Frailty Recovery Following Minimally Invasive Surgery: An Emerging Perspective on Surgical Benefits in Elderly Colorectal Cancer Patients
Hajime Ushigome, Yushi Yamakawa, Shunsuke Hayakawa, Akira Kato, Takuya Suzuki, Takafumi Sato, Hiroyuki Sagawa, Ryo Ogawa, Hiroki Takahashi, Shuji Takiguchi

TL;DR
This study shows that minimally invasive surgery for colorectal cancer in elderly patients can improve frailty over time, despite worse long-term survival in frail individuals.
Contribution
The study provides new evidence that frailty can improve after successful minimally invasive surgery in elderly colorectal cancer patients.
Findings
Frailty status significantly improved in 1-year recurrence-free patients after minimally invasive surgery.
Frail patients had worse overall survival compared to non-frail patients.
MIS was safely performed in frail elderly patients without increased complications.
Abstract
Frailty is common among elderly colorectal cancer (CRC) patients and affects both perioperative and long‐term outcomes. However, many aspects of how minimally invasive surgery (MIS) influences frailty remain unclear. Moreover, very few reports have specifically evaluated postoperative changes in frailty status. In this prospective observational study, 239 CRC patients aged ≥ 70 years undergoing MIS with R0 resection were assessed for frailty using the FRAIL Scale and Kihon Checklist preoperatively and 1 year postoperatively. Short‐ and long‐term oncological outcomes and frailty status changes were analyzed. A total of 88 patients (37%) were diagnosed as frail on the basis of either of the frailty assessment tools, and MIS was performed in all cases. Short‐term outcomes were comparable between frail and non‐frail patients; however, overall survival (OS) was significantly worse in frail…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
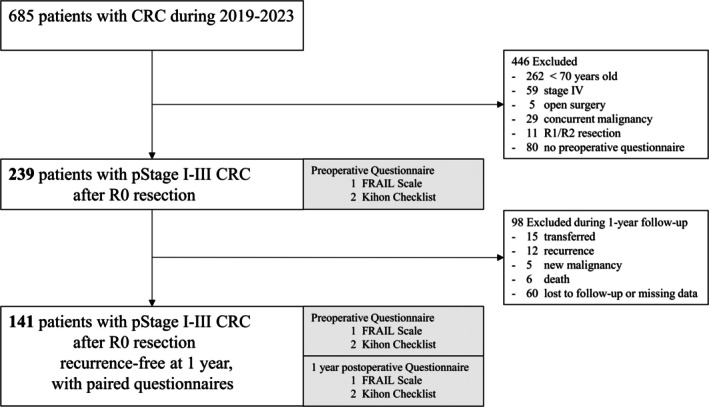 FIGURE 1
FIGURE 1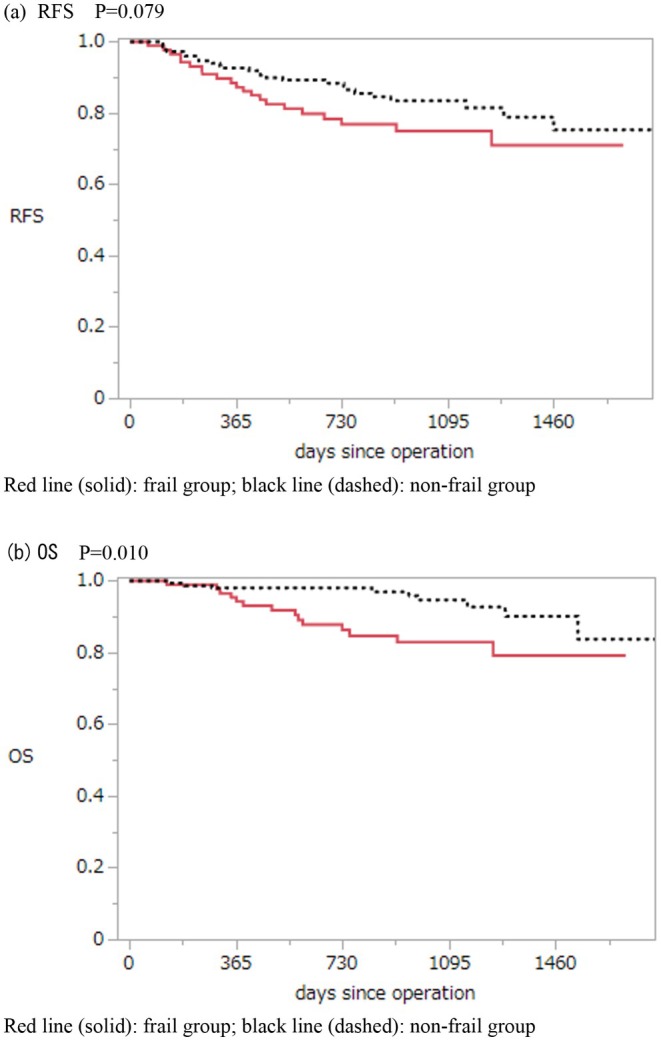 FIGURE 2
FIGURE 2| Variables, N0. (%) or Median (range) | All patients | Frail | Non frail |
|
|---|---|---|---|---|
| ( | ( | ( | ||
| Age (years) | 77 (70–95) | 80 (70–95) | 75 (70–89) | 0.001 |
| Male/Female | 128: 111 | 37:51 | 91:60 | 0.007 |
| BMI (kg/m2) | 22.1 (14.2–35.4) | 21.8 (14.1–32.9) | 22.3 (15.3–35.4) | 0.687 |
| Tumor location | ||||
| Colon | 139 (59.1) | 57 (64.7) | 82 (54.3) | 0.114 |
| Rectum | 100 (40.9) | 31 (35.2) | 69 (45.7) | |
| Obstruction | ||||
| Yes | 32 (13.3) | 13 (14.7) | 19 (12.6) | 0.632 |
| No | 207 (86.7) | 75 (85.3) | 132 (87.4) | |
| Performance status | ||||
| 0–1 | 216 (90.3) | 69 (78.4) | 147 (97.4) | 0.001 |
| 2–4 | 23 (9.7) | 19 (21.6) | 4 (2.6) | |
| ASA‐PS | ||||
| 1–2 | 187 (78.2) | 62 (70.5) | 125 (82.8) | 0.023 |
| 3–4 | 52 (21.8) | 26 (29.5) | 26 (17.2) | |
| Charlson comorbidity index | ||||
| 0–2 | 203 (84.9) | 71 (80.7) | 132 (87.4) | 0.369 |
| 3–4 | 30 (12.6) | 14 (15.9) | 16 (10.6) | |
| 5 ≦ | 6 (2.5) | 3 (3.4) | 3 (2.0) | |
| Prognostic Nutritional Index | 47 (29–68) | 44.5 (30–58) | 48.5 (29–68) | 0.001 |
| Psoas Muscle Index | 4.56 (1.8–10.9) | 4.3 (1.8–7.7) | 4.9 (2.2–10.9) | 0.001 |
| Low PMI | ||||
| Yes | 146 (63.4) | 57 (67.9) | 89 (60.9) | 0.366 |
| No | 84 (36.6) | 27 (32.1) | 57 (39.1) | |
| Preoperative chemotherapy | ||||
| Yes | 5 (2.1) | 2 (2.3) | 3 (1.9) | 0.881 |
| No | 234 (97.9) | 86 (97.7) | 148 (98.1) | |
| Preoperative radiotherapy | ||||
| Yes | 5 (2.1) | 2 (2.3) | 3 (1.9) | 0.881 |
| No | 234 (97.9) | 86 (97.7) | 148 (98.1) | |
| Variables, N0.(%) or Median (range) | Frail | Non frail |
|
|---|---|---|---|
| ( | ( | ||
| Surgical approach | |||
| Laparoscopic | 42 (47.7) | 87 (57.6) | 0.139 |
| Robotic | 46 (52.3) | 64 (42.4) | |
| Operation time | 240 (94–750) | 247 (117–882) | 0.648 |
| Bleeding | 29 (0–680) | 29 (0–1949) | 0.761 |
| TME or CME | |||
| Complete | 77 (87.5) | 141 (93.4) | 0.122 |
| Not complete | 11 (12.4) | 10 (6.6) | |
| Pathological stage (%) | |||
| 0 | 3 (3.4) | 2 (1.3) | 0.187 |
| I | 18 (20.5) | 48 (31.8) | |
| II | 41 (46.6) | 57 (37.8) | |
| III | 26 (29.6) | 44 (29.1) | |
| Morbidity (CD) | |||
| 0 | 67 (76.1) | 124 (82.1) | 0.263 |
| I–II | 15 (17.0) | 23 (15.2) | |
| ≧ III | 6 (6.8) | 4 (2.7) | |
| Mortality | 0 | 0 | |
| Postoperative in‐hospital stay | 11 (6–105) | 10 (6–92) | 0.030 |
| Adjuvant chemotherapy | 11 (12.5) | 31 (20.5) | 0.116 |
| Oxaliplatin based | 2 (18.2) | 18 (58.6) | 0.023 |
| Others | 9 (81.8) | 13 (41.9) | |
| Questionnaire | Preoperative | 1‐year postoperative |
|
|---|---|---|---|
| FRAIL Scale | |||
| Frail | 14 (10.0) | 7 (5.0) | 0.108 |
| Non‐frail | 126 (90.0) | 133 (95.0) | |
| Kihon Checklist | |||
| Frail | 47 (33.6) | 42 (30.0) | 0.336 |
| Non‐frail | 93 (66.4) | 98 (70.0) | |
| FRAIL Scale | |||
| Frail/pre‐frail | 72 (51.4) | 44 (31.4) | 0.001 |
| Non‐frail | 68 (48.6) | 96 (68.6) | |
| Kihon Checklist | |||
| Frail/pre‐frail | 88 (62.9) | 80 (57.1) | 0.157 |
| Non‐frail | 52 (37.1) | 60 (42.9) | |
| Variables | Frail/pre‐frail ( | Non‐frail ( |
| ||||
|---|---|---|---|---|---|---|---|
| Pre‐ope | 1‐year post‐ope |
| Pre‐ope | 1‐year post‐ope |
| ||
| BMI (kg/m2) | 22.4 ± 3.5 | 22.7 ± 3.5 | 0.140 | 22.6 ± 2.8 | 22.4 ± 3.1 | 0.227 | 0.232 |
| Hb (g/dL) | 11.9 ± 2.1 | 12.8 ± 1.6 | 0.001 | 13.1 ± 1.8 | 13.5 ± 1.4 | 0.436 | 0.089 |
| Alb (g/dL) | 3.91 ± 0.4 | 4.04 ± 0.3 | 0.061 | 4.0 ± 0.3 | 4.1 ± 0.3 | 0.297 | 0.845 |
| Prognostic Nutritional Index | 46.2 ± 5.3 | 48.3 ± 4.8 | 0.001 | 48.8 ± 5.0 | 49.9 ± 6.6 | 0.012 | 0.772 |
| Psoas Muscle Index | 4.8 ± 1.4 | 4.9 ± 1.5 | 0.019 | 5.1 ± 1.7 | 5.2 ± 1.7 | 0.093 | 0.614 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Frailty in Older Adults · Nutrition and Health in Aging
Introduction
1
Colorectal cancer (CRC) is one of the most common gastrointestinal malignancies in both Asia and Western countries. In recent years, the aging of the global population has led to a steady increase in elderly patients with CRC, with approximately 50% of patients aged 70 years or older and more than 40% aged 75 years or older [1].
Surgical resection remains the cornerstone of treatment for CRC in elderly patients; however, age‐related vulnerabilities—physical, psychological, and social, collectively referred to as frailty—are frequently observed in this population. Frailty has been identified not only as a risk factor for poor short‐term outcomes but also as a predictor of long‐term prognosis, functional recovery, and quality of life [2, 3, 4, 5, 6]. Therefore, frailty assessment, which evaluates the overall vulnerability of elderly patients beyond conventional indicators such as age and the presence of comorbidities, is crucial in the management of elderly patients with CRC [5, 6, 7].
Minimally invasive surgery (MIS) has become widely adopted for CRC due to its association with reduced postoperative morbidity and faster recovery compared with open surgery [8, 9]. Although short‐term outcomes of MIS, even in frail patients, have been relatively well documented [10, 11, 12, 13], the overall evidence remains limited, and data on long‐term outcomes are still scarce. Moreover, research focusing specifically on postoperative changes in frailty status remains insufficient, despite its potential relevance to optimizing postoperative care and improving survivorship in elderly patients.
A variety of tools are available for assessing frailty, but it is recommended that clinicians use validated and reliable instruments tailored to their specific clinical or research settings [5, 14]. The FRAIL scale is one such internationally recognized screening tool for physical frailty, consisting of five components: fatigue, resistance, ambulation, illnesses, and weight loss. It is simple and feasible for bedside use [5, 14, 15, 16]. The Kihon Checklist (KCL), developed by the Japanese Ministry of Health, Labour and Welfare, consists of 25 self‐reported items evaluating multiple domains including physical function, cognitive function, social participation, nutritional status, and psychological condition. KCL comprehensively covers all components of the geriatric assessment and has been widely applied in clinical and research settings in Japan [14, 15, 17, 18].
The aim of this study is to investigate short‐ and long‐term oncological outcomes, as well as changes in frailty status 1 year after MIS in elderly patients with CRC, using standardized frailty assessment tools.
Materials and Methods
2
Study Design
2.1
This prospective observational study was conducted using a questionnaire survey designed by the Nagoya City University Graduate School of Medical Sciences. Patients scheduled to undergo primary CRC resection were routinely assessed for frailty preoperatively and 1 year postoperatively using two validated questionnaires. Prospectively collected questionnaire data were retrospectively analyzed.
Questionnaires
2.2
Frailty was assessed using two types of questionnaires: the FRAIL Scale and the Kihon Checklist. The FRAIL Scale is classified as a rapid screening tool for physical frailty. It consists of five questions, scored from 0 to 5. Based on the total score, patients were categorized as non‐frail (0 points), pre‐frail (1–2 points), or frail (3–5 points) (Table S1).
The Kihon Checklist is categorized as a metrics‐computed assessment tool evaluating physical, psychological, and social frailty. It includes 25 questions, scored from 0 to 25 points. Based on the total score, patients were classified as non‐frail (0–3 points), pre‐frail (4–7 points), or frail (≥ 8 points) (Table S2).
Patient Population
2.3
From November 2019 to August 2023, 685 patients underwent primary CRC resection at Nagoya City University. Patients were excluded for the following reasons: age under 70 years (n = 262), stage IV disease (n = 59), open surgery (n = 5), presence of active malignancies under treatment (n = 29), R1 or R2 resection status (n = 11), or missing questionnaire data due to emergency surgery or patient refusal or missing data (n = 80). After these 446 patients were excluded, 239 patients were included in the analysis of the first questionnaire.
Among the 239 patients, some were later excluded because of transfer to other hospitals (n = 15); disease recurrence (n = 12); development of other malignancies (n = 5); death (n = 6); or loss to follow‐up, refusal, or missing data (n = 60). Consequently, 141 patients were included in the analysis of the second questionnaire (Figure 1). Patient background was assessed using standard clinical variables as well as the American Society of Anesthesiologists physical status (ASA‐PS) [19], the Charlson Comorbidity Index (CCI) [20], the Prognostic Nutritional Index (PNI) [21], and the Psoas Muscle Index (PMI) [22, 23].
Flow diagram for patient selection in colorectal cancer study.
As part of the evaluation of short‐term postoperative outcomes, we assessed whether total mesorectal excision (TME), tumor‐specific mesorectal excision (TSME) [24] (hereafter collectively referred to as TME), and complete mesocolic excision (CME) [25] were successfully performed. Procedures were defined as “complete” if dissection along the embryological planes was achieved. For CME, high ligation of the feeding vessels at the root of the corresponding artery was also required. Although high ligation is not a standard component of TME or TSME definitions, it was used here specifically to define the completeness of CME. The completeness of these procedures was assessed intraoperatively by the operating surgeon based on standard anatomical criteria.
Statistical Analysis
2.4
Quantitative Data Are Expressed as Medians and Ranges
2.4.1
- Differences in patient characteristics and short‐term outcomes between the frail and non‐frail groups among patients who completed the preoperative questionnaire were analyzed using the Wilcoxon rank‐sum test and the χ^2^ test. Overall survival (OS) and relapse‐free survival (RFS) in the two groups were analyzed using the Kaplan–Meier method and compared with the log‐rank test.
- Among patients who completed both preoperative and 1‐year postoperative questionnaires, changes in frailty and pre‐frailty status were evaluated using the McNemar test. Changes in various variables from the preoperative to postoperative periods within the pre‐frail/frail and non‐frail groups were assessed using the Wilcoxon signed‐rank test and the McNemar test, as appropriate. Differences in variable changes between the pre‐frail/frail and non‐frail groups were analyzed using repeated measures analysis of variance (ANOVA).
A p‐value of < 0.05 was considered statistically significant. All statistical analyses were performed using JMP software, version 8.0.2 (SAS Institute, Cary, NC, USA).
Results
3
The median age of the 239 patients who completed both preoperative questionnaires was 77 years. Among them, 59% had colon cancer and 41% had rectal cancer. Based on the psoas muscle index (PMI), 63% were diagnosed with low PMI.
Eighty‐eight patients (37%) were diagnosed as frail by either the FRAIL Scale or the Kihon Checklist. These patients were significantly older and more likely to be female compared with the non‐frail group. In addition, frail patients tended to have worse performance status (PS), higher ASA‐PS classifications, and poorer nutritional assessments than non‐frail patients. Although the CCI tended to be higher in the frail group, the difference was not statistically significant (Table 1).
Table 2 summarizes short‐term outcomes. The non‐frail group tended to have a higher rate of complete TME or CME excision compared with the frail group (p = 0.122). The rate of incomplete TME or CME was 12.4% (11 cases) in the frail group and 6.6% (10 cases) in the non‐frail group, with no statistically significant difference between the groups. Among the cases with incomplete resection, the proportion of patients with stage II or higher advanced cancer was 64% in the frail group and 30% in the non‐frail group. In these cases, the incomplete resection was attributed to the selection of a safer surgical approach, taking into consideration the patients' age and comorbidities.
There was no significant difference in postoperative complication rates between the two groups; however, the length of postoperative hospital stay was significantly longer in the frail group (p = 0.030).
Adjuvant chemotherapy was more frequently administered in the non‐frail group, and regimens containing oxaliplatin were significantly more common in the non‐frail group (p = 0.023).
Regarding long‐term outcomes in the 239 patients who completed the preoperative questionnaire, the 3‐year RFS rates were 83.4% in the non‐frail group and 74.9% in the frail group, with no significant difference according to the log‐rank test (p = 0.078). In contrast, the estimated 3‐year OS rates were 94.6% and 82.8%, respectively, showing a significant difference between the groups (p = 0.010, log‐rank test) (Figure 2). In the frail group, 14 patients died, with cancer‐related deaths accounting for 7 cases (50%). In the non‐frail group, 10 patients died, and 4 deaths (40%) were cancer‐related. The median follow‐up period was 33.4 months.
Kaplan–Meier curves for relapse‐free survival (RFS) and overall survival (OS) according to frailty status.
Table 3 compares the results of 141 patients who completed both the preoperative and 1‐year postoperative questionnaires. Although the number of patients diagnosed as frail decreased in both the FRAIL Scale and the Kihon Checklist assessments, the differences were not statistically significant. However, when evaluating the number of patients classified as either frail or pre‐frail, a significant reduction was observed in the FRAIL Scale results 1 year postoperatively (p = 0.001).
Table 4 shows the changes in various clinical variables between the preoperative and one‐year postoperative assessments among the 140 patients categorized at baseline as frail/pre‐frail or non‐frail based on the FRAIL scale. In the frail/pre‐frail group, all parameters showed improvement, with Hb, PNI, and PMI improving significantly after surgery. In contrast, although all parameters except BMI improved in the non‐frail group, only PNI showed a statistically significant improvement.
While the improvement in Hb was more pronounced in the frail/pre‐frail group compared to the non‐frail group, the difference between the two groups did not reach statistical significance (p = 0.089).
Discussion
4
This study prospectively evaluated short‐ and long‐term outcomes and changes in frailty status using standardized questionnaire‐based assessments, in CRC patients aged 70 years or older, all of whom underwent MIS, including laparoscopic and robotic procedures. Although OS was significantly worse in the frail group, no significant difference in RFS was detected. Short‐term outcomes were favorable regardless of frailty status. Notably, a significant proportion of patients classified as frail or pre‐frail preoperatively showed improvement in their frailty status at one postoperative year—this is a novel and important finding.
In the frail group, patients were significantly older, had poorer nutritional status, and reduced activities of daily living. While the CCI was comparable between groups, slightly more patients in the frail group had higher scores. Nonetheless, short‐term outcomes, including postoperative complications, did not differ significantly between groups.
Previous studies have reported poorer short‐term outcomes in frail patients undergoing CRC surgery [2, 5]; however, those studies included a substantial proportion of open surgeries. Our findings suggest that, in the current era of MIS, favorable short‐term outcomes can be expected even in frail patients, consistent with prior reports [11, 13, 26]. Nonetheless, some studies have indicated that even MIS does not always ensure favorable outcomes in patients with severely compromised immunity and physiological reserve, [5, 18] requiring cautious interpretation.
This study is novel in that approximately half of the MIS cases were performed using robot‐assisted surgery. Recently, robot‐assisted surgery has been suggested to provide better short‐term outcomes compared to conventional laparoscopic surgery, [27] and it is possible that robotic surgery had some influence on the results of this study. In any case, the effectiveness of MIS, particularly robot‐assisted surgery should be further investigated in frail patients.
Although no significant difference in RFS was observed, OS was significantly worse in the frail group. Previous reviews and meta‐analyses [3, 6, 7] have consistently reported poorer OS and RFS in frail patients after CRC surgery. Considering that frailty itself is associated with poor prognosis in the elderly, [7] these results are unsurprising.
A retrospective study investigating long‐term outcomes in frail patients with Stage I–III colorectal cancer discussed poor RFS being partly attributable to the low tolerability of adjuvant chemotherapy after surgery [3]. Similarly, in this study, adjuvant chemotherapy, particularly oxaliplatin‐based regimens was administered less frequently in the frail group. Moreover, the completion rates of CME and TME, which are both known to improve RFS [28, 29], were lower in the frail group. The frail group was significantly older and had poorer nutritional status, making it clinically challenging to implement these treatments. Although no significant difference in RFS was observed in this study, the divergence of the Kaplan–Meier curves suggests that a significant difference may emerge with a larger sample size. Further large‐scale prospective studies are warranted to validate these findings.
The most noteworthy finding of this study is that even among patients classified as frail or pre‐frail preoperatively, frailty status was significantly improved 1 year postoperatively if they remained recurrence‐free. To date, studies examining longitudinal changes in frailty status among CRC patients have been extremely limited. The recently published GOSAFE study, one of the few addressing postoperative outcomes, demonstrated that preoperative frailty was significantly associated with delayed functional recovery and reduced quality of life 3 and 6 months postoperatively in 625 CRC patients. However, the GOSAFE study focused primarily on short‐term outcomes and did not address long‐term changes in frailty status following MIS [30]. Our study directly evaluated frailty before and 1 year after MIS using standardized tools, providing valuable long‐term follow‐up data rarely reported in the literature.
In the detailed analysis of this study, significant improvements in hemoglobin levels, PNI, and PMI were observed 1 year postoperatively in frail and pre‐frail patients who had undergone curative resection and remained recurrence‐free. These physical indicators respectively reflect different aspects: the PNI represents nutritional status, while PMI reflects muscle mass. In contrast, the FRAIL scale and the Kihon Checklist assess broader domains of functional and physiological vulnerability, including fatigue, physical activity, and weight loss. The overall improvement in these conventional physical indicators likely contributed to the observed improvement in frailty status, suggesting that frailty assessments may capture vulnerabilities not fully reflected by physical indicators alone.
These improvements likely reflect recovery from cancer‐associated cachexia and chronic inflammation following tumor resection [31, 32], providing a theoretical basis for the concept that frailty can be reversible through cancer treatment. This aligns with the emerging concept of “improvement from cancer frailty” proposed in recent reviews [6], and our study offers valuable empirical evidence supporting this view.
Furthermore, as suggested by the GOSAFE study, our findings indicate that surgical resection for CRC may improve overall health status and functional recovery even in older patients. The concept of “improvement from cancer frailty” may thus become an important clinical consideration in oncogeriatric care, extending beyond traditional surgical outcomes.
Several limitations should be considered when interpreting this study. First, it is a single‐center analysis. Patients for whom preoperative surveys could not be conducted due to emergency interventions were not included, and the number of patients who completed the 1‐year postoperative follow‐up was also limited. Therefore, the influence of selection bias cannot be ruled out. Second, as the study did not include an open surgery control group, the specific benefits of MIS could not be fully assessed. Third, although two validated frailty assessment tools were used, psychological and social domains of frailty were not evaluated in detail. Fourth, the completeness of TME, TSME, and CME was assessed intraoperatively by the operating surgeon, which may introduce some degree of subjectivity in the evaluation.
Despite these limitations, two important conclusions can be drawn. First, in elderly frail patients with colorectal cancer, curative MIS did not cause significantly more postoperative complications; however, long‐term survival remained significantly worse than in non‐frail patients. Second, among frail and pre‐frail patients who remained recurrence‐free 1 year postoperatively, frailty status improved significantly. These findings support the proactive application of curative resection in elderly frail patients with CRC, not only from an oncologic standpoint but also due to the potential for improvement in frailty status. Future large‐scale prospective studies incorporating comprehensive frailty assessments are warranted to further elucidate the benefits and limitations of surgical treatment in this population.
Author Contributions
Hajime Ushigome: conceptualization, methodology, investigation, data curation, validation, formal analysis, visualization, writing – original draft, writing – review and editing. Yushi Yamakawa: data curation, investigation, validation. Shunsuke Hayakawa: conceptualization, methodology. Akira Kato: investigation, data curation, validation. Takuya Suzuki: investigation, data curation, validation. Takafumi Sato: writing – review and editing, writing – original draft. Hiroyuki Sagawa: conceptualization, methodology. Ryo Ogawa: conceptualization, methodology. Hiroki Takahashi: investigation, data curation, validation, supervision. Shuji Takiguchi: conceptualization, supervision, methodology.
Ethics Statement
Author S.T. is an editorial board member of Annals of Gastroenterological Surgery. The study protocol was approved by the institutional review board (Nos. 60‐19‐0150 and 60‐19‐0064). Written informed consent was waived due to the retrospective nature of the study. For the prospective frailty assessment (IRB No. 60‐19‐0064), consent was obtained through an explanatory document and participant agreement via checkbox.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: FRAIL Scale scoring criteria.
Table S2: Kihon Checklist scoring criteria.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. Zhang , Q. Li , C. Hu , Z. Zhang , J. She , and F. Shi , “Real‐World Analysis of Survival Benefit of Surgery and Adjuvant Therapy in Elderly Patients With Colorectal Cancer,” Scientific Reports 13, no. 1 (2023): 14866.37684265 10.1038/s 41598-023-41713-1PMC 10491681 · doi ↗ · pubmed ↗
- 2H. Okabe , T. Ohsaki , K. Ogawa , et al., “Frailty Predicts Severe Postoperative Complications After Elective Colorectal Surgery,” American Journal of Surgery 217, no. 4 (2019): 677–681.30473227 10.1016/j.amjsurg.2018.07.009 · doi ↗ · pubmed ↗
- 3K. Mima , N. Miyanari , A. Morito , et al., “Frailty Is an Independent Risk Factor for Recurrence and Mortality Following Curative Resection of Stage I‐III Colorectal Cancer,” Annals of Gastroenterological Surgery 4, no. 4 (2020): 405–412.32724884 10.1002/ags 3.12337 PMC 7382441 · doi ↗ · pubmed ↗
- 4Y. Zhou , X. L. Zhang , H. X. Ni , T. J. Shao , and P. Wang , “Impact of Frailty on Short‐Term Postoperative Outcomes in Patients Undergoing Colorectal Cancer Surgery: A Systematic Review and Meta‐Analysis,” World Journal of Gastrointestinal Surgery 16, no. 3 (2024): 893–906.38577090 10.4240/wjgs.v 16.i 3.893PMC 10989331 · doi ↗ · pubmed ↗
- 5M. Cai , Z. Gao , J. Liao , Y. Jiang , and Y. He , “Frailty Affects Prognosis in Patients With Colorectal Cancer: A Systematic Review and Meta‐Analysis,” Frontiers in Oncology 12 (2022): 1017183.36408138 10.3389/fonc.2022.1017183 PMC 9669723 · doi ↗ · pubmed ↗
- 6H. Maeda , M. Takahashi , S. Seo , and K. Hanazaki , “Frailty and Colorectal Surgery: Review and Concept of Cancer Frailty,” Journal of Clinical Medicine 12, no. 15 (2023): 5041.37568445 10.3390/jcm 12155041 PMC 10419357 · doi ↗ · pubmed ↗
- 7J. Han , Q. Zhang , J. Lan , F. Yu , and J. Liu , “Frailty Worsens Long‐Term Survival in Patients With Colorectal Cancer: A Systematic Review and Meta‐Analysis,” Frontiers in Oncology 14 (2024): 1326292.38406806 10.3389/fonc.2024.1326292 PMC 10889110 · doi ↗ · pubmed ↗
- 8R. Veldkamp , E. Kuhry , W. C. Hop , et al., “Laparoscopic Surgery Versus Open Surgery for Colon Cancer: Short‐Term Outcomes of a Randomised Trial,” Lancet Oncology 6, no. 7 (2005): 477–484.15992696 10.1016/S 1470-2045(05)70221-7 · doi ↗ · pubmed ↗