Breaking the Bowel: A Subacute Ischemic Complication of Chronic Methamphetamine Use
Benjamin Moran, Tiffany Scotto, Sophia Sheikh

TL;DR
Chronic methamphetamine use can cause severe gut damage and life-threatening complications like bowel ischemia and sepsis.
Contribution
This paper highlights methamphetamine as a rare but serious cause of subacute ischemic bowel disease.
Findings
Chronic methamphetamine use can lead to mesenteric ischemia and bowel necrosis.
Early recognition and intervention are critical for patients with methamphetamine-related gastrointestinal complications.
Abstract
Methamphetamine is a potent sympathomimetic agent primarily associated with cardiovascular and neuropsychiatric effects. However, its gastrointestinal complications, particularly ischemic bowel disease, are under-recognized in emergency medicine literature. A 34-year-old man with a history of chronic methamphetamine use presented to the emergency department (ED) seeking medical clearance for rehabilitation admission. He also reported mild, diffuse abdominal pain persisting for three days. Vital signs revealed tachycardia and hypotension. Physical examination showed mild subjective diffuse abdominal tenderness without peritoneal signs. Laboratory studies indicated leukocytosis, elevated lactate, and acute kidney injury. Non-contrast abdominal and pelvic computed tomography (CT) demonstrated pneumoperitoneum and extensive mesenteric stranding consistent with ischemia. The patient was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
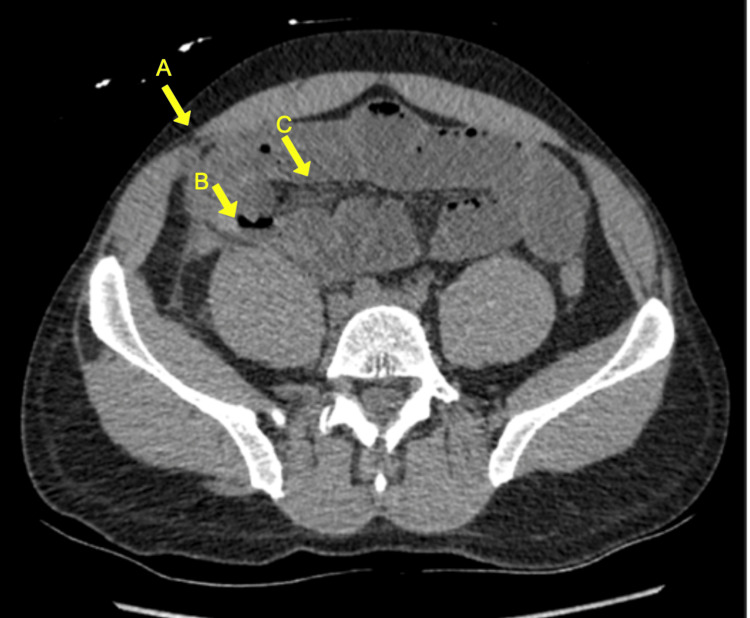 Figure 1
Figure 1| Test | Reference Range | One Year Prior | Date of Presentation |
| WBC (×10³/µL) | 4.0 – 11.0 | 5.81 (WNL) | 14.78 (H) |
| Bands (%) | 0 – 10 | 0.9 (WNL) | 28.6 (H) |
| Sodium (mmol/L) | 135 – 145 | 137 (WNL) | 132 (L) |
| Potassium (mmol/L) | 3.5 – 5.0 | 4.9 (WNL) | 5.2 (H) |
| Chloride (mmol/L) | 98 – 106 | 99 (WNL) | 87 (L) |
| CO₂ (mmol/L) | 22 – 29 | 30 (H) | 18 (L) |
| BUN (mg/dL) | 7 – 20 | 9 (WNL) | 77 (H) |
| Creatinine (mg/dL) | 0.6 – 1.3 | 0.97 (WNL) | 7.88 (H) |
| eGFR (mL/min/1.73m²) | >60 | 76 (WNL) | 9 (L) |
| Lactic acid (mmol/L) | 0.5 – 2.0 | Not Obtained | 2.2 (H), 3.7* (H) |
| Urine drug screen (immunoassay) | Negative | Not Obtained | Methamphetamine (Positive) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Toxicology and Drug Analysis · Pharmacology and Obesity Treatment · Pain Management and Opioid Use
Introduction
The most common side effects and complications of methamphetamine use include acute symptoms such as chest pain, palpitations, hypertension, hyperthermia, impulsivity, psychosis, and delirium [1]. However, its impact on the gastrointestinal system, particularly in causing ischemic bowel disease, remains underappreciated in emergency medicine literature compared to other stimulants such as cocaine [2-4]. The vasoconstrictive properties of methamphetamine can lead to mesenteric ischemia, a condition that, if not promptly diagnosed and treated, carries a high mortality rate [5].
Mesenteric ischemia, bowel obstruction, and sepsis can evolve insidiously in the context of chronic methamphetamine use, often leading to delayed diagnosis and poor outcomes. Emergency physicians are uniquely positioned to identify these presentations early, especially in patients who may not initially appear acutely ill. This report highlights an unusual case of subacute non-occlusive ischemic bowel disease from chronic methamphetamine use. Additionally, this case also aims to raise awareness of chronic methamphetamine use as a risk factor for serious gastrointestinal pathology and to reinforce the need for high suspicion and early surgical consultation in such patients. This is especially important given the fact that chronic methamphetamine use rose 45% among United States adults from 2015 to 2019 [6].
Case presentation
A 34-year-old man with a history of chronic methamphetamine use presented to the ED in October 2024, requesting medical clearance for admission to a rehabilitation facility for assistance with his methamphetamine use disorder. He also reported mild, diffuse abdominal pain for the past three days. He admitted to daily methamphetamine use over the past several weeks but denied nausea, vomiting, fever, decreased appetite, decreased fluid intake, or changes in bowel habits. Of note, the patient denied co-ingestion of alcohol or other xenobiotics. He had no prior surgical history.
Upon arrival, the patient was tachycardic at 112 beats per minute, diaphoretic, and appeared mildly uncomfortable and paranoid, which he attributed to his methamphetamine use. He was hypotensive at 89/64 mm Hg with preserved mean arterial pressures (72 mm Hg) and remained afebrile. Abdominal examination revealed diffuse subjective mild tenderness without rebound or guarding. There were no signs of peritonitis, though his general discomfort appeared disproportionate to the abdominal examination findings. He had decreased bowel sounds. Pulses in all four extremities were equal and he exhibited no focal neurological findings.
Laboratory studies were notable for a white blood cell count of 14.88 x10^3/μL, a rising lactate level (initially 2.2 mmol/L, peaking at 3.7 mmol/L), and acute kidney injury (creatinine of 7.88 mg/dL elevated from 0.97 mg/dL one year prior), and he remained anuric in the ED without any output into his Foley catheter (Table 1).
A non-contrast CT scan of the abdomen and pelvis revealed pneumoperitoneum, a pelvic abscess measuring 6.8 x 3.3 cm, dilated and fluid-filled small bowel loops concerning for developing small bowel obstruction, and extensive mesenteric stranding consistent with ischemia (Figure 1).
Abdominal computed tomography (CT) scan. Axial non-contrast CT of the abdomen demonstrates pneumoperitoneum (A), dilated fluid-filled small bowel loops (B), and mesenteric stranding (C). These findings are concerning for bowel ischemia with perforation, later confirmed intraoperatively.
Given the concern for sepsis and bowel ischemia, the patient received 2.5 liters of intravenous fluid and was started on vancomycin and piperacillin-tazobactam. Due to the progression of his clinical picture, including hypotension, rising lactate, and persistent abdominal pain, he was transferred to the surgical intensive care unit for emergent surgical intervention.
Exploratory laparotomy revealed hemoperitoneum with foul-smelling fluid and a large abscess cavity in the right lower quadrant. There was necrosis of the cecum and signs of mesenteric ischemia. The surgical team performed an ileocecectomy, removing the necrotic right colon and distal ileum. Due to coagulopathy and clinical instability in the setting of septic shock and acidosis, the abdomen was left in discontinuity with a vacuum-assisted closure system in place.
Postoperatively, the patient remained critically ill with ongoing septic shock and renal failure. He required vasopressor support and continued on the same broad-spectrum antibiotics. His abdominal wound was managed with serial dressing changes and several re-explorations. Despite the severity of his illness, he showed gradual clinical improvement with intensive supportive care and his renal function returned to baseline without renal replacement therapy. He was eventually discharged to a rehabilitation facility for assistance with his methamphetamine use disorder after 15 days in the surgical intensive care unit.
Discussion
Methamphetamine exerts potent sympathomimetic effects that induce systemic vasoconstriction, predisposing multiple organ systems, including the gastrointestinal tract, to ischemia [7,8]. Experimental animal studies further support this mechanism, demonstrating methamphetamine-related intestinal inflammation, impaired mucosal integrity, and microvascular injury over time [9-14]. Although the cardiovascular, psychiatric, and neurologic complications of methamphetamine use are well characterized, methamphetamine-associated bowel ischemia remains relatively uncommon in the literature. Most published cases involve an abrupt onset of severe abdominal pain following acute intoxication or binge use, often in individuals without consistent, long-term daily exposure [15,16].
In contrast to prior reports, our patient was a chronic, daily user who developed symptoms gradually over several days. This more insidious presentation aligns with the possibility of partial or intermittent mesenteric hypoperfusion, allowing ischemia to evolve slowly into necrosis and abscess formation rather than producing the rapid, catastrophic ischemia described in binge-use cases. The absence of peritoneal signs in this patient likely contributed to diagnostic delay, emphasizing the challenge of identifying mesenteric ischemia when exam findings are subtle. Therefore, this case represents a novel presentation in emergency medicine literature.
The distinction between chronic and binge use may also explain the divergent clinical course. Chronic vasoconstriction may lead to progressive microvascular compromise with temporary periods of preserved perfusion due to small bowel collateral circulation [17]. This contrasts with binge-induced ischemia, where sudden, profound vasospasm overwhelms collateral flow and results in abrupt, severe ischemic insult [18]. Our patient had no other risk factors, no prior abdominal surgeries, immunocompromise, or other xenobiotic exposures, making methamphetamine the most plausible driver of his vascular pathology.
This case highlights the need for emergency physicians to maintain vigilance when evaluating methamphetamine users with vague abdominal complaints. Even mild or atypical symptoms may mask evolving ischemia, and early imaging should be strongly considered when laboratory abnormalities such as leukocytosis or lactic acidosis are present.
Conclusions
Early recognition of mesenteric ischemia is critical in chronic methamphetamine users, as symptoms may be subtle and nonspecific. This case demonstrates that abdominal pathology can be easily overlooked, especially when abdominal pain is not the main chief complaint, underscoring the importance of a thorough history and physical examination. Prompt imaging, aggressive resuscitation, broad-spectrum antibiotics, and early surgical consultation were essential to this patient’s survival. Emergency physicians should maintain a high index of suspicion for ischemic bowel in methamphetamine users presenting with shock, lactic acidosis, or abdominal pain out of proportion to physical examination findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Methamphetamine use disorder JAMA Leyde S Tilhou AS Tsui JI 1192119333420254090057510.1001/jama.2025.12007 · doi ↗ · pubmed ↗
- 2Methamphetamine colitis: a rare case of ischemic colitis in a young patient Arch Surg Holubar SD Hassinger JP Dozois EJ Masuoka HC 7807821442009 https://pubmed.ncbi.nlm.nih.gov/19687384/1968738410.1001/archsurg.2009.139 · doi ↗ · pubmed ↗
- 3Methamphetamine-induced ischemic colitis J Clin Gastroenterol Johnson TD Berenson MM 687689131991 https://pubmed.ncbi.nlm.nih.gov/1761842/176184210.1097/00004836-199112000-00015 · doi ↗ · pubmed ↗
- 4High mortality of cocaine-related ischemic colitis: a hybrid cohort/case-control study Gastrointest Endosc Elramah M Einstein M Mori N Vakil N 12261232752012 https://pubmed.ncbi.nlm.nih.gov/?term=%22Gastrointest+Endosc%22%5Bjour%5D&sort=date&sort_order=desc 2248292110.1016/j.gie.2012.02.016 · doi ↗ · pubmed ↗
- 5Incidence, diagnosis, management and outcome of acute mesenteric ischaemia: a prospective, multicentre observational study (AMESI Study)Crit Care Blaser AR Mändul M Björck M 32282024 https://ccforum.biomedcentral.com/articles/10.1186/s 13054-024-04807-43826305810.1186/s 13054-024-04807-4PMC 10807222 · doi ↗ · pubmed ↗
- 6Methamphetamine use, methamphetamine use disorder, and associated overdose deaths among US adults JAMA Psychiatry Han B Compton WM Jones CM Einstein EB Volkow ND 132913427820213455030110.1001/jamapsychiatry.2021.2588 PMC 8459304 · doi ↗ · pubmed ↗
- 7Necrotizing angiitis associated with drug abuse N Engl J Med Citron BP Halpern M Mc Carron M 100310112831970 https://pubmed.ncbi.nlm.nih.gov/4394271/439427110.1056/NEJM 197011052831901 · doi ↗ · pubmed ↗
- 8Goldfrank's Toxicologic Emergencies. 11th ed Smith SW Goldfrank LR Hoffman RS Mc Graw-Hill Education 2019 https://accesspharmacy.mhmedical.com/content.aspx?bookid=2569§ionid=210259500