28539915 PMC 5423951 · doi ↗ · pubmed ↗
- 7Choi S. H. Ginsberg H. N. (2011). Increased very low density lipoprotein (VLDL) secretion, hepatic steatosis, and insulin resistance. Trends Endocrinol. metabolism: TEM. 22, 353–363. doi: 10.1016/j.tem.2011.04.007, PMID: 21616678 PMC 3163828 · doi ↗ · pubmed ↗
- 8Corsonello A. Pedone C. Battaglia S. Paglino G. Bellia V. Incalzi R. A. (2011). C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as inflammation markers in elderly patients with stable chronic obstructive pulmonary disease (COPD). Arch. gerontology geriatrics. 53, 190–195. doi: 10.1016/j.archger.2010.10.015, PMID: 21074870 · doi ↗ · pubmed ↗