ZAP-X Stereotactic Radiosurgery: The Initial Experience Involving 200 Patients
Timothy Chen, Patrick Pema, Michael Chaga, Wenzheng Feng, Tingyu Wang, Darra Conti, Jing Feng, Akil Anthony, Ma Rhudelyn Rodrigo, Harshal Shah, Daniel Monahan, Elizabeth Luick, Daniel Thompson, Joy Baldwin, Brielle Latif, Georgia Montone, Joseph Hanley, Nitesh V Patel

TL;DR
This study evaluates the ZAP-X radiosurgery system's performance in 200 patients, showing it is a feasible and promising alternative to existing systems.
Contribution
The study presents the largest single-institution experience with ZAP-X, offering new insights into its clinical and dosimetric performance.
Findings
ZAP-X achieved high gamma passing rates and favorable dosimetric indices across a variety of intracranial targets.
Patient satisfaction was high, with the Efficast mask improving comfort and reducing alignment errors.
Treatment time averaged 50 minutes, with setup time being the main factor affecting duration.
Abstract
The ZAP-X (ZAP Surgical Systems, Inc., San Carlos, CA) is the newest dedicated cranial stereotactic radiosurgery (SRS) platform. A prospective study was conducted between October 2023 and January 2025 involving 200 patients with 374 intracranial targets treated using ZAP-X. The study aimed to assess the feasibility of the ZAP-X workflow, as well as its safety, clinical and dosimetric performance, and patient satisfaction. The study cohort included various central nervous system pathologies, including 106 brain metastases (BM), 42 meningiomas (MA), 18 trigeminal neuralgias (TN), 11 acoustic neuromas (AN), nine recurrent glioblastomas (RGBM), seven pituitary adenomas (PA), three spinal tumors (ST), three arteriovenous malformations (AVM), and one cavernous hemangioma of the pons (HM). The average number of patients treated per month was 13 ± 2, and the average number of treatments per…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
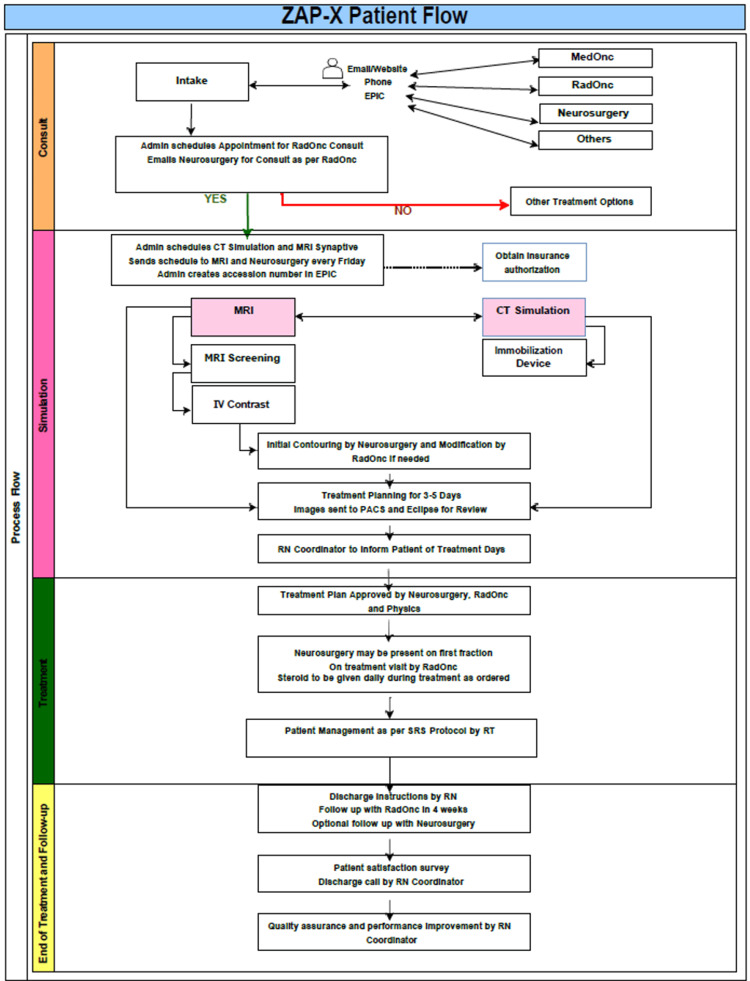 Figure 1
Figure 1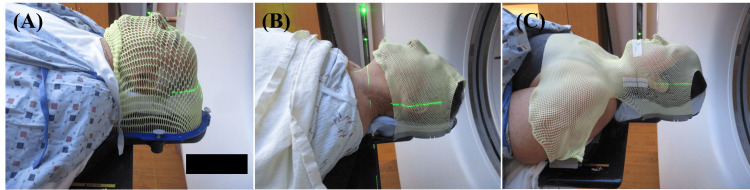 Figure 2
Figure 2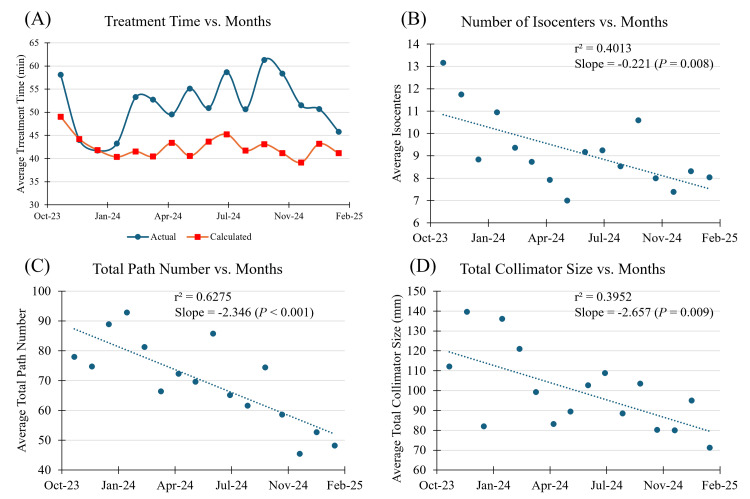 Figure 3
Figure 3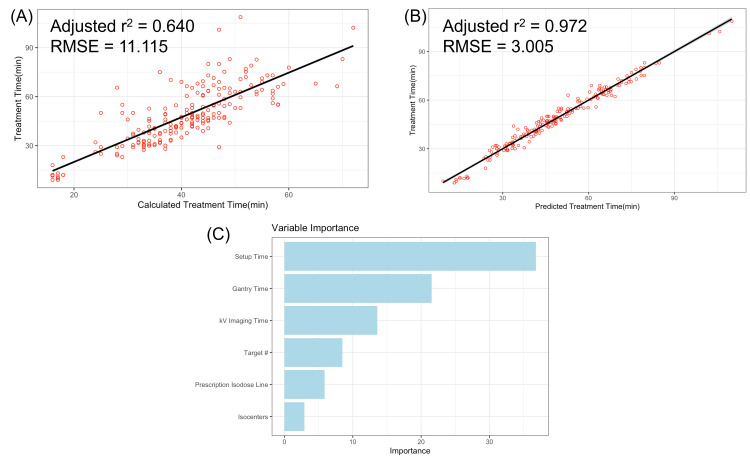 Figure 4
Figure 4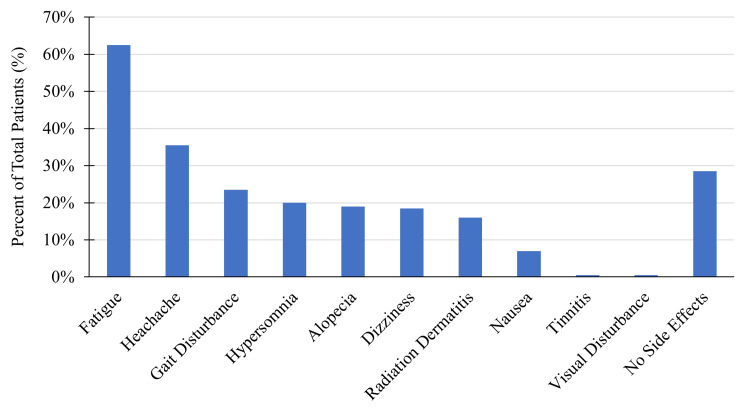 Figure 5
Figure 5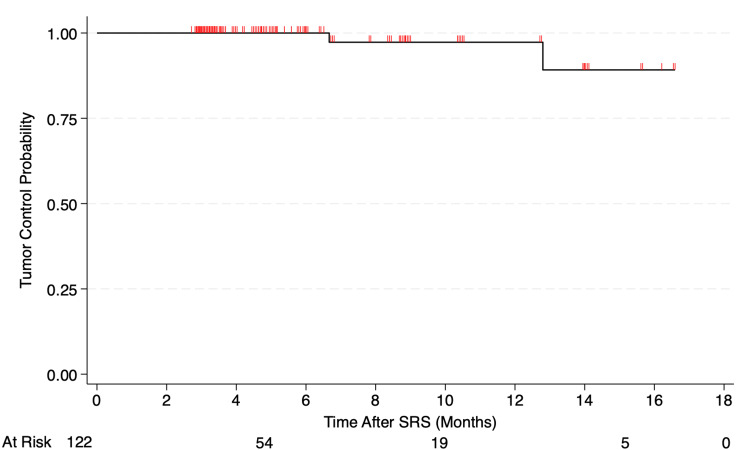 Figure 6
Figure 6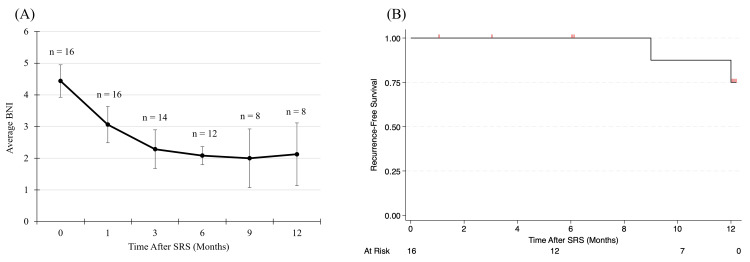 Figure 7
Figure 7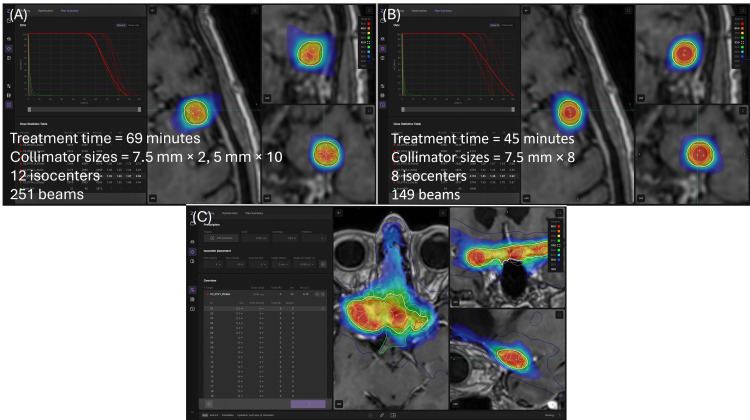 Figure 8
Figure 8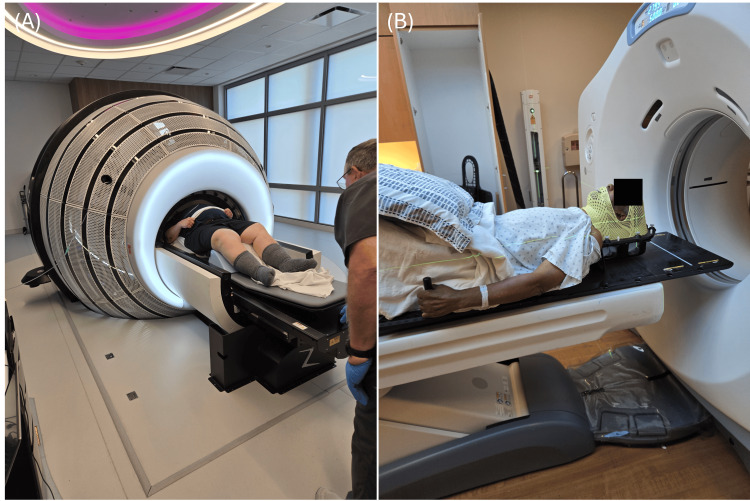 Figure 9
Figure 9| Procedure | Tolerance |
| Daily | |
| Safety/imaging | |
| Software, hardware, and exclusion zone E-Stop | Functional |
| Table, shell, and door | Initialized, move to intended positions |
| Gantry rotation | Initialized, move to intended positions |
| Proximity error check | Interlock tripped when close to the table |
| Beam on indicators | Functional |
| Audio/visual | Functional |
| Pendant | Functional, E-Stop functional |
| kV imaging (accuracy of table and gantry position) | Baseline |
| MV imaging (consistency of beam positioning and output) | Baseline |
| Winston-Lutz (Hayes Phantom, collimator = 15 mm, 6 gantry angles) | |
| Translational target and beam offsets | <1 mm |
| Output check (PTW Semiflex 31021, collimator = 25 mm, 0°, 500 MU, 45 cm SAD) | |
| Absolute dose output in air | ± 2% baseline |
| Primary and secondary MU difference | ≤3% |
| Monthly | |
| Safety | |
| Emergency button | Functional |
| Door release | Functional |
| Shell release | Functional |
| kV imaging (Leeds Phantom, Gammex Tool) | |
| kV homogeneity, kV high contrast, low contrast | ± 5% baseline |
| MV imaging (all collimators, 0°, 200 MU) | |
| MV cone center and size consistency | <1 mm |
| End-to-end (Hayes Phantom, EBT3 film, collimator = 25 mm, 45 cm SAD) | |
| Orthogonal film difference | <1 mm |
| End-to-end (SRS MapCHECK, gamma criteria 10%/2%/1 mm) | ≥95% |
| TPS integrity and plan consistency | <1% |
| Output check (PTW Semiflex 31010, Sphere Phantom, collimator = 25 mm, 0°, 200 MU, 50 cm SAD) | |
| Absolute dose output | ± 2% baseline |
| Energy check (PTW Semiflex 31010, Column Phantom, collimator = 25 mm, 0°, 200 MU, 45 cm SSD) | |
| D10cm/D0.7cm | ± 2% baseline |
| Daily QA | Refer to daily |
| Annually | |
| Absolute output (PTW Semiflex 31010, PTW MP3-XS, collimator = 25 mm, 0°, 500 MU, 45 cm SSD, 5 cm depth) | |
| Dmax at 45 cm SAD | ± 2% nominal |
| Output factor comparison with TPS (MicroSilicon, all collimators, 0°, 45 cm SAD) | |
| Output factor at Dmax normalized with a 25 mm collimator | ± 2% commissioning |
| PDD comparison (MicroSilicon, PTW MP3-XS, 45 cm SSD) | |
| Measured and TPS PDD difference | ± 1% commissioning |
| Profile comparison (MicroSilicon, PTW MP3-XS, 45 cm SSD) | |
| Measured and TPS profile difference | 0.1 mm or ± 1% commissioning |
| Start shot test (Star shot fixture, EBT3 film, collimator = 5 mm, 5 gantry angles, 500 MU, 45 cm SAD) | |
| Radius | ± 1 mm baseline |
| Chamber cross calibration (PTW Semiflex 31021, collimator = 25 mm, 0°, 500 MU, 45 cm SAD) | |
| Charge ratio of calibrated to cross-calibrated chambers | ± 1% baseline |
| External audit with RDS (cylindrical phantom, TLD, 45 cm SAD, 7 mm depth) | |
| Measured and RDS absolute dose difference | ± 5% |
| PSQA with timer and interrupt test (SRS MapCHECK, gamma criteria 10%/2%/1 mm) | |
| Simulation plan delivery to the chamber isocenter | ≥95% |
| Monthly and daily QA | Refer to monthly and daily |
| BM (106) | MA (42) | TN (18) | AN (11) | RGBM (9) | PA (7) | AVM (3) | ST (3) | HM (1) | All (200) | |
| Rx dose (Gy) | 23 ± 4 | 23 ± 4 | 83 ± 5 | 21 ± 5 | 30 | 26 ± 3 | 34 ± 6 | 28 ± 3 | 25 | 29 ± 17 |
| 18 – 30 | 16 – 30 | 80 – 90 | 14 – 30 | 21 – 30 | 27 –37.5 | 24 – 30 | 14 – 90 | |||
| Rx isodose line (%) | 60 ± 10 | 59 ± 5 | 100 | 59 ± 6 | 57 ± 8 | 62 ± 7 | 61 ± 5 | 62 ± 5 | 57 | 66 ± 14 |
| 50 – 89 | 52 – 75 | 51 – 71 | 50 – 75 | 53 – 70 | 55 – 64 | 56 – 66 | 50 – 100 | |||
| Number of targets | 3 ± 2 | 1.1 ± 0.4 | 1 | 1.2 ± 0.4 | 1.2 ± 0.7 | 1 | 1 | 1 | 1 | 1.9 ± 1.7 |
| 1 – 10 | 1 – 3 | 1 – 2 | 1 – 3 | 1 – 10 | ||||||
| Target volume (cm3) | 3 ± 5 | 6 ± 6 | 0.05 ± 0.03 | 3 ± 2 | 10 ± 4 | 8 ± 9 | 9 ± 4 | 3 ± 3 | 1.9 | 4 ± 6 |
| 0.05 – 29.29 | 0.27 – 24.57 | 0.01 – 0.11 | 0.12 – 8.33 | 3.66 – 19.36 | 0.79 – 26.4 | 4.84 –11.56 | 0.61 – 6.29 | 0.01 – 29.29 | ||
| Number of fractions | 2.5 ± 1.6 | 4 ± 4 | 1 | 3.2 ± 1.1 | 5 | 4 ± 1 | 4.3 ± 1.2 | 4.3 ± 1.2 | 5 | 2.8 ± 1.6 |
| 1 – 5 | 1 – 5 | 1 – 5 | 3 – 5 | 3 – 5 | 3 – 5 | 1 – 5 | ||||
| Number of isocenters | 7 ± 4 | 10 ± 3 | 1 | 8 ± 4 | 10 ± 3 | 12 ± 4 | 10 ± 3 | 12 ± 4 | 12 | 8 ± 4 |
| 1 – 18 | 4 – 15 | 1 – 16 | 6 – 15 | 6 – 17 | 8 – 13 | 8 – 16 | 1 – 18 | |||
| Number of beams | 180 ± 80 | 190 ± 50 | 200 ± 70 | 180 ± 50 | 240 ± 50 | 200 ± 60 | 260 ± 70 | 280 ± 70 | 266 | 190 ± 70 |
| 31 – 429 | 74 – 289 | 130 – 330 | 68 – 233 | 162 – 325 | 122 – 321 | 177 –318 | 212 – 257 | 31 – 429 | ||
| Target Rx coverage (%) | 99 ± 2 | 98 ± 1 | - | 97.8 ± 1.2 | 98.0 ± 1.2 | 98.8 ± 1.1 | 97.6 ± 0.6 | 97 ± 1 | 99.36 | 98 ± 2 |
| 71.28 – 100 | 95.91 – 99.80 | 95.47 – 99.73 | 95.43 – 99.42 | 96.44 – 99.82 | 97.22 – 98.33 | 96.19 – 98.16 | 71.28 – 100 | |||
| CI | 1.3 ± 0.3 | 1.26 ± 0.17 | - | 1.2 ± 0.2 | 1.2 ± 0.1 | 1.28 ± 0.08 | 1.22 ± 0.04 | 1.13 ± 0.06 | 1.17 | 1.3 ± 0.3 |
| 0.71 – 3.87 | 1.08 – 1.92 | 1.06 – 1.86 | 1.04 – 1.41 | 1.18 – 1.37 | 1.18 – 1.26 | 1.07 – 1.17 | 0.71 – 3.87 | |||
| PCI | 0.76 ± 0.12 | 0.78 ± 0.08 | - | 0.79 ± 0.09 | 0.85 ± 0.11 | 0.76 ± 0.04 | 0.78 ± 0.03 | 0.84 ± 0.03 | 0.85 | 0.77 ± 0.11 |
| 0.26 – 1.33 | 0.51 – 0.89 | 0.54 – 0.81 | 0.70 – 1.12 | 0.72 – 0.84 | 0.75 – 0.81 | 0.81 – 0.87 | 0.26 – 1.33 | |||
| GI | 3.4 ± 0.8 | 2.9 ± 0.5 | - | 3.0 ± 0.3 | 2.9 ± 0.7 | 2.78 ± 0.14 | 2.9 ± 0.2 | 3.0 ± 0.5 | 2.60 | 3.3 ± 0.8 |
| 2.13 – 7.77 | 2.33 – 5.45 | 2.60 – 3.68 | 2.34 – 4.93 | 2.59 – 3.03 | 2.68 – 3.14 | 2.58 – 3.54 | 2.13 – 7.77 | |||
| HI | 1.5 ± 0.2 | 1.69 ± 0.16 | - | 1.70 ± 0.17 | 1.8 ± 0.2 | 1.63 ± 0.18 | 1.66 ± 0.14 | 1.63 ± 0.14 | 2.60 | 1.5 ± 0.3 |
| 1.08 – 2.02 | 1.31 – 1.92 | 1.41 – 1.96 | 1.33 – 2 | 1.43 – 1.89 | 1.56 – 1.82 | 1.52 – 1.79 | 1.08 – 2.60 | |||
| GM (cm) | 0.35 ± 0.16 | 0.44 ± 0.14 | - | 0.38 ± 0.11 | 0.6 ± 0.1 | 0.50 ± 0.17 | 0.57 ± 0.04 | 0.38 ± 0.08 | 0.30 | 0.38 ± 0.16 |
| 0.13 – 1.06 | 0.20 – 0.79 | 0.19 – 0.65 | 0.48 – 0.76 | 0.28 – 0.73 | 0.53 – 0.61 | 0.29 – 0.43 | 0.13 – 1.06 | |||
| Treatment time (min/Fx) | 50 ± 20 | 49 ± 16 | 35 ± 7 | 48 ± 19 | 66 ± 19 | 40 ± 10 | 65 ± 11 | 58 ± 9 | 40 ± 1.1 | 50 ± 20 |
| 9 – 141 | 25 – 133 | 28 – 52 | 12 – 84 | 38 – 118 | 29 – 66 | 42 – 84 | 44 – 73 | 39 – 42 | 9 – 141 |
| Parameter | Mask | Average ± SD | Median† | Range | P=value‡ |
| Comfort | Head (n = 30) | 4.1 ± 1.0 | 4 (3.5, 5) | 2 – 5 | 0.0345 |
| Efficast (n = 30) | 4.7 ± 0.7 | 5 (4.5, 5) | 3 – 5 | ||
| Readjustments | Head (n = 30) | 5 ± 4 | 4 (1, 7) | 0 – 13 | 0.0194 |
| Efficast (n = 30) | 2 ± 3 | 1 (0, 4) | 0 – 12 | ||
| Setup time (min) | Head (n = 30) | 17 ± 11 | 15 (7, 24) | 1 – 47 | <0.001 |
| Efficast (n = 30) | 10 ± 10 | 4 (2, 11) | 1 – 51 | ||
| x-offset (mm) | Head (n = 30) | 0.0 ± 0.4 | 0 (-0.15, 0.14) | -3.94 – 4.31 | 0.406 |
| Efficast (n = 30) | 0.0 ± 0.3 | 0 (-0.12, 0.11) | -2.76 – 2.48 | ||
| y-offset (mm) | Head (n = 30) | 0.0 ± 0.3 | 0 (-0.11, 0.11) | -6.57 – 2.28 | 0.0014 |
| Efficast (n = 30) | 0.0 ± 0.3 | 0 (-0.08, 0.11) | -3.06 – 3.61 | ||
| z-offset (mm) | Head (n = 30) | 0.0 ± 0.3 | 0 (-0.12, 0.14) | -3.12 – 6.53 | 0.453 |
| Efficast (n = 30) | 0.0 ± 0.3 | 0 (-0.11, 0.12) | -3.01 – 2.22 | ||
| Pitch-offset (°) | Head (n = 30) | 0.1 ± 0.8 | 0.15 (-0.61, 0.79) | -2.79 – 2.04 | <0.001 |
| Efficast (n = 30) | 0.0 ± 0.5 | -0.09 (-0.46, 0.72) | -2.64 – 2.01 | ||
| Roll-offset (°) | Head (n = 30) | -0.2 ± 0.8 | -0.20 (-0.87, 0.36) | -3.05 – 2.40 | <0.001 |
| Efficast (n = 30) | 0.0 ± 0.6 | -0.16 (-0.72, 0.26) | -1.87 – 1.68 | ||
| Yaw-offset (°) | Head (n = 30) | 0.0 ± 0.8 | -0.22 (-0.62, 0.62) | -2.18 – 2.71 | <0.001 |
| Efficast (n = 30) | 0.0 ± 0.8 | -0.12 (-0.52, 0.50) | -2.11 – 2.08 |
| Average | Median† | Range | |
| Treatment time (min/Fx) | 50 ± 20 | 49 (39, 63) | 9 – 141 |
| Calculated treatment time (min/Fx) | 40 ± 10 | 43 (37, 48) | 16 – 72 |
| Setup time (min/Fx) | 11 ± 12 | 7 (4, 15) | 1 – 81 |
| Gantry time (min/Fx) | 30 ± 10 | 25 (19, 31) | 2 – 73 |
| Table time (min/Fx) | 0.8 ± 0.5 | 0.73 (0.55, 0.98) | 0.05 – 6 |
| kV imaging and processing time (min/Fx) | 8 ± 4 | 7.58 (4.975, 10.28) | 0.1 – 26 |
| Linac time (min/Fx) | 6 ± 3 | 5 (4, 7) | 1 – 23 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Brain Metastases and Treatment · Meningioma and schwannoma management
Introduction
The ZAP-X (ZAP Surgical Systems, Inc., San Carlos, CA) is the newest dedicated cranial stereotactic radiosurgery (SRS) platform. The radiation source for the ZAP-X is a 3 MV S-band linear accelerator (Linac) mounted on axial and oblique gimbals, which allows for isocentric, non-coplanar, dual-axis radiation delivery over a solid angle of greater than 2π steradians. The flattening filter free beam is collimated via a rotating tungsten wheel with eight circular field sizes ranging from 4 to 25 mm in diameter, defined at a source-to-axis distance (SAD) of 45 cm. The self-shielded ZAP-X system design consists of a shielded treatment chamber, rotating shell, and a pneumatic door located at the foot of the table. This design reduces radiation exposure inside the treatment room, eliminating the need for a shielded vault and increasing installation flexibility [1-3]. The ZAP-X produced the lowest full-width half maximum and sharpest overall penumbra for its smallest collimator compared to beam profile parameters of Gamma Knife (GK) and CyberKnife (CK) for the corresponding smallest collimator [4].
The objective of this study is to evaluate ZAP-X workflow feasibility, safety, clinical and dosimetric performance, and patient satisfaction. Analysis of this newly pioneered system is important to gauge its efficacy and refine its specificity for varying patients and conditions. Our report on the first 200 patients treated with the ZAP-X SRS platform is particularly significant given the novelty of the technology and the current scarcity of extensive literature on it [5-8]. This review provides first-hand, valuable insights into dosimetric characteristics, clinical efficacy, pathology-specific treatment parameters, and patient satisfaction. To date, it represents the largest single-institution series treated with the ZAP-X platform.
Materials and methods
The data were collected prospectively on patients receiving ZAP-X SRS who were treated between October 2023 and January 2025 at Jersey Shore University Medical Center (JSUMC). The study protocol was reviewed and approved by the Institutional Review Board, Pro2024-0029. The patient cohort comprised individuals who met clinical indications for treatment with ZAP-X SRS.
Clinical workflow
Our workflow process consists of four stages: consultation, simulation, treatment, and end of treatment and follow-up. At the beginning of the simulation phase, CT imaging is used to create an immobilization mask, and on-site planning MRI is performed, and imaging is sent to Eclipse for fusion and contouring. Imaging data is then processed and sent to PACS and the Eclipse (Varian Medical Systems, Palo Alto, CA, version 15.6) treatment planning system (TPS) for contouring and treatment planning. The treatment phase begins with treatment plan approval by the neurosurgeon, radiation oncologist, and physicist. The neurosurgeon and radiation oncologist are required to be present for the first treatment fraction. The last phase - end of treatment and follow-up - begins with patient discharge per the registered nurse's instruction. Follow-up with both radiation oncology and neurosurgery occurs four weeks post-SRS. A patient satisfaction survey utilizing a 5-point Likert scale is completed by each patient. Lastly, quality assurance (QA) and performance improvement are handled by the nurse coordinator. A diagram of the ZAP-X clinical workflow is shown in Figure 1.
ZAP-X clinical workflow
All patients underwent planning MRI with or without gadolinium contrast on a 0.5 T Synaptive MRI co-located in a room adjacent to the ZAP-X as described by Chaga et al. [9]. Patients were scheduled for same-day CT Sim and MRI with a goal of ≤5 days between consult and imaging for benign cases and same-day consult and imaging for malignant cases. After imaging, patients were scheduled for SRS treatment with a goal of ≤5 days between imaging and treatment. Volumes of interest were contoured by a qualified radiation oncologist, neurosurgeon, and medical physicist utilizing a fused dataset comprising treatment planning CT and post-gadolinium MRI within the Eclipse TPS. The contoured images were then imported to the ZAP-X TPS (versions 1.8 - 1.10).
Treatment planning was performed using either forward-planning or combined forward- and inverse-planning modes. In forward-planning mode, isocenters were manually placed in the target by the planner. In combined forward- and inverse-planning mode, isocenters were manually placed first, followed by inverse optimization of beam weights and manual addition, deletion, or repositioning of isocenters. A 0.5 mm dose grid was utilized, limiting the dose to the eyes, lens, optic nerves, optic chiasm, cochleae, brainstem, and spinal cord based on Timmerman organ-at-risk (OAR) recommendations [10]. Plan quality was evaluated for conformality, dose fall-off, and dose homogeneity using conformity index (CI), Paddick conformity index (PCI), gradient index (GI), homogeneity index (HI), and gradient measure (GM).
The CI was defined as the ratio of the prescription isodose volume to the target volume [11]. The PCI was calculated as the square of the target volume covered by the prescription isodose divided by the product of the target volume and the prescription isodose volume [12]. The GI was defined as the ratio of the volume receiving half the prescription dose to the prescription isodose volume [13]. The HI was calculated as the ratio of the maximum dose to the prescription dose [14]. The GM was defined as the difference, in centimeters, between the equivalent sphere radii of the 50% and 100% prescription isodose line volumes [15]. Plan quality constraints followed the Radiation Therapy Oncology Group Protocol 0813 [16].
Patient-specific and machine quality assurance
For each patient case, a patient-specific quality assurance (PSQA) program was utilized to ensure high accuracy of the planned versus delivered dose. PSQA consisted of two components: independent dose calculation and absolute planar dose measurements. For independent dose calculation, a software developed in-house called ZapMU was utilized [17-19]. For absolute planar dose measurements, SRS MapCHECK was utilized along with SNC Patient software (Sun Nuclear, Melbourne, FL) for gamma analysis [20-21]. Machine daily QA is performed once each day before each treatment, along with monthly and annual QA. All ZAP-X QA tests are summarized in Table 1.
ZAP-X thermoplastic masks
To ensure patient comfort and precise positioning, patients were placed in mold care and thermoplastic Fibreplast head masks (CQ Medical, Avondale, PA) [22], Nanor head masks (Orfit Industries, Jericho, NY) [23], and Efficast head and shoulder masks (Orfit Industries, Jericho, NY) [24]. All masks are shown in Figure 2.
ZAP-X thermoplastic masks utilized at JSUMC(A) Fibreplast head mask, (B) Nanor head mask. (C) Efficast head and shoulder mask with two shimsJSUMC: Jersey Shore University Medical Center
For the Efficast masks, two shims were employed during mask creation. For mask comparison, patient comfort, number of readjustments, setup time, and alignment offsets were evaluated for 60 patients: 30 Fibreplast and Nanor head mask patients and 30 Efficast mask patients. The patient alignment process involves a sequence of 3D alignment steps using non-coaxial kV X-ray images from multiple gantry angles. The images are co-registered to digitally reconstructed radiographs (DRRs) generated from the initial CT used in the treatment plan. The initial auto-alignment before treatment was approved by a radiation oncologist. Alignment deviation of more than 2 mm in any direction and 1.5° in any rotation axis would require a readjustment of the patient positioning and repeating auto-alignment and radiation oncologist approval. If >5 gantry locations with MV dosimetry deviation of more than 10% exist, a physicist's investigation is required. Treatment would be stopped for further investigation with the vendor if >10 gantry locations with MV dosimetry deviation of more than 10% exist. Patient alignment offsets and the number of readjustments were obtained from system log files on the treatment console. Mask comfort was evaluated using a Likert scale from 1-5 (1 = “very poor”, 5 = “very good”).
Patient satisfaction
Patient satisfaction was measured using a postoperative questionnaire, which utilized a 5-point Likert scale. Patients were asked to rate their experience in the following categories: ease of scheduling, staff helpfulness, ZAP-X cleanliness, staff friendliness/courtesy, physician procedure explanation, comfort of waiting area, comfort during simulation, comfort during mask creation, comfort during MRI, comfort during treatment, comfort post-treatment, response to concerns/complaints, overall rating of care, care coordination, and recommending JSUMC.
ZAP-X treatment time
As a clinical endeavor to reduce the total treatment time, the treatment time variables for each patient were obtained from reports generated by the ZAP-X system upon completion of treatment. Setup time was defined as the duration required for auto-alignment imaging and its subsequent review. Gantry time was the duration for the gantry to move all gantry angles throughout the entire delivery. Table time was the duration for the treatment table to move to all table locations throughout the entire delivery. kV imaging and processing time was the duration to acquire the kV images throughout the entire delivery, match to DRRs, and perform noise reduction, edge detection, and normalization. Linac time was the beam-on delivery duration. Treatment time was the duration from initial auto-alignment to the end of treatment. Calculated treatment time was the predicted treatment duration by the ZAP-X TPS.
Statistical analysis
Statistical analysis was conducted in Stata 18 (Release 18, StataCorp LLC, College Station, TX) and R version 4.4.1, utilizing mean, standard deviation (SD), median, interquartile range (IQR), range, and linear regression. Correlations among the various dosimetric parameters and indices were examined using Pearson correlation coefficients r and 95% confidence interval (95% CI) using Fisher’s transforms. Variables were considered correlated if |r| > √0.6 and 95%CI > 0. Two-sample t-test with Welch correction was performed for mask comfort comparison. Two-sample Wilcoxon rank-sum (Mann-Whitney) test was performed for the mask number of readjustments, setup time, and offset comparisons. Statistical significance was defined as p<0.05. ZAP-X treatment time was modeled using multivariate linear regression to determine variable importance. Clinical outcome was assessed using Kaplan-Meier survival analysis.
Results
A total of 200 patients were treated with ZAP-X SRS from October 2023 to January 2025, consisting of 374 targets. Patient pathology demographics consisted of 106 brain metastases (BM), 42 meningiomas (MA), 18 trigeminal neuralgias (TN), 11 acoustic neuromas (AN), nine recurrent glioblastomas (RGBM), seven pituitary adenomas (PA), three spinal tumors (ST), three arteriovenous malformations (AVM), and one cavernous hemangioma of the pons (HM). The average number of patients treated per month was 13 ± 2, and the average number of treatments per month was 35 ± 9.
The maximum number of patients treated in a day was five. Self-reported physicist treatment planning time was as follows: TN: ≤5 minutes, single target spherical: ≤30 minutes, multiple targets spherical: ≤1 hour, irregular single target or multiple targets = minutes - three days, PSQA = hours. From October 2023 to January 2025, five patients were postponed due to machine issues, with no cancellations. All QA tests and measurements were within the recommended tolerances. The average Winston-Lutz x-offset was 0.04 ± 0.13 mm (range: -0.32 - 0.36 mm), the average y-offset was 0.38 ± 0.09 mm (range: -0.15 - 0.58 mm), and the average z-offset was 0.1 ± 0.1 mm (range: -0.13 - 0.66 mm). The average PSQA gamma passing rate was 98.5 ± 1.7% (range: 91.2 - 100%) at a 10% low-dose threshold, 2% dose difference, and 1 mm distance-to-agreement.
Dosimetric evaluation
Various dosimetric variables for each pathology are presented in Table 2. The average delivered doses were 23 ± 4 Gy for BM, 23 ± 4 Gy for MA, 83 ± 5 Gy for TN, 21 ± 5 Gy for AN, 30 Gy for RGBM, 26 ± 3 Gy for PA, 34 ± 6 Gy for AVM, 28 ± 3 Gy for ST, and 25 Gy for HM. The largest tumor volume treated was 29.29 cm³, and the maximum number of targets treated in a single course was 10. Regarding plan quality, the average indices were as follows: CI: 1.3 ± 0.3, PCI: 0.77 ± 0.11, GI: 3.3 ± 0.8, HI: 1.5 ± 0.3, and GM: 0.38 ± 0.16. Mean target prescription dose coverage was 98 ± 2%. Strong correlations were found between the following dosimetric variables: monitor units and Linac time (r = 0.995, 95%CI = 0.994 - 0.996), GM and target volume (r = 0.888, 95% CI = 0.864 - 0.908), treatment time and setup time (r = 0.880, 95% CI = 0.860 - 0.898), number of beams and calculated treatment time (r = 0.870, 95% CI = 0.848 - 0.889), HI and prescription isodose line (r = -0.846, 95% CI = -0.873 - -0.814), dose and number of fractions (r = 0.832, 95% CI = 0.804 - 0.856), number of isocenters and calculated treatment time (r = 0.816, 95% CI = 0.786 - 0.842), CI and PCI (r = -0.814, 95% CI = -0.846 - -0.777), total collimator size and number of isocenters (r = 0.813, 95% CI = 0.783 - 0.839), treatment time and gantry time (r = 0.800, 95% CI = 0.768 - 0.828), and total path number and number of isocenters (r = 0.783, 95% CI = 0.748 - 0.813).
Mask evaluation
Mask parameter results for the Fibreplast and Nanor head mask, and the Efficast head and shoulder mask, are shown in Table 3. The shim mask significantly reduced y-offset (p = 0.0014), pitch-offset (p<0.001), roll-offset (p<0.001), yaw-offset (p<0.001), number of readjustments (p = 0.0294), and setup time (p = 0.0017). There was no significant difference in x-offset (p = 0.406) and z-offset (p = 0.453). Mask comfort improved significantly (p = 0.0345).
Table 3: Mask parameter results for Fibreplast and Nanor head mask and Efficast head and shoulder mask†Median (IQR: p25, p75). ‡P<0.05 indicates statistical significanceTwo-sample t-test with Welch correction was performed for mask comfort comparison. Two-sample Wilcoxon rank-sum (Mann-Whitney) test was performed for readjustments, setup time, and offset comparisonsSD: standard deviation; IQR: interquartile range
Patient satisfaction
100 patients responded to the postoperative satisfaction survey. The average patient ratings were as follows: ease of scheduling: 4.9 ± 0.3, staff helpfulness: 4.98 ± 0.13, ZAP-X cleanliness: 4.97 ± 0.18, staff friendliness/courtesy: 4.98 ± 0.13, physician procedure explanation: 4.9 ± 0.3, waiting area comfort: 4.9 ± 0.3, simulation comfort: 4.7 ± 0.6, mask creation comfort: 4.6 ± 0.6, MRI comfort: 4.7 ± 0.6, treatment comfort: 4.4 ± 0.9, post-treatment comfort: 4.7 ± 0.5, response to concerns/complaints: 4.9 ± 0.3, overall rating of care: 4.97 ± 0.18, care coordination: 5.0 ± 0.2, and recommending JSUMC: 4.98 ± 0.13.
ZAP-X treatment time
ZAP-X treatment time variables are presented in Table 4. The average treatment time was 50 ± 20 minutes, calculated treatment time 40 ± 10 minutes, setup time 11 ± 12 minutes, gantry time 30 ± 10 minutes, table time 0.8 ± 0.5 minutes, kV imaging and processing time 8 ± 4 minutes, and Linac time 6 ± 3 minutes. Average treatment time and calculated treatment time plotted over months are shown in Figure 3A. The treatment time appears oscillatory in nature, increasing and decreasing periodically as the months increase. Calculated treatment time appears higher in the first month and levels out in the second month. The higher calculated treatment time in the beginning may be due to a learning curve in treatment planning, supported by plotting over months the number of isocenters (slope = -0.221, p = 0.008), total path number (slope = -2.657, p = 0.009), and total collimator size (slope = -2.346, p<0.001), as shown in Figures 3B-3D.
(A) Treatment time, (B) number of isocenters, (C) total path number, and (D) total collimator size over monthsThe treatment time appears oscillatory in nature, increasing and decreasing periodically as the months increase. Calculated treatment time appears higher in the first month and levels out in the second month. The higher calculated treatment time in the beginning may be due to a learning curve in treatment planning
The number of isocenters, total path number, and total collimator size used by the physicist treatment planners decreased significantly over time. To assess the accuracy of the ZAP-X TPS calculated treatment time, linear regression was performed against treatment time, producing an adjusted r^2^ of 0.640 with a root mean square error (RMSE) of 11.115, as shown in Figure 4A. The ZAP-X TPS model’s predictions for treatment time deviate on average by 11 minutes from the actual treatment durations. For the multivariate model of treatment time, three multivariate models were analyzed. The model utilizing setup time, gantry time, kV imaging and processing time, number of targets, number of isocenters, and prescription isodose line had residuals that were the most normally distributed. Additionally, the model achieved an adjusted r² of 0.972, indicating that it captures almost all variability in treatment time, and with an RMSE of 3.005, the model’s predictions on average deviate by three minutes from the actual treatment durations. The regression plot for the multivariate model is shown in Figure 4B. In this model, all predictors were statistically significant. The model revealed that setup time was the most important predictor of treatment duration, followed by gantry time and kV imaging and processing time. The model also demonstrated that the number of targets, the prescription isodose line, and the number of isocenters significantly impacted treatment time. The variable importance graph for the multivariate model is shown in Figure 4C.
(A) Treatment time vs. calculated treatment time. (B) A multivariate linear regression was conducted with six variables: setup time, gantry time, kV imaging and processing time, number of targets, prescription isodose line, and number of isocenters. (C) Variable importance graph: setup time had the greatest effect on treatment durationRMSE: root mean square error
Treatment side effects
Treatment side effects observed after ZAP-X SRS were fatigue (62.5%), headache (35.5%), gait disturbance (23.5%), hypersomnia (20%), alopecia (19%), dizziness (18.5%), radiation dermatitis (16%), nausea (7%), tinnitus (0.5%), and visual disturbance (0.5%) (Figure 5). The two most common side effects observed were fatigue and headache. Most side effects were mild or moderate and self-limited, resolving approximately within two weeks after treatment. Overall, 28.5% of patients reported no side effects.
ZAP-X SRS treatment side effectsSRS: stereotactic radiosurgery
Clinical outcomes
For 40 BM patients consisting of 122 targets, the median follow-up was four months (IQR: p25 = 3, p75 = 8 months). Follow-up was scheduled at one month post-treatment, followed by three-month intervals, which consisted of the neurosurgeon's and radiation oncologist's direct evaluation and follow-up MRI. Complete response was defined as no visible target lesion, partial response ≥30% decrease in longest distance, stable <30% decrease in longest distance, and progressive disease ≥20% or 2.5 mm increase in longest distance [25-26]. Of note, 75 targets (61.5%) were classified as complete response, 30 (24.6%) as partial response, 15 (12.3%) as stable, and two (1.6%) as progressive disease. The Kaplan-Meier local tumor control was 97% at 12 months and 89% at 16 months. The BM Kaplan-Meier local tumor control curve is shown in Figure 6.
BM Kaplan-Meier tumor control curve for 40 patients (122 targets)The Kaplan-Meier local tumor control was 97% at 12 months and 89% at 16 monthsBM: brain metastases; SRS: stereotactic radiosurgery
For 16 TN patients, the median follow-up was 7.5 months (IQR: 5, 12 months). Follow-up was scheduled at one month post-treatment, followed by three-month intervals, which consisted of the neurosurgeon's and radiation oncologist's direct evaluation, Modified Barrow Neurological Institute (BNI) pain scale classification [27], and follow-up MRI. A positive outcome was defined as achieving a BNI score lower than the presentation value, while recurrence was defined as an increase in the BNI score relative to the last follow-up assessment. Follow-up BNI was provided for 16 patients at one month, 14 patients at three months, 12 patients at six months, eight patients at nine months, and eight patients at 12 months. One-, three-, and six-month follow-ups demonstrated positive patient outcomes, with all patients experiencing decreased pain intensity and relief at one month. Three patients had a complete response to treatment (BNI = I, no pain, no medication): one patient at three months, two patients at nine months. The average BNI before SRS was 4.4 ± 0.5 for 16 patients, and the average BNI 12 months after SRS was 2 ± 1 for eight patients (Figure 7A). The Kaplan-Meier recurrence-free survival was 75% at 12 months (25% rate). At nine and 12 months, two patients experienced pain recurrence. The TN Kaplan-Meier recurrence-free survival curve is shown in Figure 7B.
(A) Average BNI versus time after ZAP-X TN SRS. (B) TN Kaplan-Meier recurrence-free survival curve for 16 patientsThe recurrence-free survival was 75% at 12 months (25% recurrence rate)BNI: Barrow Neurological Institute pain scale classification; SRS: stereotactic radiosurgery
Discussion
The purpose of this study was to evaluate the clinical performance and initial implementation outcomes of the ZAP-X SRS system through a prospective analysis of the first 200 patients treated at JSUMC. As one of the earliest and most comprehensive clinical experiences with this novel gyroscopic, self-shielded SRS platform, this study aimed to assess treatment efficiency, patient satisfaction, and technical accuracy across a wide spectrum of central nervous system pathologies. The findings demonstrate that the ZAP-X system offers high dosimetric precision, treatment capability, and patient satisfaction, supporting its role as a viable and effective alternative to traditional SRS systems such as GK and CK. This work provides important real-world validation of the system's potential in clinical settings and lays the groundwork for further exploration and expansion of its applications.
Dosimetric indices and performance
The plan quality indices calculated in this study are similar to those reported in the literature for ZAP-X. In the first large prospective study involving the ZAP-X platform, Ehret et al. reported an average CI of 1.26 ± 0.20, PCI of 0.78 ± 0.16, GI of 3.20 ± 0.44, and HI of 1.69 ± 0.24 across 100 patients [5]. Hendricks et al. reported an average CI of 1.54 ± 0.47 across 59 patients for ZAP-X SRS [6]. Muacevic et al. reported an average PCI of 0.79, GI of 3.04, and HI of 1.89 across 41 patients for ZAP-X SRS [7]. Conroy et al. reported an average CI of 1.43 (range: 1.21 - 1.86), GI of 3.16 (2.49 - 4.88), and HI of 1.52 (1.14 - 2.00) [8]. Paddick et al. reported an average PCI of 0.830 and GI of 2.74 for benign lesions and an average PCI of 0.700 and GI of 3.83 for metastases across seven patients [28].
Patient satisfaction
One hundred patients responded to the post-treatment questionnaire. Most patients rated their ease of scheduling highly. Staff and facility ratings were high, and patients reported a high degree of satisfaction with both staff helpfulness and facility cleanliness. Physician communication was also rated highly. Patients provided mixed feedback regarding comfort during preoperative MRI and the ZAP-X treatment itself, with some patients mentioning that the thermoplastic mask was uncomfortable. Overall, satisfaction was high, and several patients left positive comments regarding the coordination of the care team. Nearly all respondents indicated that they would recommend JSUMC’s Radiation Oncology suite to others. These results demonstrate a high level of patient satisfaction with their ZAP-X experience.
Treatment time
Treatment times for ZAP-X SRS show considerable variation in the existing literature. Ehret et al. reported an average treatment time of 47 ± 30.6 minutes and an average setup time of 9.7 ± 10.0 minutes for ZAP-X SRS [5]. Hendricks et al. reported an average treatment time of 66.1 ± 36.2 minutes [6]. Muacevic et al. reported a median treatment time of 30 minutes (IQR: p25 = 26, p75 = 34 minutes) [7]. Conroy et al. reported a median treatment time of 24 minutes per lesion (range: 9-123 minutes) [8]. Gevaert et al. and Han et al. documented average treatment times of 68.1 ± 27.5 minutes for GK, 28.4 ± 8.1 minutes for CK, 16.8 ± 2.2 minutes for Novalis-Tx DCA, 21.7 ± 3.4 minutes for Novalis-Tx DMLC-IMRT, and 42 ± 16 minutes for Helical Tomotherapy [29-30]. Reducing setup time could be achieved by streamlining patient alignment, partly through the use of the Efficast head and shoulder mask with two shims. The vendor has indicated that a gyroscopic correction update for the ZAP-X system will be implemented, which may further help decrease setup time.
The gyroscopic correction will use the gantry to make automatic corrections for rotational offsets (pitch, roll, and yaw) to enhance precision upon patient misalignment. The second greatest factor contributing to the treatment time was the gantry time. Currently, the ZAP-X utilizes static beams. Switching to arc-based delivery is expected to significantly reduce gantry time. According to the vendor, this upgrade is planned for implementation in the near future. The constraint for the calculated treatment time of a ZAP-X SRS plan at JSUMC is generally ≤60 minutes. To help reduce ZAP-X treatment time, the treatment planner can utilize larger collimator sizes. In our clinic, we have observed cases where two equivalent plans for the same patient (one using larger collimators and one using smaller) show that the plan with larger collimators achieves a substantially shorter treatment time, as illustrated in Figures 8A-8B. However, planners must be mindful that larger field sizes may not always be feasible for highly irregularly shaped targets, as demonstrated in Figure 8C.
Equivalent plans on a patient where (A) one utilizes smaller collimator sizes and (B) one utilizes larger, where the larger plan has a significantly shorter treatment time. (C) Utilizing larger field sizes may not always be achievable with highly irregular shaped targets
Clinical outcomes
The clinical results in this study for BM and TN ZAP-X SRS are in line with those reported in the literature for SRS. In a pooled analysis of manuscripts evaluating tumor control probability for BM SRS, Redmond et al. reported that for tumors ≤20 mm, single-fraction doses of 18 and 24 Gy corresponded with >85% and 95% one-year local control rates, respectively. For tumors of 21-30 mm, an 18 Gy single-fraction dose was associated with 75% local control. For tumors of 31-40 mm, a 15 Gy single-fraction dose yielded ~69% local control. For three- to five-fraction SRS using total doses ranging from 27 to 35 Gy, one-year local control of 80% has been reported for tumors 21-40 mm in diameter. [31]. In a systematic review of TN SRS, Tuleasca et al. reported a median recurrence rate of 23% for GK, 27.2% for CK, and 29% for Linac-based [32].
Mixed fractionation optimization
To reduce ZAP-X treatment planning time for mixed fraction schemes, a method was developed utilizing one optimization run for multiple targets [33]. To accommodate mixed fractionation schemes for ZAP-X SRS, targets are first optimized in a single plan (Plan_A) using a single fractionation to their prescribed doses. After optimization, isocenters with new beams/MUs on them are split into groups with their associated targets to make individual plans (Plan_A_PTV1, Plan_A_PTV2, etc.) with proper fractionation. Each plan is then only re-prescribed to any isodose level to scale the dose to achieve 99% coverage on the respective targets. After individual plans achieve 99% dose coverage, plan sums for individual plans are compared on clinical objectives using Timmerman dose constraints. A study reporting and analyzing this ZAP-X mixed fraction optimization method is planned for a separate report.
Patient clearance
When planning the treatment, the dimensions of the ZAP-X relative to the patient must be considered and checked regarding larger-sized patients or patients who require accommodations during treatment. The table to shell entrance height is 45.72 cm, the shell entrance width is 81.28 cm, the table railing width is 50.8 cm, the treatment range from table to nose is 27 cm, and the table weight limit currently is 460 lbs. At JSUMC, the largest patient treated with ZAP-X SRS weighed 300 lbs (Figure 9). One patient required elevation using mold care due to difficulty breathing while lying flat.
(A) Largest patient treated with ZAP-X SRS at JSUMC (weighing 300 lbs). (B) Patient requiring elevation with mold care due to difficulty breathing while lying down flat on the treatment tableJSUMC: Jersey Shore University Medical Center
Limitations
As this study was conducted at a single center, the findings may have limited generalizability. Outcomes could differ at other institutions with different personnel or patient populations and varying proportions of pathologies. In the future, we hope our data can contribute to a larger, multi-institutional study on ZAP-X technology. Patient satisfaction and mask evaluations may be subject to selection bias. Additionally, because the technology was recently implemented at JSUMC, follow-up time was limited. Future analyses will aim to evaluate prospective outcomes related to tumor control, symptomatic improvement, and other patient care metrics following SRS. Further studies will also include a control group, such as GK, CK, or Linac-based systems, to directly compare the efficacy of ZAP-X with other widely used SRS modalities. The results presented in this study pertain to system version DP-1010.
Conclusions
Our experience utilizing the ZAP-X radiosurgery platform has been extremely positive. Since its implementation at JSUMC, treatment of both benign and malignant lesions alike has been effective and without complications. Across the board, our Neurosurgery and Radiation Oncology Departments effectively synergized to deliver a streamlined treatment planning workflow, which contributed to excellent patient satisfaction. We look forward to exploring future directions with this novel radiotherapy option and expanding the scope of its utilization to other pathologies of the central nervous system and beyond. As the body of literature on ZAP-X continues to grow, we anticipate that its benefits will draw wider adoption by physicians worldwide. In this context, our findings can help guide the refinement and optimization of the ZAP-X system for a broad range of clinical indications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Characterization of a novel 3 megavolt linear accelerator for dedicated intracranial stereotactic radiosurgery Cureus Weidlich GA Bodduluri M Achkire Y Lee C Adler JR Jr 011201910.7759/cureus.4275 PMC 653823531183264 · doi ↗ · pubmed ↗
- 2Self-shielding for the ZAP-X: revised characterization and evaluation Cureus Weidlich GA Schneider MB Simcic V Oostman Z Adler JR Jr 013202110.7759/cureus.13660 PMC 801725633824811 · doi ↗ · pubmed ↗
- 3Machine performance and stability of the first clinical self-shielded stereotactic radiosurgery system: Initial 2-year experience J Appl Clin Med Phys Srivastava SP Sorensen SP Jani SS Yan X Pinnaduwage DS 024202310.1002/acm 2.13857 PMC 1001867336519493 · doi ↗ · pubmed ↗
- 4Profile comparisons of small dose volumes between three radiosurgery systems Cureus Sorensen SP Pinnaduwage D Srivastava S 161842019 https://www.cureus.com/abstracts/388-profile-comparisons-of-small-dose-volumes-between-three-radiosurgery-systems
- 5Self-shielding gyroscopic radiosurgery: a prospective experience and analysis of the first 100 patients Cureus Ehret F Kohlhase N Eftimova D 016202410.7759/cureus.56035 PMC 1100869838606262 · doi ↗ · pubmed ↗
- 6ZAP-X gyroscopic radiosurgery system: A preliminary analysis of clinical applications within a retrospective case series Stereotact Funct Neurosurg Hendricks BK Di Domenico JD Barani IJ Barranco FD 9910710020223494262910.1159/000519862 · doi ↗ · pubmed ↗
- 7Self-shielding gyroscopic radiosurgery—a first clinical experience, case series, and dosimetric comparison World Neurosurg Muacevic A Eder MM Hofmann T Fürweger C Ehret F 06164202210.1016/j.wneu.2022.04.12035568128 · doi ↗ · pubmed ↗
- 8Gyroscopic stereotactic radiosurgery: a retrospective analysis Cureus Conroy DR Woody SM Niu YE 017202510.7759/cureus.88553 PMC 1237038340851739 · doi ↗ · pubmed ↗