Dose-Summation–Guided Re-irradiation Planning for Brain Metastases: Cross-Platform Verification Between Brainlab Elements and GammaPlan
Shigeo Matsunaga, Takashi Shuto, Jo Sasame

TL;DR
This paper presents a method to safely plan repeated brain cancer radiation treatments by tracking cumulative doses across different systems.
Contribution
A cross-platform workflow for cumulative-dose-aware re-irradiation planning in brain metastases is introduced and verified.
Findings
A verification case showed that non-target dose summation could prevent radiation necrosis.
Prospective dose summation maintained target coverage while reducing unintended dose to prior treatment areas.
The cross-platform approach is feasible for balancing efficacy and safety in repeat brain radiosurgery.
Abstract
We report a practical, cross-platform workflow for cumulative-dose-aware re-irradiation in brain metastases. Before RT-DOSE is imported across planning systems (Brainlab Elements and/or GammaPlan), previously irradiated foci are treated prospectively as organs-at-risk during optimization, and the summed dose is visualized to avoid hotspots while preserving coverage. In a verification case planned without dose summation, a non-target previously irradiated focus ultimately developed radiation necrosis; post-hoc summation showed that explicit constraints could have reduced cumulative exposure. In a second case prospectively planned with summation, target coverage was maintained while decreasing the unintended dose to a non-target previously treated focus, with subsequent control and no new toxicity. This cross-platform approach is feasible and clinically actionable for balancing efficacy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
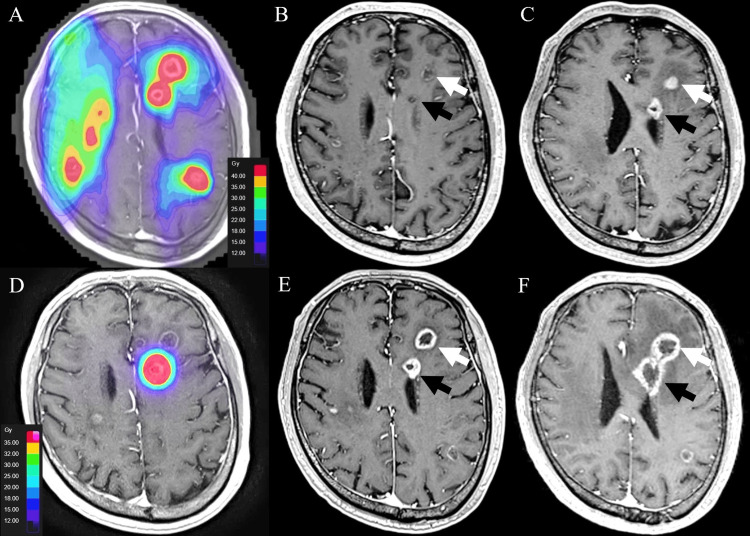 Figure 1
Figure 1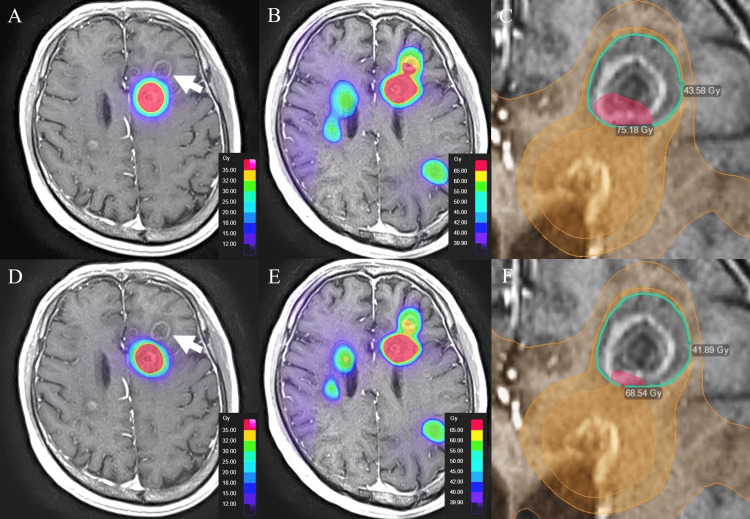 Figure 2
Figure 2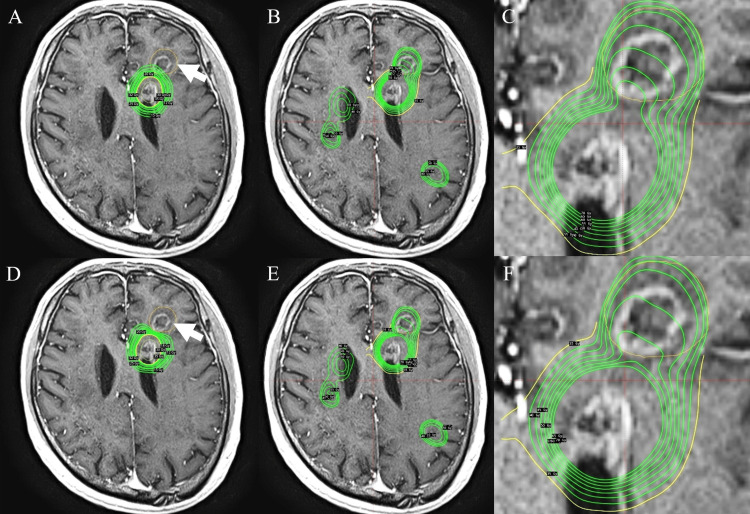 Figure 3
Figure 3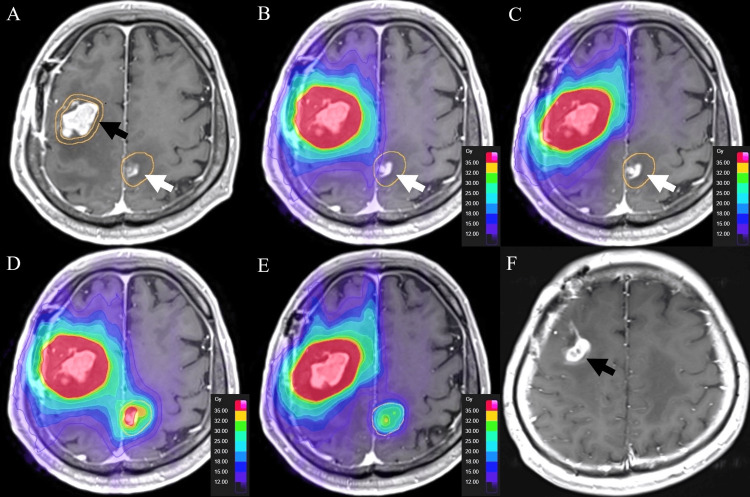 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Brain Metastases and Treatment · Radiation Therapy and Dosimetry
Introduction
As survival has improved with modern systemic therapies and advanced imaging detects ever smaller intracranial lesions, the incidence of brain metastases continues to rise [1,2]. Consequently, repeated stereotactic radiosurgery (SRS) for new or recurrent brain metastases has become common in clinical practice [3,4]. Large multi-institutional and large-cohort data, including the JLGK0901 trial and companion series, demonstrate that SRS alone is safe and effective for patients harboring multiple brain metastases, even when five or more (and up to ≥10) lesions are treated [5-8]. Randomized evidence suggests that, for patients with one to three metastases, SRS alone limits cognitive deterioration compared with whole-brain radiotherapy without compromising overall survival, underscoring the value of focal approaches [3,9]. However, when a new target abuts a previously irradiated focus, ignoring historical dose risks, unrecognized hotspots, and iatrogenic injury. We implemented a cross-platform strategy that (i) imports prior RT-DOSE, (ii) sums dose across courses and platforms, and (iii) prospectively treats previously irradiated foci as organs-at-risk (OARs) during optimization; this design was informed by accumulating evidence that cumulative dose to the brain and critical structures, including overlap volumes across radiation courses, predicts toxicity and guides safe re-irradiation in intracranial tumors [10-15], that normal-brain dose-volume metrics (e.g., V12) correlate with symptomatic radionecrosis [16,17], and that RTOG 90-05 single-fraction dose-escalation limits provide practical guardrails for retreatment [8,18-20]. We then verified its clinical implications in two representative cases.
Technical report
Platforms and imaging
Planning was performed with Brainlab Elements (v4.0; Brainlab, Munich) and GammaPlan (v11.4.2; Elekta, Stockholm). Datasets included non-contrast CT and contrast-enhanced T1-weighted MRI (1-mm slices) plus T2-weighted MRI (2-mm, no gap).
Cross-platform transfer and dose summation
Prior RT-DOSE (DICOM RT) was transferred between systems, rigidly co-registered to the current dataset, and visualized as cumulative isodose volumes. When summation was not natively available, RT-DOSE from the other platform was imported for verification.
Immobilization and delivery
Gamma Knife SRS used the Leksell Gamma Knife Icon (frame or mask). LINAC-based SRS used TrueBeam STx/Novalis with thermoplastic mask immobilization and multiple dynamic conformal arcs (typical prescription ~70% isodose), with fractionation individualized.
Planning strategy (previous foci treated as OARs)
Planning was performed with prior RT-DOSE imported and rigidly co-registered to the current dataset. Previously irradiated foci were contoured and treated as OARs during optimization. For each re-irradiation, we generated and compared two plans: (1) an unconstrained plan that did not apply limits to the prior foci, and (2) a summation-guided plan that prospectively constrained the prior foci while maintaining planning target volume (PTV) coverage. Plan optimization prioritized target coverage and conformity while explicitly minimizing the cumulative dose to previously irradiated foci based on the summed (initial + re-irradiation) dose distribution [4,10]. In practice, we targeted cumulative Dmax ≤ ~65-70 Gy and cumulative Dmean ≤ ~55-60 Gy to the prior focus when feasible and monitored normal-brain V12_cum alongside standard target metrics (e.g., PTV coverage/D95) and isodose line (IDL) selection (typically ~70%). These values were used as planning guardrails rather than absolute cutoffs, informed by single-fraction dose-escalation limits (RTOG 90-05) and by reports linking normal-brain V12 to symptomatic radionecrosis after SRS [16-18] (with contemporary data in modern systemic therapy settings) [10]. Cumulative maxima/means within prior foci and PTV coverage were recorded for both plans, and the final plan was selected to preserve target coverage while reducing exposure to previously irradiated non-target foci.
Case presentation
Case 1: Delivered Without Dose Summation and Verification Added Later
A man in his 60s with ALK-rearranged lung adenocarcinoma presented with left hemiparesis. Twelve metastases were treated using Brainlab Elements Multiple Brain Mets SRS (40 Gy/10 fx to the 70% isodose; eight arcs) (Figure 1A).
Case 1 (delivered without dose summation)(A) Initial Brainlab Elements plan (Multiple Brain Mets SRS): 40 Gy in 10 fractions prescribed to the 70% isodose, with the composite RT-dose distribution superimposed on the baseline contrast-enhanced T1-weighted MR image (the underlying tumor margins remain faintly visible). (B, C) Baseline contrast-enhanced T1-weighted MR images without RT-dose overlay demonstrating the left frontal index metastasis (white arrow) and an adjacent previously irradiated focus (black arrow); panel B (four-month follow-up) shows partial regression and panel C (eight-month follow-up) shows subsequent regrowth of the index lesion. (D) Brainlab Elements re-irradiation: 35 Gy in five fractions. (E) Early (three-month) post–re-irradiation follow-up demonstrating a subtle decrease in lesion size with thinning of the enhancing rim and enlargement of the central low-signal area (white arrow), with minimal change in the adjacent previously treated focus (black arrow). (F) Six-month follow-up showing enlargement of both the re-irradiated target and the adjacent previously treated, non-target left frontal focus (white and black arrows), findings consistent with radiation necrosis.
Lesions regressed at four months (Figure 1B). At eight months, a left frontal lesion regrew (Figure 1C) and was re-irradiated (35 Gy/5 fx; six arcs) as the sole target (Figure 1D); the adjacent previously treated left frontal focus-non-target at re-irradiation-later enlarged, consistent with radiation necrosis (RN) (Figures 1E, 1F).
Brainlab Elements verification: Plan 1 (no constraint to the non-target left frontal focus) followed by dose summation yielded cumulative max 75.18 Gy and mean 58.64 Gy in that focus (Figures 2A-2C).
Case 1 verification in Brainlab Elements using dose summation(A) Plan 1 without constraints to the non-target left frontal focus (white arrow). (B) Summed dose for the initial and re-irradiation plans. (C) Cumulative metrics within the non-target focus for Plan 1 (max 75.18 Gy; mean 58.64 Gy). (D) Plan 2 with constraints to the non-target focus. (E) Summed dose for Plan 2. (F) Cumulative metrics within the non-target focus for Plan 2 (max 68.54 Gy; mean 56.23 Gy).
Plan 2 (explicit constraints to that focus) reduced the cumulative exposure to max 68.54 Gy and mean 56.23 Gy (Figures 2D-2F).
GammaPlan verification: Importing the initial Elements RT-DOSE, Plan 3 (no constraint) yielded cumulative max 75.4 Gy and mean 57.9 Gy (Figures 3A-3C); Plan 4 (with constraints) reduced to max 67.1 Gy and mean 55.9 Gy (Figures 3D-3F).
Case 1 verification in GammaPlan using dose summation(A) Plan 3 without constraints to the non-target left frontal focus (white arrow). (B) Summed dose for the initial and re-irradiation plans. (C) Cumulative metrics within the non-target focus for Plan 3 (max 75.4 Gy; mean 57.9 Gy). (D) Plan 4 with constraints to the non-target focus. (E) Summed dose for Plan 4. (F) Cumulative metrics within the non-target focus for Plan 4 (max 67.1 Gy; mean 55.9 Gy).
Although platform-specific differences were small, both showed consistent reductions with summation-guided constraints. Had Plan 2 (Brainlab Elements verification) (Figure 2D-F)/Plan 4 (GammaPlan verification) (Figure 3D-F) been delivered clinically, complete prevention of radionecrosis cannot be guaranteed, but severity might have been mitigated.
Case 2: Planned and Delivered With Dose Summation
A man in his 50s with gastroesophageal junction cancer developed multiple brain metastases, including a right frontal lesion requiring surgery and 14 additional small lesions treated with Gamma Knife SRS (single fraction 20 Gy to 51-90% IDL). The right frontal cavity recurred (Figure 4A).
Case 2 (planned and delivered with dose summation)(A) Recurrence at the right frontal postoperative cavity (black arrow). (B) Brainlab Elements Plan 1 without constraints to the previously treated left parietal focus (white arrow). (C) Plan 2 with explicit constraints to that non-target focus. (D and E) Summed dose distributions for Plans 1 and 2. (F) Six-month decrease of the right frontal target with near-resolution and continued control of the previously treated left parietal focus.
Re-irradiation was planned in Elements (10 arcs; 35 Gy/5 fx at 70% IDL). Prior GammaPlan RT-DOSE was imported. Plan 1 (no constraint to a non-target left parietal focus previously treated by GK) yielded higher non-target dose on summation (Figure 4B), whereas Plan 2 with explicit constraints reduced the non-target exposure while maintaining PTV coverage (Figure 4C). The summed dose distributions, combining the initial GammaPlan RT-DOSE with the re-irradiation RT-DOSE from Elements, for Plan 1 and Plan 2 are shown in Figure 4D and Figure 4E, respectively. At six months, the right frontal target decreased and the previously treated left parietal focus nearly disappeared while remaining controlled (Figure 4F).
Discussion
Summation-guided planning operationalizes a simple principle: visualize the true cumulative dose and treat previously irradiated foci as OARs while protecting the current target. Without summation, imposing constraints based on geometric surrogates (e.g., prior GTV/PTV shells) can distort both peripheral and internal high-dose regions and may compromise coverage. Summation makes these trade-offs explicit, enabling an informed choice between constrained and unconstrained solutions.
In our experience, Case 1 was re-irradiated in routine practice without dose summation, and the adjacent, previously irradiated non-target focus ultimately developed RN. In contrast, verification performed in both Brainlab Elements and GammaPlan demonstrated that when the previously treated non-target focus was prospectively constrained as an OAR, the cumulative dose (max/mean) to that focus was consistently reduced across platforms. In Case 2, summation was used prospectively during planning, which maintained PTV coverage while lowering exposure to the non-target previously irradiated focus.
Summation-guided planning primarily advances how retreatment decisions are made: cumulative dose is rendered explicit, previously treated foci are constrained like OARs, and target coverage is maintained with fewer unexpected effects on adjacent high-dose regions, an approach that is consistent with emerging data on the clinical relevance of cumulative-dose evaluation in repeat intracranial irradiation [9,10] and with reports linking normal-brain dose-volume metrics such as V12 to symptomatic radionecrosis after SRS [11,16] (including contemporary series evaluating V12 and adverse radiation effects in modern systemic therapy contexts [19]). Beyond V12, prior studies have explored additional dose, volume or biologically adjusted metrics, V10-V14 and Dmax [16,17], as well as BED/EQD2 and V12_eq [10,11], as correlates of symptomatic radionecrosis. Taken together with the single-fraction limits from RTOG 90-05 and the association between normal-brain V12 and adverse radiation effects, these cumulative constraints serve as planning guardrails rather than absolute cutoffs, helping balance target coverage against injury risk during retreatment. Our two cases, verified across Brainlab Elements and GammaPlan, illustrate cross-platform, consistent reductions in exposure to non-target prior foci when summation-based constraints are applied, while preserving PTV coverage. In day-to-day practice, conventional single-fraction dose-escalation limits (RTOG 90-05) can serve as pragmatic guardrails within this workflow [18].
Given the retrospective design and the inclusion of only two patients, no definitive conclusions regarding safety or clinical efficacy can be drawn from this report. Rather, our aim is to illustrate a technically simple, readily adoptable workflow for repeat intracranial SRS near previously high-dose regions and to highlight how it can be implemented in daily practice. Future work, ideally in prospective, multi-institutional cohorts, is needed to validate whether such summation-guided planning actually improves toxicity and tumor control outcomes and to explore thresholding strategies (e.g., V12-derived or EQD2/BED-based limits) that can be operationalized within planning systems.
Conclusions
Summation-guided re-irradiation primarily advances how retreatment decisions are made: cumulative dose is rendered explicit, previously treated foci are prospectively constrained as OARs, and target coverage is preserved while minimizing unexpected dose escalation in adjacent high-dose regions. In our two cases, cross-platform verification in Brainlab Elements and GammaPlan showed consistent reductions in exposure to non-target prior foci when summation-based constraints were applied, without compromising PTV coverage. Given its technical feasibility and clinical clarity, we recommend incorporating cumulative-dose summation as a routine checkpoint for repeat intracranial SRS near prior high-dose areas, while acknowledging that broader prospective validation and operational thresholding (e.g., V12-derived or EQD2/BED-based limits) are warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of brain metastases Curr Oncol Rep Nayak L Lee EQ Wen PY 48541420122201263310.1007/s 11912-011-0203-y · doi ↗ · pubmed ↗
- 2Brain metastases: an update on the multi-disciplinary approach of clinical management Neurochirurgie Mitchell DK Kwon HJ Kubica PA Huff WX O'Regan R Dey M 69856820223386477310.1016/j.neuchi.2021.04.001PMC 8514593 · doi ↗ · pubmed ↗
- 3Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial JAMA Aoyama H Shirato H Tago M 2483249129520061675772010.1001/jama.295.21.2483 · doi ↗ · pubmed ↗
- 4Cumulative doses to brain and other critical structures after multisession Gamma Knife stereotactic radiosurgery for treatment of multiple metastatic tumors Front Oncol Yuan J Lee R Dusenbery KE Lee CK Mathew DC Sperduto PW Watanabe Y 65820182959404510.3389/fonc.2018.00065 PMC 5859351 · doi ↗ · pubmed ↗
- 5Stereotactic radiosurgery for patients with multiple brain metastases (JLGK 0901): a multi-institutional prospective observational study Lancet Oncol Yamamoto M Serizawa T Shuto T 3873951520142462162010.1016/S 1470-2045(14)70061-0 · doi ↗ · pubmed ↗
- 6A multi-institutional prospective observational study of stereotactic radiosurgery for patients with multiple brain metastases (JLGK 0901 study update): irradiation-related complications and long-term maintenance of mini-mental state examination scores Int J Radiat Oncol Biol Phys Yamamoto M Serizawa T Higuchi Y 31409920172881615810.1016/j.ijrobp.2017.04.037 · doi ↗ · pubmed ↗
- 7A case-matched study of stereotactic radiosurgery for patients with multiple brain metastases: comparing treatment results for 1-4 vs ≥ 5 tumors: clinical article J Neurosurg Yamamoto M Kawabe T Sato Y 1258126811820132360093810.3171/2013.3.JNS 121900 · doi ↗ · pubmed ↗
- 8Stereotactic radiosurgery for patients with multiple brain metastases: a case-matched study comparing treatment results for patients with 2-9 versus 10 or more tumors J Neurosurg Yamamoto M Kawabe T Sato Y Higuchi Y Nariai T Watanabe S Kasuya H 1625121 Suppl 20142543493310.3171/2014.8.GKS 141421 · doi ↗ · pubmed ↗