The relationship between preoperative hypoalbuminemia and postoperative subsyndromal delirium in elderly hip fracture patients: a prospective study
Peipei Li, Zi Ruo Zhang, Dan Chen, Hong Zhi, Jing Hu, Ping Xie, Lian Wen, Si Tong Yan

TL;DR
This study found that low preoperative albumin levels in elderly hip fracture patients are linked to a higher risk of postoperative delirium symptoms.
Contribution
The study identifies hypoalbuminemia as an independent risk factor for postoperative subsyndromal delirium in elderly hip fracture patients.
Findings
21.51% of patients had preoperative hypoalbuminemia.
Hypoalbuminemia increased the risk of postoperative SSD by 6.13 times.
A threshold effect was observed between albumin levels and SSD risk.
Abstract
This study aimed to assess the prevalence of preoperative hypoalbuminemia in patients with hip fractures at Honghui Hospital, Xi’an Jiaotong University, and to examine its associations with postoperative subsyndromal delirium (SSD) and postoperative discharge-status. A prospective study was conducted at Honghui Hospital, Xi’an Jiaotong University, involving patients who underwent hip fracture surgery between October 2023 and March 2024. Data on demographics, comorbidities, preoperative serum albumin levels, SSD occurrence, and postoperative discharge status were also collected. Hypoalbuminemia was defined as serum albumin levels below 35 g/L. In total, 279 patients were included in the analysis. Hypoalbuminemia was observed in 60 patients (21.51%) and 114 patients (40.86%) exhibited postoperative SSD. Multivariate logistic regression analysis revealed that diabetes mellitus (OR =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
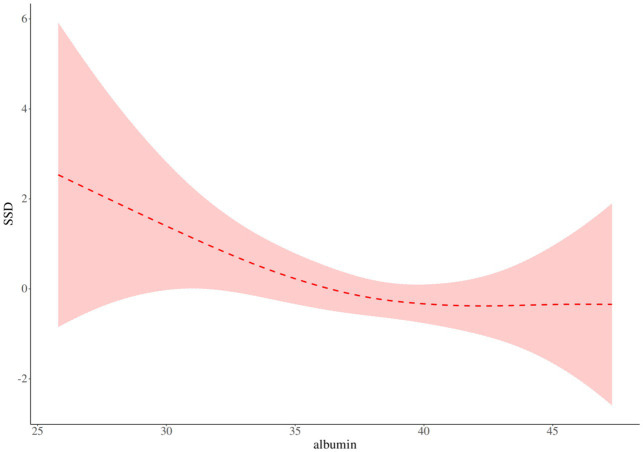 Figure 1
Figure 1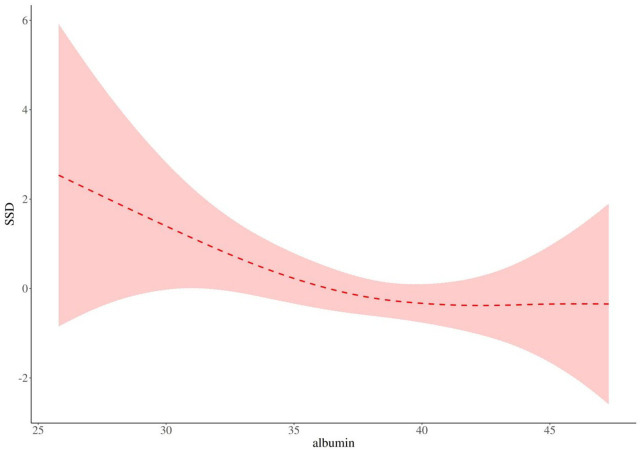 Figure 2
Figure 2| Variables | Total ( | Albumin ≥35 g/L | Albumin <35 g/L | Statistic |
|
|---|---|---|---|---|---|
| Age, Mean ± SD | 75.55 ± 8.01 | 75.43 ± 8.14 | 75.97 ± 7.58 | 0.649 | |
| MMSE score, Mean ± SD | 22.69 ± 4.76 | 22.97 ± 4.69 | 21.67 ± 4.92 | 0.060 | |
| LOS (d), Mean ± SD | 9.42 ± 4.34 | 9.43 ± 4.11 | 9.37 ± 5.13 | 0.916 | |
| Hb (g/L), Mean ± SD | 117.20 ± 20.25 | 120.66 ± 19.55 | 104.57 ± 17.68 | <0.001 | |
| Creatinine (ummol/L), Mean ± SD | 67.51 ± 31.52 | 69.76 ± 33.95 | 59.07 ± 17.72 | 0.021 | |
| BMI (kg/m2), Mean ± SD | 22.24 ± 3.46 | 22.26 ± 3.52 | 22.18 ± 3.27 | 0.881 | |
| Duration of operation (min), Mean ± SD | 110.73 ± 49.60 | 109.59 ± 45.69 | 114.90 ± 62.12 | 0.538 | |
| NRS score, M (Q₁, Q₃) | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | 2.00 (1.00, 4.00) | 0.458 | |
| Depth of anesthesia, M (Q₁, Q₃) | 22.00 (21.00, 22.00) | 22.00 (21.00, 22.50) | 22.00 (22.00, 22.00) | 0.875 | |
| Sex, | 0.027 | ||||
| Male | 114 (40.86) | 82 (37.44) | 32 (53.33) | ||
| Female | 165 (59.14) | 137 (62.56) | 28 (46.67) | ||
| Type of fracture, | 0.434 | ||||
| Femoral neck fracture | 160 (57.35) | 126 (57.53) | 34 (56.67) | ||
| Intertrochanteric fracture | 101 (36.20) | 81 (36.99) | 20 (33.33) | ||
| Subtrochanteric fracture | 18 (6.45) | 12 (5.48) | 6 (10.00) | ||
| Hypertension, | 0.086 | ||||
| No | 140 (50.18) | 104 (47.49) | 36 (60.00) | ||
| Yes | 139 (49.82) | 115 (52.51) | 24 (40.00) | ||
| CHD, | 0.775 | ||||
| No | 229 (82.08) | 179 (81.74) | 50 (83.33) | ||
| Yes | 50 (17.92) | 40 (18.26) | 10 (16.67) | ||
| DM, | 0.102 | ||||
| No | 210 (75.27) | 160 (73.06) | 50 (83.33) | ||
| Yes | 69 (24.73) | 59 (26.94) | 10 (16.67) | ||
| CVAs, | 0.410 | ||||
| No | 189 (67.74) | 151 (68.95) | 38 (63.33) | ||
| Yes | 90 (32.26) | 68 (31.05) | 22 (36.67) | ||
| COPD, | 0.320 | ||||
| No | 265 (94.98) | 210 (95.89) | 55 (91.67) | ||
| Yes | 14 (5.02) | 9 (4.11) | 5 (8.33) | ||
| Smoking, | 0.154 | ||||
| No | 32 (11.47) | 22 (10.05) | 10 (16.67) | ||
| Yes | 247 (88.53) | 197 (89.95) | 50 (83.33) | ||
| Type of operation, | 0.833 | ||||
| THA and partial-hip replacement | 154 (55.20) | 122 (55.71) | 32 (53.33) | ||
| ORIF | 12 (4.30) | 10 (4.57) | 2 (3.33) | ||
| Closed reduction and internal fixation | 113 (40.50) | 87 (39.73) | 26 (43.33) | ||
| ASA-PS score, | – | <0.001 | |||
| 1 | 4 (1.43) | 2 (0.91) | 2 (3.33) | ||
| 2 | 92 (32.97) | 82 (37.44) | 10 (16.67) | ||
| 3 | 181 (64.87) | 135 (61.64) | 46 (76.67) | ||
| 4 | 2 (0.72) | 0 (0.00) | 2 (3.33) | ||
| Type of anesthesia, | – | 0.107 | |||
| GA | 28 (10.04) | 26 (11.87) | 2 (3.33) | ||
| RA | 2 (0.72) | 2 (0.91) | 0 (0.00) | ||
| GA + RA | 249 (89.25) | 191 (87.21) | 58 (96.67) | ||
| Intraoperative blood transfusion, | 0.018 | ||||
| No | 176 (63.08) | 146 (66.67) | 30 (50.00) | ||
| Yes | 103 (36.92) | 73 (33.33) | 30 (50.00) | ||
| SSD, | <0.001 | ||||
| No | 165 (59.14) | 143 (65.30) | 22 (36.67) | ||
| Yes | 114 (40.86) | 76 (34.70) | 38 (63.33) |
| Variables |
| S.E |
|
| OR (95%CI) |
|---|---|---|---|---|---|
| Sex | |||||
| Male | Reference | ||||
| Female | 0.15 | 0.25 | 0.60 | 0.550 | 1.16 (0.71–1.89) |
| Type of fracture | |||||
| Femoral neck fracture | Reference | ||||
| Intertrochanteric fracture | 0.03 | 0.26 | 0.10 | 0.919 | 1.03 (0.62–1.70) |
| Subtrochanteric fracture | −1.78 | 0.77 | −2.32 | 0.020 | 0.17 (0.04–0.76) |
| CHD | |||||
| No | Reference | ||||
| Yes | 0.16 | 0.32 | 0.52 | 0.602 | 1.18 (0.64–2.19) |
| DM | |||||
| No | Reference | ||||
| Yes | 0.58 | 0.28 | 2.09 | 0.036 | 1.79 (1.04–3.09) |
| Hypertension | |||||
| No | Reference | ||||
| Yes | 0.66 | 0.25 | 2.66 | 0.008 | 1.93 (1.19–3.13) |
| CVAs | |||||
| No | Reference | ||||
| Yes | 0.60 | 0.26 | 2.31 | 0.021 | 1.82 (1.10–3.02) |
| COPD | |||||
| No | Reference | ||||
| Yes | 1.02 | 0.57 | 1.78 | 0.076 | 2.76 (0.90–8.46) |
| Smoking | |||||
| No | Reference | ||||
| Yes | 1.21 | 0.47 | 2.56 | 0.010 | 3.34 (1.33–8.41) |
| Type of operation | |||||
| THA and partial-hip replacement | Reference | ||||
| ORIF | −1.43 | 0.79 | −1.80 | 0.071 | 0.24 (0.05–1.13) |
| Closed reduction and internal fixation | −0.36 | 0.25 | −1.41 | 0.158 | 0.70 (0.43–1.15) |
| ASA-PS score | |||||
| 1 | / | ||||
| 2 | 15.29 | 1,199.77 | 0.01 | 0.990 | / |
| 3 | 16.63 | 1,199.77 | 0.01 | 0.989 | / |
| 4 | 0.00 | 2,078.07 | 0.00 | 1.000 | / |
| Type of anesthesia | |||||
| GA | Reference | ||||
| RA | −14.28 | 624.19 | −0.02 | 0.982 | 0.00 (0.00–Inf) |
| GA + RA | −0.08 | 0.40 | −0.21 | 0.834 | 0.92 (0.42–2.02) |
| Intraoperative blood transfusion | |||||
| No | Reference | ||||
| Yes | 0.23 | 0.25 | 0.92 | 0.358 | 1.26 (0.77–2.06) |
| Hypoalbuminemia | |||||
| No | Reference | ||||
| Yes | 1.18 | 0.30 | 3.89 | <0.001 | 3.25 (1.79–5.89) |
| Age | 0.06 | 0.02 | 3.58 | <0.001 | 1.06 (1.03–1.09) |
| MMSE score | −0.30 | 0.04 | −7.95 | <0.001 | 0.74 (0.69–0.80) |
| Hb | −0.01 | 0.01 | −1.26 | 0.207 | 0.99 (0.98–1.00) |
| Creatinine | −0.00 | 0.00 | −0.20 | 0.838 | 1.00 (0.99–1.01) |
| BMI | 0.01 | 0.04 | 0.37 | 0.708 | 1.01 (0.95–1.09) |
| NRS score | −0.05 | 0.10 | −0.51 | 0.610 | 0.95 (0.78–1.15) |
| Depth of anesthesia | −0.22 | 0.12 | −1.88 | 0.060 | 0.81 (0.64–1.01) |
| Duration of operation | −0.00 | 0.00 | −1.33 | 0.184 | 1.00 (0.99–1.00) |
| Variables |
| S.E |
|
| OR (95%CI) |
|---|---|---|---|---|---|
| Intercept | 3.01 | 2.27 | 1.33 | 0.185 | 20.35 (0.24–1,745.24) |
| Type of fracture | |||||
| Femoral neck fracture | Reference | ||||
| Intertrochanteric fracture | 0.32 | 0.34 | 0.96 | 0.335 | 1.38 (0.72–2.67) |
| Subtrochanteric fracture | −1.23 | 0.86 | −1.43 | 0.153 | 0.29 (0.05–1.58) |
| DM | |||||
| No | Reference | ||||
| Yes | 1.08 | 0.40 | 2.68 | 0.007 | 2.93 (1.34–6.44) |
| Hypertension | |||||
| No | Reference | ||||
| Yes | 0.49 | 0.34 | 1.46 | 0.145 | 1.64 (0.84–3.19) |
| CVAs | |||||
| No | Reference | ||||
| Yes | 0.11 | 0.35 | 0.32 | 0.747 | 1.12 (0.56–2.23) |
| Smoking | |||||
| No | Reference | ||||
| Yes | 1.46 | 0.69 | 2.13 | 0.033 | 4.30 (1.12–16.49) |
| Hypoalbuminemia | |||||
| No | Reference | ||||
| Yes | 1.81 | 0.42 | 4.28 | <0.001 | 6.13 (2.67–14.05) |
| Age | 0.01 | 0.02 | 0.54 | 0.590 | 1.01 (0.97–1.06) |
| MMSE score | −0.29 | 0.04 | −6.63 | <0.001 | 0.74 (0.68–0.81) |
| Variables | Albumin ≥35 g/L | Albumin <35 g/L | OR (95%CI) |
| ||
|---|---|---|---|---|---|---|
| All patients | 279 (100.00) | 76/219 | 38/60 | 3.25 (1.79–5.89) | <0.001 | |
| Sex | 0.469 | |||||
| Male | 114 (40.71) | 26/82 | 18/32 | 2.77 (1.20–6.41) | 0.017 | |
| Female | 166 (59.29) | 50/137 | 20/28 | 4.35 (1.79–10.60) | 0.001 |
| Outcome | Effect |
|
|---|---|---|
| Model 1 Fitting model by standard linear regression | 0.89 (0.83–0.95) | <0.001 |
| Model 2 Fitting model by two-piecewise linear regression | ||
| Inflection point | 38.4 | |
| <38.4 | 0.78 (0.69–0.90) | <0.001 |
| ≥38.4 | 1.03 (0.87–1.22) | 0.713 |
| 0.034 |
| Variables | Total | Albumin ≥35 g/L | Albumin <35 g/L |
|---|---|---|---|
| Postoperative destination, | |||
| In-hospital ward | 257 (92.11) | 202 (92.24) | 55 (91.67) |
| ICU | 22 (7.89) | 17 (7.76) | 5 (8.33) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Cardiac, Anesthesia and Surgical Outcomes · Nutrition and Health in Aging
Introduction
According to statistics, the annual number of new cases of hip fracture in China exceeds 1 million, and it is on the rise, with a high incidence in the elderly, especially those over 65 years of age, accounting for approximately 95% of the total number (1, 2). Surgery is the primary treatment for hip fractures in the elderly (3). Malnutrition is prevalent in older people with hip fractures and reduces their ability to recover from injuries (4). Markers of malnutrition was low serum albumin and has been found to affect hip fracture outcomes. Bohl et al. (5) study reported that the prevalence of hypoalbuminemia was 45.9% in elderly patients undergoing hip fracture surgery. At the same time, some studies have found that preoperative hypoproteinemia not only significantly affects the immune function and anti-infection ability of patients, but also increases the risk of postoperative complications, including confusion, mortality and prolonged hospital (6–9). In clinical practice, hypoalbuminemia has a serious impact on patients’ quality of life and treatment effects; therefore, in-depth studies are of great clinical significance.
Subsyndromal Delirium (SSD) is characterized by a sudden onset condition affecting attention and consciousness, presenting with one or more core symptoms of delirium but does not meet the criteria for full-blown delirium (4, 10). Hospitalized older patients frequently exhibit signs of acute cognitive decline and attentional impairment, and are ultimately diagnosed with delirium (11). Research indicates that up to 50% of individuals with hip fractures experience episodes of delirium during hospitalized (12). Additionally, certain investigations have revealed that hypoalbuminemia can predict postoperative complications, such as infections, increased mortality rates, and longer hospital stays (13). Hypoalbuminemia is an indicator of malnutrition, reflecting the poor physical condition of patients (14). Hypoalbuminemia is also known to be a risk factor for delirium (15). Nevertheless, studies specifically addressing the influence of low albumin levels on the incidence of subsyndromal delirium following hip fractures in older adults are lacking. Consequently, this research aimed to explore potential risk factors contributing to postoperative subsyndromal delirium in elderly patients with hip fractures and to examine whether low albumin levels are associated with postoperative subsyndromal delirium as well as patient outcomes after surgery.
Methods
Hospital Ethics Review Board approval was obtained prior to the start of the study (approval number: 202410002). We collected the clinical data of 342 patients who underwent hip fracture between October 2023 and March 2024 at Honghui Hospital, Xi’an Jiaotong University, including patient demographics and preoperative comorbidities such as age, sex, body mass index (BMI), smoking, hemoglobin (Hb) level, hypertension, history of previous cerebrovascular accidents (CVAs), Coronary Heart Disease (CHD), diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), preoperative creatinine level, preoperative serum albumin level, type of fracture, Mini-Mental State Examination (MMSE) score (16), American Society of Anesthesiologist Physical Status (ASA-PS) score (17), details of the operation such as duration of operation, type of anesthesia, type of operation, depth of anesthesia, and intraoperative blood transfusion (18); postoperative data included the Numeric Rating Scale (NRS) (19), and length of hospital stay (LOS). We defined the window for preoperative serum albumin levels to be taken at admission and a minimum of 1 day before the surgery. We also defined serum albumin levels below 35 g/L as hypoalbuminemia.
The primary outcome was SSD, and the secondary outcomes were postoperative destination, in-hospital ward, or ICU. We used the confusion assessment method (CAM) (20) to collect subsyndromal delirium, which involves four core symptoms (21): ① acute changes in consciousness; ② attention deficits; ③ disorganized thinking; ④ changes in level of consciousness. If one or more of the four core symptoms of CAM are present and do not meet the diagnostic criteria for delirium, it indicates the presence of SSD; if all four core symptoms of CAM are present with characteristic ①, characteristic ② and characteristic ③ (or characteristic ④), it indicates the presence of delirium. Before the study began, the evaluators studied the operation process and scoring criteria of the relevant scales in detail, and learned the operation guide manual of CAM evaluators to ensure the scientificity and reliability of the evaluation work. The CAM assessment was conducted by trained researchers using observation and face-to-face interviews to collect data. If the patient developed symptoms on days 1–3 after surgery, two assessors evaluated the occurrence time, duration (in days), clinical presentation, and whether delirium progressed; if the subject was discharged after surgery, it was considered lost to follow-up; if the subject was transferred to another department after surgery, the investigator will continue to evaluate the subject in the transferred department; if the subject is transferred to the ICU after surgery, the investigator will enter the ICU and evaluate the subject using the same data collection method to reduce the subjective bias of evaluators and improve the objectivity and credibility of the research results. The evaluation of the outcome indicators was conducted by two rigorously trained assessors: the researcher (Assessor A) and another graduate student from the research group (Assessor B). The two assessors stood on opposite sides of the same subject and used a rotating questioning method for blind assessments. In case of disputes, they consulted a neurologist for the final determination, with the physician’s final decision being the standard.
After excluding 38 patients younger than 65 years, 6 patients with combined fractures in the other, 8 patients with more than three missing variables, and 11 patients who did not have preoperative serum albumin levels, we obtained 279 patients in the final analysis.
Statistical analysis
The collected variables were quality-checked, screened, and sorted, and a database was established using Excel. R4.3.3 software was used for data analysis, and numerical variables were expressed as mean ± standard deviation and categorical variables as frequency and percentages. Data for continuous variables were normally distributed using an independent t-test; data for continuous variables were non-normally distributed using the rank sum test and chi-square test for categorical variables. Logistic regression was used for one-way analysis of each variable, and predictor variables were screened according to the criterion of p ≤ 0.05. The factors resulting from screening were included in the multifactorial logistic regression analysis, and a regression model was used to observe the effect of hypoalbuminemia on postoperative subsyndromal delirium in elderly patients with hip fracture under different adjustment strategies. Finally, the serum albumin level was used as a continuous variable for serum albumin and SSD threshold analysis using R4.3.3.
Results
Demographics
Of the 279 elderly patients who experienced hip fracture during the study period, 21.51% had hypoalbuminemia, 40.86% had SSD, and hypoalbuminemia 63.33% had SSD. As shown in Table 1. Patients with hypoalbuminemia had lower mean Hb levels than those with normal albumin levels (p < 0.001) and lower preoperative creatinine levels (p = 0.021). However, patients with hypoalbuminemia tended to have a higher male ASA-PS score (p < 0.001), intraoperative blood transfusion (p = 0.018), and incidence of SSD (p < 0.001). There were no significant differences in the other variables between the two groups.
Table 1: Demographics of patients with normal albumin (≥35 g/L) versus those with hypoalbuminemia (<35 g/L) postoperative hip fracture in elderly.
Results of the univariate logistic regression
Univariate logistic regression analysis was performed using SSD as the dependent variable. Based on the univariate analysis presented in Table 2, the variables associated with an elevated risk of SSD included age (OR = 1.06, p < 0.001), subtrochanteric fractures (OR = 0.17, p = 0.020), DM (OR = 1.79, p = 0.036), hypertension (OR = 1.93, p = 0.008), CVAs (OR = 1.82, p = 0.021), smoking (OR = 3.34, p = 0.010), and hypoalbuminemia (OR = 3.25, p < 0.001). Additionally, the risk of developing SSD decreases as MMSE scores increase.
Results of the multivariate logistic regression
This study employed a single-factor strategy for variable selection, incorporating variables from Table 2 that demonstrated statistical significance (p < 0.05) in univariate analysis into the multivariate regression analysis. Based on the multivariate analysis presented in Table 3, the variables associated with an independent elevated risk of SSD included DM (OR = 2.93, p = 0.007), smoking (OR = 4.30, p = 0.033), and hypoalbuminemia (OR = 6.13, p < 0.001). Each one-point increase in MMSE score was associated with a 26% reduction in the odds of SSD (OR = 0.74, p < 0.001).
In the subgroup analysis stratified by sex (Table 4), males (n = 114) showed a moderate association (OR = 2.77, 95% CI: 1.20–6.41, p = 0.017), while females (n = 166) demonstrated a stronger association (OR = 4.35, 95% CI: 1.79–10.60, p = 0.001). However, the interaction effect between sex and albumin levels was not statistically significant (p for interaction = 0.469), indicating that sex did not significantly modify the observed association.
Albumin and SSD threshold analysis results
As shown in Table 5 and Figure 1, there is a threshold effect for the association of albumin and SSD (p for likelihood test = 0.034); in general, albumin and SSD were negatively associated [OR (95%CI): 0.89 (0.83–0.95), p < 0.001], when the albumin is below 38.4 g/L, albumin and SSD were negatively associated [OR (95%CI): 0.78 (0.69–0.90), p < 0.001]; when the albumin level was above 38.4 g/L, no association of albumin and SSD was found; at the same time, I also adjusted for sex, age, intraoperative blood transfusion, and Hb, and the results showed that there is a threshold effect for the association of albumin and SSD (p for likelihood test = 0.025), albumin, and SSD were negatively associated [OR (95%CI): 0.87 (0.80–0.94), p < 0.001], Figure 2.
Albumin and SSD threshold analysis.
Albumin and SSD threshold analysis after adjustment for covariates.
Postoperative destination
A total of 22 patients went to the ICU among the 279 patients (Table 6). Five patients with hypoalbuminemia were admitted to the ICU, and no further statistical analysis was performed owing to the low ICU occupancy rate.
Discussion
Our study found that the incidence of preoperative hypoalbuminemia in elderly patients undergoing hip fracture surgery was 21.51%, whereas the incidence of SSD in patients with hypoalbuminemia was 63.33%. Although the classical definition of hypoalbuminemia is <30 g/L, some studies have reported that serum total protein is <60 g/L or albumin is <35 g/L as hypoalbuminemia, because even mild hypoalbuminemia affects the outcome of patients (22, 23). The criterion for hypoalbuminemia in this study was an albumin level of <35 g/L. The incidence of preoperative hypoalbuminemia is not low, with an incidence of 14–20.7% (24, 25). Our study showed a higher incidence of hypoalbuminemia than that reported in the literature. The first studied population was older and often had a certain degree of digestive and absorption function, insufficient intake of protein and other nutrients, and limited absorption, resulting in varying degrees of preoperative malnutrition (26). Second, hip fractures in the elderly are mostly osteoporotic fractures, and recent studies have found a correlation between hypoalbuminemia and osteoporosis and fracture, which may affect bone metabolism in various ways, resulting in decreased bone mass, decreased bone density, and osteoporosis (27). Afshinnia and Pennathur (28) found that the incidence of osteoporosis in the femoral neck in patients with hypoalbuminemia was significantly higher than that in those with normal albumin, and the difference was statistically significant; therefore, hypoalbuminemia should be actively corrected to reduce the occurrence of related osteoporosis, reduce muscle strength reduction, and prevent the occurrence of osteoporotic fractures the same time. Most studies have reported a significant relationship between hypoalbuminemia and poor patient prognosis (29, 30), the incidence of SSD in hypoalbuminemia has rarely been reported.
Our study found that subjects with hypertension had a higher risk of developing SSD compared to healthy subjects (p < 0.001). Hypoalbuminemia was an independent influencing factor affecting postoperative SSD in elderly patients with hip fracture, consistent with previous studies that showed that the preoperative risk of malnutrition and malnutrition status increased the risk of postoperative delirium (31). Albumin is an important indicator of the nutritional status of the body and plays an important role in the overall function of the body (32). The relationship between nutritional status and rehabilitation after fracture has been reported in some studies, including hip function after hip fracture (7) and the risk of postoperative SSD (33). Therefore, comprehensive nutritional assessment should be conducted in elderly patients with hip fracture, focusing attention on patients with albumin below 35 g/L, and preoperative albumin as a key measurement index to accurately assess the risk of postoperative SSD.
Our study also found that individuals with diabetes had a higher risk of SSD than those without diabetes (p = 0.007). Consistent with the results of a study by Kalyan et al., elderly patients with diabetes and other complications were more likely to develop SSD (34). In the study, smokers were found to have a higher risk of developing SSD (p = 0.033). However, there have been few studies addressing the link between smoking and SSD. Moreover, each one-point increase in MMSE score was associated with a 26% reduction in the odds of SSD. Consistent with the findings of Denny and Such (35), MMSE is an independent risk factor for postoperative SSD in older adults, highlighting preoperative diabetes and poor preoperative cognitive function as risk factors for high risk of SSD, thus using screening for diabetes and cognitive function assessment as a routine preoperative examination item for patients with hip fracture over 65 years of age.
Our results showed a threshold effect on the association of albumin and SSD (p for likelihood test = 0.034), and when albumin<38.4 g/L, the decrease in SSD threshold after increased albumin levels was statistically significant (p < 0.05). However, at albumin≥38.4 g/L, no association of albumin and SSD was found. The results of the study by Lu et al. (36) showed that Preoperative albumin were associated with postoperative delirium, potentially aiding in identifying high-risk patients and playing a key role in preventing POD. The study was shown by Wang et al. (37) treating preoperative serum albumin level as a continuous variable, the risk of postoperative (POD) delirium increased by 11% (95%CI, 1.08–1.15) with each 1 g/L decrease in preoperative serum albumin level. It was also found that maintaining preoperative serum albumin levels above 38 g/L may lead to a more favorable outcome. Probably because, in the central nervous system, low serum albumin levels appear to be insufficient in fully exerting their antioxidant effects and capturing free radicals (38–40). Normal serum albumin levels can provide essential amino acids to the cell and immune system, thereby optimizing the composition ratio between albumin and other inflammatory factors to enhance the body’s immune response capabilities (41, 42). Furthermore, the evaluation of preoperative serum albumin levels could facilitate early identification of high-risk SSD. Therefore, the aim of our study was to encourage clinical healthcare professionals to re-emphasize monitoring and management of preoperative serum albumin levels in elderly patients with hip fractures.
One of the aims of our study was to identify the risk factors for postoperative destination in our study population. However, out of 279 patients, a total of 22 patients went to the ICU, and 5 of patients with hypoproteinemia went to the ICU with low ICU occupancy without further statistical analysis.
Strengths of study
We focused our study on elderly patients who underwent hip fracture, which is more commonly performed in the literature, as we wanted a more homogenous study population. The outcome of our study focused on the occurrence of SSD rather than delirium, and the identification of SSD helped improve the vigilance of the prestate of medical staff and reduce missed diagnoses and misdiagnoses due to inconspicuous symptoms.
Study limitations
This study was limited by its single-center design, potentially impacting the sample size and population homogeneity, which could introduce selection bias during data analysis. Additionally, the rapid changes in hypoalbuminemia over a short period may pose challenges in clinical application, potentially diminishing the significance of hypoalbuminemia as a modifiable risk factor. Moreover, SSD is a multifaceted condition that cannot be solely attributed to a single risk factor, necessitating a comprehensive management approach to effectively mitigate SSD occurrence. At the same time, CAM features may overestimate the incidence of SSD. In later studies, we may use more detailed criteria. Finally, due to limitations in human and material resources, we only analyzed the relationship between preoperative albumin levels and SSD. We did not further examine the relationship between postoperative albumin levels and SSD. Further investigation is needed in the future.
Conclusion
In conclusion, our study revealed a 21.51% prevalence of preoperative hypoalbuminemia among elderly patients undergoing hip fracture surgery at our institution, establishing it as an independent risk factor for postoperative SSD. We advocate for preoperative interventions to address hypoalbuminemia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang C Feng J Wang S Gao P Xu L Zhu J . Incidence of and trends in hipfracture among adults in urban China: a nationwide retrospectivecohort study. P Lo S Med. (2020) 17:e 1003180. doi: 10.1371/journal.pmed.1003180, 32760065 PMC 7410202 · doi ↗ · pubmed ↗
- 2Griffiths R Babu S Dixon P Freeman N Hurford D Kelleher E . Guideline for the management of hip fractures 2020: guideline by the association of anaesthetists. Anaesthesia. (2021) 76:225–37. doi: 10.1111/anae.15291, 33289066 · doi ↗ · pubmed ↗
- 3Sing CW Lin TC Bartholomew S Bell JS Bennett C Beyene K . Global epidemiology of hip fractures: secular trends in incidence rate, post-fracture treatment, and all-cause mortality. J Bone Miner Res. (2023) 38:1064–75. doi: 10.1002/jbmr.4821, 37118993 · doi ↗ · pubmed ↗
- 4Gao Y Gan XN Yang RQ . Conceptual connotation and research progress of subsyndromal delirium. Chin J Nurs. (2021) 56:1883–8.
- 5Bohl DD Shen MR Hannon CP Fillingham YA Darrith B Della Valle CJ. Serum albumin predicts survival and postoperative course following surgery for geriatric hip fracture. J Bone Joint Surg Am. (2017) 99:2110–8. doi: 10.2106/JBJS.16.01620, 29257017 · doi ↗ · pubmed ↗
- 6Takimoto M Yasui-Yamada S Nasu N Kagiya N Aotani N Kurokawa Y . Development and validation of cutoff value for reduced muscle mass for GLIM criteria in patients with gastrointestinal and hepatobiliary-pancreatic cancers. Nutrients. (2022) 14:943. doi: 10.3390/nu 14050943, 35267918 PMC 8912591 · doi ↗ · pubmed ↗
- 7Malafarina V Reginster JY Cabrerizo S Bruyère O Kanis JA Martinez JA . Nutritional status and nutritional treatment are related to outcomes and mortality in older adults with hip fracture. Nutrients. (2018) 10:555. doi: 10.3390/nu 10050555, 29710860 PMC 5986435 · doi ↗ · pubmed ↗
- 8Abd-El-Aziz MA Hübner M Demartines N Larson DW Grass F . Simple clinical screening underestimates malnutrition in surgical patients with inflammatory bowel disease-an ACS NSQIP analysis. Nutrients. (2022) 14:932. doi: 10.3390/nu 14050932, 35267906 PMC 8912602 · doi ↗ · pubmed ↗