Efficacy of botulinum toxin type A in myogenic temporomandibulardisorders: a single arm, prospective, pilot study
Bruno Macedo de Sousa, Nansi López-Valverde, Carolina Ferreira, André Mariz de Almeida, Antonio López-Valverde, José A. Blanco Rueda

TL;DR
This pilot study found that botulinum toxin type A significantly reduced pain and improved function in patients with myofascial temporomandibular disorders.
Contribution
The study provides preliminary evidence for the efficacy of botulinum toxin type A in treating myofascial TMDs.
Findings
Pain levels dropped significantly from 6.84 to 0.84 on the VAS scale.
Functional limitations improved significantly on the JFLS-8 scale.
Quality of life improved significantly on the OHIP-14 scale.
Abstract
Myogenous temporomandibular disorders (TMDs) is commonly associated with myofascial pain and functional limitations. Botulinum toxin type A (BoNT-A) has shown potential in relieving chronic muscular pain. In this single arm, prospective, pilot study, 25 patients diagnosed with myofascial TMDs received a single bilateral intramuscular injection of 50 units of BoNT-A. Assessments using the Visual Analog Scale (VAS), Chronic Pain Index (CPI), Jaw Functional Limitation Scale (JFLS-8), and Oral Health Impact Profile (OHIP-14) were performed at baseline, 6 weeks, and 12 weeks post-treatment. Significant reductions in pain (VAS: 6.84 ± 1.03 to 0.84 ± 0.94) and CPI (61.87 ± 8.12 to 9.86 ± 4.46) were observed. Functional improvement (JFLS-8: 5.82 ± 0.56 to 1.08 ± 0.51) and enhanced quality of life (OHIP-14: 24.56 ± 8.39 to 5.96 ± 2.79) were also significant. No adverse effects were reported.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
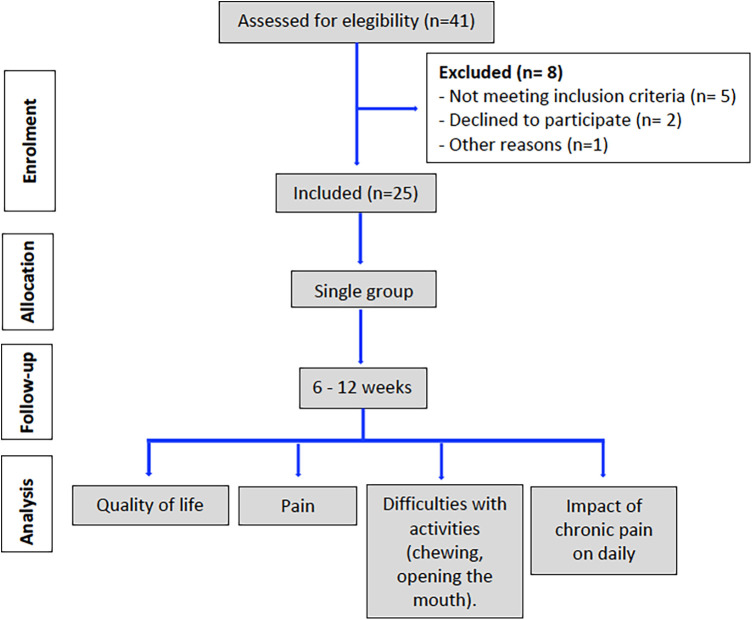 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3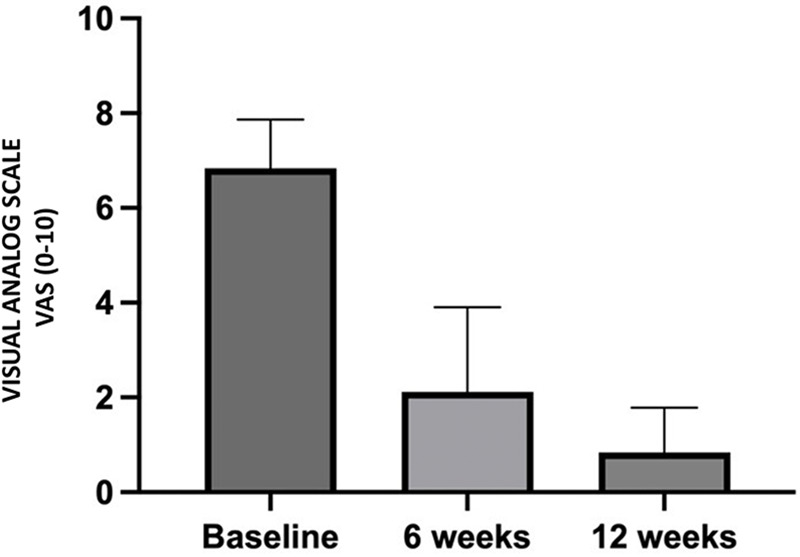 Figure 4
Figure 4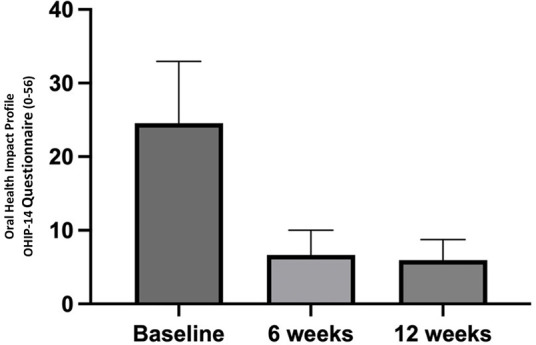 Figure 5
Figure 5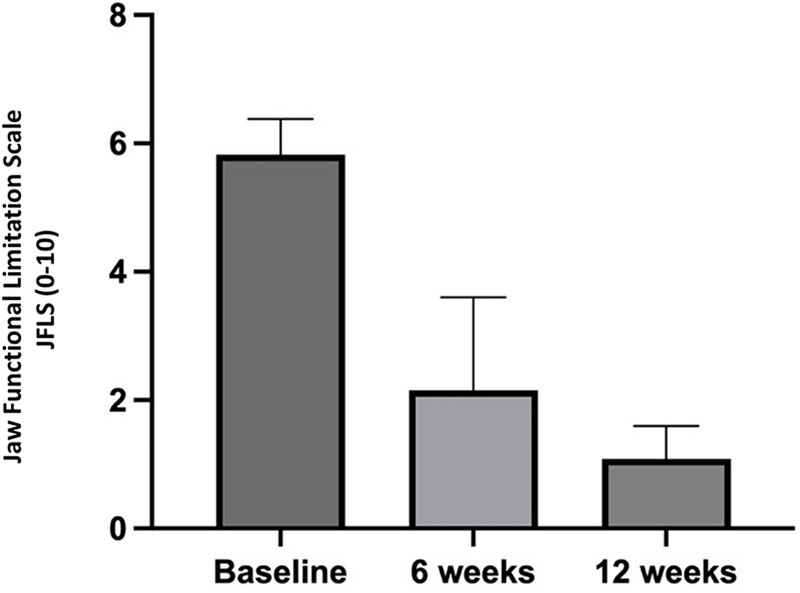 Figure 6
Figure 6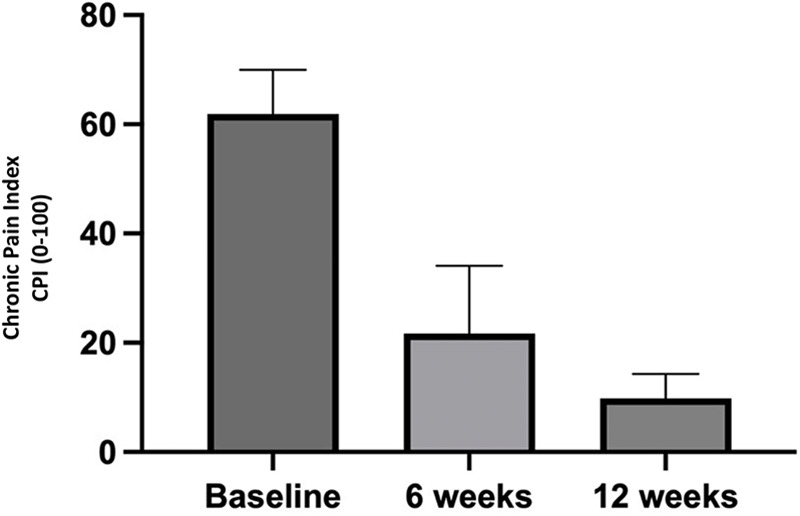 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTemporomandibular Joint Disorders · Botulinum Toxin and Related Neurological Disorders · Myofascial pain diagnosis and treatment
Introduction
1
Temporomandibular disorders (TMDs) are a widely studied topic encompassing a variety of musculoskeletal conditions affecting the temporomandibular joint (TMJ), masticatory muscles, and associated structures. Among the most common conditions are myofascial pain, joint disc displacement, and degenerative joint diseases. Diagnosis is often established using standardized systems, such as the Diagnostic Criteria for TMDs (DC/TMDs), which are universally regarded as the gold standard in scientific research (1). These criteria are organized into two main axes: Axis I, which includes diagnoses based on specific clinical criteria for the most common painful conditions and intra-articular disorders, and Axis II, which assesses biopsychosocial dimensions such as anxiety, depression, stress, and pain-related disability, allowing for a broader and more integrated analysis of the impact of the disorder on the patient's life (2). TMDs present with a wide range of signs and symptoms, including pain in the masticatory muscles, which may radiate to the neck and head; headaches; hearing disorders; tooth wear; limited jaw mobility; muscle hypertrophy; and inflammatory processes or joint noises during jaw movements (3). They are considered the leading cause of non-dental/periodontal orofacial pain and affect people of all ages, although their prevalence is highest in young adults between the ages of 20 and 40. There is a marked female predominance, with a ratio of approximately four women for every man affected. Studies indicate that approximately 31% of adults experience TMDs at some point in their lives. Beyond its high prevalence, the condition can significantly affect quality of life, interfering with essential activities such as chewing, speaking, and swallowing, as well as simple gestures such as yawning (4–6).
The etiology of TMDs is multifactorial, reflecting the interaction between biological, psychological, and social factors. Biologically, it may be associated with genetic predisposition, hormonal changes, pain modulation, and overall physical health (7). Psycho-logically, individual beliefs, anxiety, fear, depression, sleep disorders, and mood changes play a significant role (8). Socially, interpersonal relationships, culture, socioeconomic status, and occupational conditions may influence the onset and progression of TMDs. The interaction between these biopsychosocial factors not only contributes to its manifestation but also affects treatment response, particularly in cases with associated psychological comorbidities such as anxiety and depression. TMDs imposes both individual and societal burdens. Functional limitations and chronic pain substantially reduce patients' quality of life. From an occupational perspective, the condition is associated with increased absenteeism, higher healthcare expenditures, and persistent consultation of multiple healthcare providers (9).
The treatment of TMDs requires a multidisciplinary approach, initially focused on conservative and reversible options aimed at alleviating symptoms without resorting to invasive or irreversible interventions. Treatment usually begins with patient education and learning self-care strategies. These include controlling oral parafunctions (e.g., avoiding teeth clenching or excessive chewing gum use), adopting good sleep hygiene, performing therapeutic exercises, and relaxation techniques. The use of intraoral appliances, such as stabilization splints, is another common strategy for short-term pain relief, although their effectiveness, compared to placebo, remains a subject of debate (10).
Physical therapy also plays a key role, incorporating mobilization and strengthening exercises that have been shown to be effective in reducing pain and improving joint function (11). In more complex cases, pharmacotherapy may be used, employing muscle relaxants, anti-inflammatories, or other centrally and peripherally acting agents (12, 13).
Psychological interventions, such as cognitive behavioral therapy (CBT), have demonstrated long-term benefits, especially in patients with significant psychological symptoms. These approaches, which may include biofeedback, relaxation techniques, and counseling, complement physical treatments by addressing the emotional and social factors that contribute to dysfunction (14). Other strategies, such as acupuncture and dry needling, have proven effective in relieving muscle pain. Intra-articular injections are more suitable for joint pain. Invasive procedures, such as arthrocentesis and surgery, are reserved for severe or treatment-resistant cases (15, 16). For muscle conditions that do not respond to conventional treatments, new approaches have been investigated, such as the use of botulinum toxin type A (BoNT-A). It is a powerful neurotoxin produced by the gram-negative spore-forming bacterium Clostridium botulinum and has become a common treatment for TMDs in recent years. This therapy has shown potential for relieving chronic myofascial pain and other associated muscle conditions, offering hope to patients with persistent and refractory symptoms (17, 18). However, there is no consensus on the effects of BoNT-A in the treatment of painful TMDs, nor on the effects of BoNT-A application in the masticatory muscles of people with bruxism, despite its increasing use in dentistry (19–22). For a time, it was thought that the analgesic effect of botulinum toxin type A (BoNT-A) was due to its muscle-relaxing effect (23). However, recent studies in neuropathic pain models have demonstrated that it has an analgesic effect independent of muscle relaxation through a dissociative effect between the duration of muscle relaxation and the duration of pain relief (24). However, despite having proven effective in treating various conditions, including TMDs, concerns remain about possible adverse effects, particularly on mandibular bone health (25, 26). Studies show that BoNT-A injections into the masticatory muscles can reduce muscle fiber size and alter fiber type proportions, increasing the proportion of type IIb fibers, which have lower fatigue resistance. The findings indicate that a single BoNT-A injection temporarily reduces masticatory function and causes degenerative changes in muscle tissue and bone structure, including alveolar bone resorption, lasting at least four weeks (25, 27). However, there is also no consensus regarding bone-related aspects: repeated injections of BoNT-A appear to exacerbate bone loss compared to single applications; nevertheless, there are no conclusive reports from high-quality studies on this aspect, with most studies being of suboptimal methodological quality and indicating small-magnitude bone changes, which should be interpreted with caution (28). Therefore, although BoNT-A remains a valuable therapeutic tool, it is essential to carefully evaluate its potential risks and benefits in the clinical treatment of TMDs.
The objective of this pilot study was to evaluate the effects of BoNT-A on M-TMDs, as well as to assess its impact on mandibular function and quality of life in treated individuals. This study also analyzed adverse effects to evaluate the safety of BoNT-A in patients with TMDs.
Methods
2
This is a prospective, multicenter, single-group pilot study conducted in collaboration with two academic institutions: The Faculty of Medicine of the University of Coimbra (Portugal) and the Egas Moniz University Institute (Portugal). Its implementation was authorized by the Ethics Committee of the Faculty of Medicine of the University of Coimbra, which issued a favorable opinion at its meeting on September 14, 2023, under file number CE-090/2023. The study is also registered on Clinicaltrials.gov under identifier NCT05651256. All participants included in the study signed informed consent, in accordance with the ethical requirements stipulated by the aforementioned committee.
The study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, which are suitable for single-arm interventional designs without a control group.
Participants
2.1
No formal sample size calculation was performed due to the exploratory and pilot nature of this study. The number of participants was determined based on the estimated recruitment feasibility within the study period and the sample sizes used in similar published studies on botulinum toxin for myogenic temporomandibular disorders. This approach is consistent with previously reported exploratory single-arm trials.
The sample for this study consisted of 25 participants, of whom 21 were women and 4 were men, aged between 23 and 69 years. The mean age was 53.60 ± 12.25 years. The total study period lasted 12 weeks and took place between November 2024 and February 2025. Participant selection and study phases are presented in a flow chart (Figure 1).
Flow chart of progress through the phases of the study according to the CONSORT statement 2010 (29).
Patient description; inclusion and exclusion criteria
2.2
The patients recruited came from the clinics of the two participating institutions. The study exclusively included participants with a confirmed diagnosis of myofascial pain, according to DC/TMD, lasting more than three months and whose pain had not responded to previous conservative treatment.
Participants underwent an initial screening visit 1–2 weeks prior to the baseline assessment. During the screening visit, eligibility was confirmed, medical history was obtained, and DC/TMD diagnostic procedures were completed. All participants underwent standardized clinical assessment including structured history-taking, muscle palpation of the masticatory muscles, and pain localization tests. Diagnostic criteria for myalgia and myofascial pain were applied following DC/TMD definitions.
Exclusion criteria were previous surgery or arthrocentesis of the temporomandibular joint; surgery in the cervicofacial region in the previous six months; active follow-up in a Pain Unit at the time of inclusion; history of previous successful treatment; history of previous treatment with BoNT-A.
All clinical examinations were performed by a single clinician trained in the DC/TMD protocol. Calibration was achieved through joint assessment of pilot cases prior to study initiation, following the recommendations of Schiffman et al. (2014) (1). To minimize confounding, the use of new analgesic medications, muscle relaxants, physiotherapy, occlusal splints, or any other TMD-related interventions was not permitted during the follow-up period.
Axis II (psychosocial) measures were not collected, as the study focused on somatic (Axis I) diagnostic outcomes. This omission is acknowledged as a limitation regarding the assessment of psychosocial comorbidities.
Treatments
2.3
The therapeutic protocol consisted of a single session of bilateral intramuscular injections of BoNT-A, with a total of 50 units (Botox®, Allergan, Irvine, California, USA), previously reconstituted with 0.9% isotonic saline solution. The injection sites were identified based on muscle palpation and contraction induced by dental occlusion, according to a standardized anatomical pattern. Injections were performed using a 1 mL Luer-lock syringe with a 30-gauge, 13 mm needle (0.3 mm × 13 mm). In the anterior temporal muscle, two injection sites were defined in its anterior portion, with 5 units administered per site. In the masseter muscle, five injection points were arranged around a central point, with 3 units administered per point (Figures 2,3). Injections were performed bilaterally, with a total of 25 units per side of the face (30).
Marking of the injection points with the aid of muscle palpation and contraction induced by dental occlusion.
Administration of 5 units of BoNT-A at each temporal point and 3 units at each masseter point.
The lateral pterygoid was deliberately excluded from the injection protocol due to its deep location, proximity to major vascular structures, and higher risk of toxin diffusion to adjacent tissues such as the pterygoid venous plexus, maxillary artery, or extraocular muscles. Injection of this muscle generally requires ultrasound guidance to ensure safe placement, which was not part of the standardized protocol used in this study. To prioritize safety and reproducibility across clinical settings, injections were therefore restricted to the masseter and anterior temporalis muscles, which are easily accessible and commonly targeted in M-TMD research.
No ultrasound guidance was used; instead, muscle palpation and visual anatomical cues were employed to ensure accuracy. All procedures were performed under aseptic conditions, and patients were advised to avoid massage or strenuous activity involving the injected muscles for 24 h post-procedure.
Adverse events
2.4
Adverse events (AEs) were defined according to the International Council for Harmonisation Good Clinical Practice (ICH-GCP) guidelines as any untoward medical occurrence following BoNT-A administration, irrespective of causal relationship to treatment.
AEs were actively solicited at each follow-up visit (weeks 2, 6, and 12) and through scheduled telephone interviews conducted one week after injection. Patients were specifically questioned regarding local reactions (e.g., pain, edema, bruising, muscle weakness, asymmetry) and systemic symptoms.
An AE was defined as any untoward medical occurrence following BoNT-A injection, irrespective of its causal relationship to treatment. Serious adverse events (SAEs) were defined as any event resulting in hospitalization, persistent disability, or life-threatening condition.
All AEs were recorded in standardized case report forms, graded according to severity (mild, moderate, severe), and assessed for possible relation to BoNT-A administration.
Measuring tools
2.5
To conduct a comprehensive assessment of TMDs and response to treatment, a set of validated instruments was used to analyze different dimensions of the patient experience. Pain was assessed using the Visual Analog Scale (VAS), a simple and widely recognized tool that allows patients to indicate pain intensity on a scale from 0 (no pain) to 10 (maximum pain) (31). The VAS is particularly useful for tracking pain over time and response to treatment. Complementarily, the 14-item Oral Health Impact Profile (OHIP-14) was used to measure the impact of oral health on quality of life, covering physical pain, functional limitations, psychological distress, and social impact (32, 33). To quantify specific functional limitations of the jaw, the 8-item Jaw Functional Limitation Scale (JFLS-8) was applied, which assesses difficulties in activities such as chewing, opening the mouth, and speaking, thus reflecting the degree of functional impairment experienced in daily life (34). In addition, the Chronic Pain Inventory (CPI) was used to characterize chronic pain, assessing not only the intensity and frequency of pain, but also its impact on daily activities, interpersonal relationships, and productivity, parameters that are particularly relevant to myofascial pain (35).
To support clinical interpretation of the outcomes, previously validated minimal clinically important differences (MCID) thresholds were applied. For pain intensity on the VAS, an MCID of 1–2 points is widely accepted for chronic musculoskeletal pain. For the OHIP-14, a decrease of 5–6 points represents a clinically meaningful improvement in oral health-related quality of life. For the JFLS-8, a change of approximately 4–8 points has been reported as clinically relevant for functional limitation in the jaw (1, 34).
These thresholds were used to interpret the magnitude of improvement observed in this study.
The combination of these instruments allows for a multidimensional analysis of TMDs, covering pain, jaw function, and quality of life, which are key aspects for a rigorous evaluation of treatment efficacy.
All outcome measures were collected by the same examiner who conducted the baseline evaluations. Due to the single-arm design and longitudinal nature of the study, blinding of the examiner to the treatment timepoint was not feasible. Nevertheless, standardized assessment procedures were applied consistently across all timepoints to minimize measurement variability.
Statistics
2.6
The collected data were organized in Microsoft Excel® spreadsheets and subsequently analyzed using GraphPad Prism® software version 9.5.1 (GraphPad Software, San Diego, CA, USA). Sample normality was verified using the Shapiro–Wilk test.
Statistical analyses were performed using IBM SPSS Statistics version v26 platform (IBM Corp., Armonk, NY, USA). Normality of data distribution was assessed with the Shapiro–Wilk test. For normally distributed variables, changes across timepoints were analyzed using repeated-measures ANOVA, followed by Bonferroni-adjusted pairwise comparisons. For non-normally distributed data, the Friedman test was applied, with Wilcoxon signed-rank tests for post-hoc comparisons.
Effect sizes were reported as partial eta-squared (η^2^) for ANOVA and r for nonparametric tests, with corresponding 95% confidence intervals (CIs) where applicable.
Missing data were handled by listwise deletion, as fewer than 5% of data points were incomplete. Statistical significance was set at p < 0.05 (two-tailed) after correction for multiple comparisons.
Results
3
Results for pain
3.1
All analyses were conducted according to the predefined statistical plan. Effect sizes and 95% confidence intervals are reported to facilitate interpretation of clinical relevance.
Statistical analysis revealed a significant reduction in pain intensity after BoNT-A administration. On average, the Visual Analog Scale (VAS) score decreased from 6.84 ± 1.03 at the start of the study to 2.12 ± 1.79 six weeks after treatment (p = 0.0002). Twelve weeks after treatment, the VAS score decreased to 0.84 ± 0.94 (p < 0.0001). Comparison of the mean pain scores at weeks 6 and 12 also revealed a statistically significant difference (p = 0.0400) (Figure 4).
Perceived pain intensity reported by patients during the study period.
Results for quality of life
3.2
In terms of quality of life, assessed using the Oral Health Impact Profile (OHIP-14), the mean score decreased from 24.56 ± 8.39 at the start of the study to 6.64 ± 3.37 at six weeks (p < 0.0001) and to 5.96 ± 2.79 at twelve weeks (p < 0.0001). The difference between the values at weeks 6 and 12 was not statistically significant (p > 0.9999) (Figure 5).
Patients’ perceived quality of life throughout the study period.
Results for mandibular functional limitation
3.3
Regarding mandibular functional limitation, measured using the Jaw Functional Limitation Scale (JFLS-8), a progressive improvement was observed, with a decrease in the mean score from 5.82 ± 0.56 before the intervention to 2.15 ± 1.45 after six weeks (p = 0.0001) and to 1.08 ± 0.51 after twelve weeks (p < 0.0001). The comparison between the values at weeks 6 and 12 showed no statistical significance (p = 0.1431) (Figure 6).
Patients’ perceived mandibular functional limitation throughout the study period.
Results for chronic pain
3.4
As for the impact of chronic pain measured by the Chronic Pain Inventory (CPI), the mean score decreased from 61.87 ± 8.12 at baseline to 21.73 ± 12.37 at six weeks (p = 0.0016), and 9.86 ± 4.46 at twelve weeks (p < 0.0001). The comparison between the two post-intervention time points also showed a significant difference (p = 0.0016) (Figure 7).
Perception of chronic pain by patients throughout the study.
No statistically significant correlations were observed between pain intensity (VAS) and quality of life (OHIP-14) at any of the assessment points: baseline (r = 0.1412; p = 0.5007), six weeks (r = −0.2073; p = 0.3200), and twelve weeks (r = 0.0291; p = 0.8901).
Adverse events communication
3.5
None of the patients reported AE during or after treatment.
Discussion
4
In the present pilot study, a clinically significant reduction in pain was observed in individuals with M-TMDs, both on the VAS and CPI, at 6 and 12 weeks after BoNT-A administration. These findings indicate a favorable short-term response to BoNT-A, supporting its potential role in pain control in cases of M-TMDs, while acknowledging that the single-arm design precludes causal inference. The absence of significant adverse events further reinforces the apparent safety profile of the intervention within the short follow-up period.
The marked decrease in VAS scores, already evident at six weeks, indicates an early analgesic effect of BoNT-A. These results are consistent with those published by Le Victor et al. and Jadhao et al. (19, 36), who, in two randomized studies, reported substantial reductions in myofascial pain after a single administration of the toxin, with effects that persisted, in some cases, for up to six months. Guarda-Nardini et al. (37) in a pilot study in patients with bruxism, supported treatment with BoNT-A to improve pain at rest and during chewing. Existing scientific evidence contextualizes and reinforces our findings. A double-blind randomized clinical trial conducted by De la Torre Canales et al. (38) demonstrated that BoNT-A promotes significant pain reduction and perceived improvement in patients with refractory M-TMDs, with greater efficacy than placebo. Although the participants in our study did not meet the criteria for refractoriness, com-parable results were observed, suggesting that BoNT-A may also be effective in the early stages of the disease, thus broadening its therapeutic potential. Montes-Carmona et al. likewise reported significant improvements in cases of masticatory myofascial pain, both localized and referred (39). The similarity of their findings with those of the present study is particularly relevant, given that our participants presented with both pain patterns, reinforcing the applicability of BoNT-A in different manifestations of M-TMDs. Gonzalez-Perez et al. (40) also highlighted a good therapeutic response with the use of BoNT-A in the treatment of chronic masticatory myalgia, with high efficacy and safety in long-term pain reduction.
However, contemporary systematic reviews and meta-analyses have emphasized substantial heterogeneity across RCTs regarding injection protocols, total dose, and target muscles. Most controlled studies have used per-muscle doses between approximately 10 and 75 U, most often distributed in three to six injection points per muscle, targeting the masseter and/or temporalis. Our dosing regimen (50 U total; 25 U per side, five points in the masseter and two in the anterior temporalis) therefore lies within the lower–moderate range of the doses commonly used in recent RCTs and systematic reviews (36, 37, 39, 41). This moderate-dose, multi-point approach was deliberately selected to balance potential analgesic benefit with safety, particularly in light of recent concerns about dose-related adverse effects.
The early pain improvement may partly account for the functional gains observed in JFLS-8 assessments, supporting the theory that pain reduction precedes and facilitates mandibular movement recovery (42). This tool, used in our study and designed specifically to assess jaw function, revealed significant improvements at 6 and 12 weeks, reflecting progressive functional recovery, in line with the results of De la Torre Canales et al. (43). However, despite the improvements observed in pain and jaw function, the effects of BoNT-A on maximum mouth opening remain controversial. Studies such as those by Guarda-Nardini et al., De Carli et al. and Kim et al. did not observe significant differences between the treated groups and the control groups (37, 44, 45). In contrast, Nixdorf et al. reported a significant reduction in mouth opening, albeit with a high risk of bias due to dropout rates (46). However, a recent meta-analysis by Li et al. demonstrated a significant increase in pain-free opening after one month and unassisted opening at 1 and 6 months (47). Such discrepancies between studies may be related to methodological differences, the initial characteristics of the participants, or the use of complementary interventions. The results obtained on the OHIP-14 scale after treatment with BoNT-A indicate a significant improvement in oral health-related quality of life, corroborating the psychosocial benefits of this intervention in people with myofascial pain. These findings are consistent with those of De la Torre Canales et al., who demonstrated that BoNT-A not only reduces pain but also contributes to the reduction of psychological comorbidities frequently associated with TMJ (48). Therefore, the scores obtained in the OHIP-14 can be understood as a direct consequence of symptom relief, as several studies suggest that reduced pain intensity is closely related to a lower functional and psychosocial impact in patients with TMDs (49, 50). Another relevant aspect is that the observed benefits may also be associated with indirect effects of BoNT-A on mental health. According to the literature, this toxin appears to have a positive influence on variables such as anxiety and depression (51, 52), factors which, when present, amplify the perception of disability and worsen the discomfort associated with orofacial limitations (53). The hypothesis of a central action of BoNT-A, specifically in the modulation of limbic pathways involved in emotional processing (54, 55), is a plausible explanation for the overall improvement described by patients, even in areas assessed by the OHIP-14 tool, such as psychological distress and functional limitation (56).
Regarding BoNT-A application protocols for the treatment of M-TMDs, several recent systematic reviews (including those by Li et al., De la Torre Canales et al., Delcanho et al. and Kharraz et al. (47, 48, 57, 58) have consistently demonstrated a lack of consensus. These studies highlight the heterogeneity in the doses used (50–300 units), the muscles selected for injection, and the administration techniques adopted. Given this methodological diversity, our study opted for a therapeutic protocol that prioritizes safety without com-promising efficacy, based on the most recent scientific evidence. The choice of a moderate dose of 50 units (25 U per hemisphere) was based on several factors. First, the review by De la Torre Canales et al. (48) warns of the possible adverse effects associated with higher doses, such as muscle atrophy, bone alterations, and significant reduction in masticatory strength. These data are corroborated by De la Torre Canales et al., who demonstrated in a sample of 100 women that higher doses are not associated with greater efficacy, but with a higher incidence of adverse effects. In addition, they suggested that a single administration of reduced doses can significantly improve pain without causing adverse effects (59). The administration technique used with multiple injection sites (five in the masseter and two in the anterior temporalis), with reduced doses per site, was designed to optimize toxin distribution. This approach promotes greater dispersion of the active substance while maintaining the same total dose, ensuring more homogeneous distribution within the target muscle. By avoiding high local concentrations, this technique also reduces the risk of local adverse effects and contributes to the observed safety profile (60). The selection of the masseter and anterior temporalis muscles as therapeutic targets is based on anatomical and accessibility criteria. These muscles are easily located by palpation, unlike the pterygoid muscle, which requires ultrasound guidance for safe application (61). This choice increases the reproducibility of the protocol in clinical settings and minimizes the risk of accidental injections into adjacent structures. The clinical relevance of this muscle selection is likewise supported by the review by De la Torre Canales et al., which highlights the central role of these muscles in the pathophysiology of M-TMDs (62). The timing of the assessments (6 and 12 weeks after treatment) was strategically chosen to capture both the peak action and duration of the therapeutic effects. This decision was based on the literature describing the peak muscle action of BoNT-A between 1 and 4 weeks, with effects that can persist for 3–4 months (63, 64). By including these two assessments, the present study offers a comprehensive perspective on the temporal profile of the therapeutic response.
Recent systematic reviews and experimental studies have also raised important considerations about the structural safety of BoNT-A for masticatory muscles. Although clinical studies generally report only mild and transient adverse events, several imaging and histological investigations have demonstrated masseter muscle atrophy and mandibular bone cortical thinning following repeated or high-dose injections. Animal models and human imaging studies suggest that BoNT-A–induced muscle inactivity may reduce mechanical loading on the mandible, leading to localized bone remodeling and density loss. These potential effects appear to be dose- and time-dependent and may partially reverse after several months, but long-term data in humans remain scarce. Consequently, the apparent short-term safety observed in this and similar studies should be interpreted with caution, and further randomized, placebo-controlled trials with longitudinal imaging follow-up are warranted to assess bone and muscle outcomes more comprehensively (7, 14, 65, 66).
Despite the promising results of this multicenter pilot study, some limitations must be acknowledged. The relatively small sample size and short follow-up further restrict the generalizability of the findings. The administration of BoNT-A in a single session prevented the evaluation of cumulative or prolonged effects of treatment, which would be relevant for defining more sustainable therapeutic protocols. The absence of a placebo control group is another limitation, as it makes it difficult to distinguish between the specific effects of the intervention and possible placebo effects. In addition, the sample consisted exclusively of participants recruited from academic institutions, which may limit the generalizability of the results to a broader population with M-TMDs.
Furthermore, no direct comparisons were made with other currently used therapeutic approaches, preventing conclusions about the relative efficacy of BoNT-A. It is also important to note that, despite the use of validated tools, the data collected were based on the subjective perceptions of participants, which may introduce bias in the interpretation of results.
In light of these methodological constraints, the present findings should be considered preliminary evidence supporting the potential benefit of BoNT-A in myogenous TMDs. Confirmation in larger randomized, placebo-controlled studies with longer follow-up and standardized imaging and functional endpoints is essential. Future research should also systematically monitor muscle thickness and mandibular bone density to clarify the structural safety profile of this therapy.
These limitations underscore the need for future studies with larger samples, adequate control groups, and long-term follow-up. It is also essential to develop standardized treatment protocols and clear clinical guidelines for the application of BoNT-A in M-TMDs. In addition, studies evaluating the economic feasibility of this intervention (cost/benefit ratio) should be conducted to determine the cost-effectiveness of its clinical use.
Conclusions
5
The results obtained in this study indicate that BoNT-A represents an effective and safe therapeutic option for pain relief in cases of M-TMDs, in addition to providing beneficial effects on mandibular function and patients' quality of life.
We observed a significant and sustained improvement in pain symptoms at 6 and 12 weeks after BoNT-A administration, along with a positive impact on functional limitations and psychosocial well-being, as assessed using validated clinical tools. Furthermore, the absence of relevant adverse effects reinforces the safety profile of the protocol adopted, which was based on a moderate dose and careful anatomical distribution.
These findings contribute to consolidating the existing scientific evidence on the efficacy of BoNT-A in the context of M-TMDs and suggest its possible role as part of a multidisciplinary therapeutic approach.
However, for robust validation of these results and the establishment of clear clinical guidelines, further studies with larger sample sizes, the inclusion of a placebo control group, longer follow-up, and comparisons with other therapeutic strategies are required. Future research should also consider evaluating the economic impact of this intervention and developing standardized clinical application protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schiffman E Ohrbach R Truelove E Look J Anderson G Goulet JP Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. (2014) 28:6–27. 10.11607/jop.115124482784 PMC 4478082 · doi ↗ · pubmed ↗
- 2Ohrbach R Greene C. Temporomandibular disorders: priorities for research and care. J Dent Res. (2022) 101:742–3. 10.1177/0022034521106204735001698 · doi ↗ · pubmed ↗
- 3Wang X Yang Y Lin L Yao Q Zhang J. Obesity and temporomandibular joint disorders: a systematic review and meta-analysis. BMC Oral Health. (2023) 23:607. 10.1186/s 12903-023-03322-237644424 PMC 10466750 · doi ↗ · pubmed ↗
- 4Valesan LF Da-Cas CD Réus JC Denardin ACS Garanhani RR Bonotto D Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig. (2021) 25:441–53. 10.1007/s 00784-020-03710-w 33409693 · doi ↗ · pubmed ↗
- 5Minervini G Franco R Marrapodi MM Fiorillo L Cervino G CicciùM. Prevalence of temporomandibular disorders in children and adolescents evaluated with diagnostic criteria for temporomandibular disorders: a systematic review with meta-analysis. J Oral Rehabil. (2023) 50:522–30. 10.1111/joor.1344636912441 · doi ↗ · pubmed ↗
- 6Al-Hanbali LMS Burhan AS Hajeer MY Sultan K Nawaya FR. The effectiveness of interventions in reducing pain related to orthodontic separation: a systematic review and meta-analysis. Eur J Orthod. (2024) 46:cjad 078. 10.1093/ejo/cjad 07838168817 · doi ↗ · pubmed ↗
- 7Kapos FP Exposto FG Oyarzo JF Durham J. Temporomandibular disorders: a review of current concepts in aetiology, diagnosis and management. Oral Surg. (2020) 13:321–34. 10.1111/ors.1247334853604 PMC 8631581 · doi ↗ · pubmed ↗
- 8Sójka A Stelcer B Roy M Mojs E Pryliński M. Is there a relationship between psychological factors and TMD? Brain Behav. (2019) 9:e 01386. 10.1002/brb 3.136031339236 PMC 7649956 · doi ↗ · pubmed ↗