Network-Level Brain Dysfunction Beyond the Lesion: A Rare Case of Monakow Syndrome Presenting With Fluctuating Consciousness and Left Hemispatial Neglect Due to Right Anterior Choroidal Artery Infarction
Godai Yawata, Asato Tsuji, Mariko Takata, Tetsuya Oda, Hirotoshi Hamaguchi

TL;DR
A rare case of brain infarction shows how damage to specific brain hubs can cause widespread dysfunction beyond the lesion site.
Contribution
Demonstrates network-level dysfunction in AChA infarction through functional imaging and clinical presentation.
Findings
Right AChA infarction caused fluctuating consciousness and left hemispatial neglect.
ASL and IMP-SPECT showed extensive hypoperfusion in the right hemisphere beyond structural lesions.
PLIC and LGN act as network hubs, and their injury disrupts global brain efficiency.
Abstract
Anterior choroidal artery (AChA) infarction typically manifests as the classical triad of contralateral hemiparesis, hemisensory loss, and homonymous hemianopia (Monakow syndrome). We report a rare case of right AChA infarction presenting with fluctuating consciousness and left hemispatial neglect, accompanied by widespread functional suppression of the right cerebral hemisphere. A 65-year-old right-handed man initially exhibited mild dysarthria and left-sided sensory impairment, with no acute lesions on diffusion-weighted MRI. He subsequently developed impaired consciousness and hemispatial neglect. Follow-up MRI demonstrated acute infarcts in the posterior limb of the internal capsule (PLIC) and lateral geniculate nucleus (LGN). Arterial spin labeling (ASL) and N-isopropyl-p-[123I]iodoamphetamine single-photon emission computed tomography (IMP-SPECT) revealed extensive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
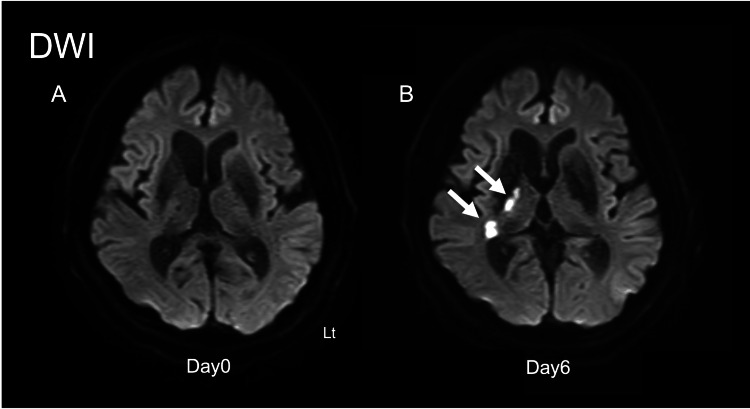 Figure 1
Figure 1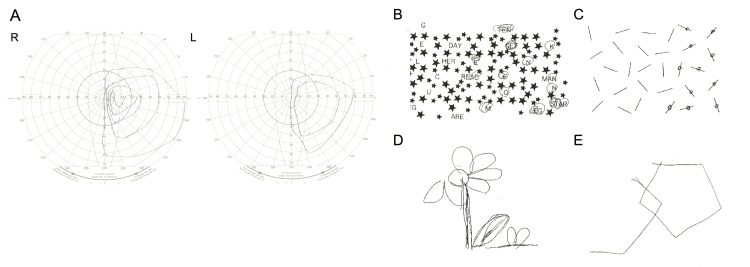 Figure 2
Figure 2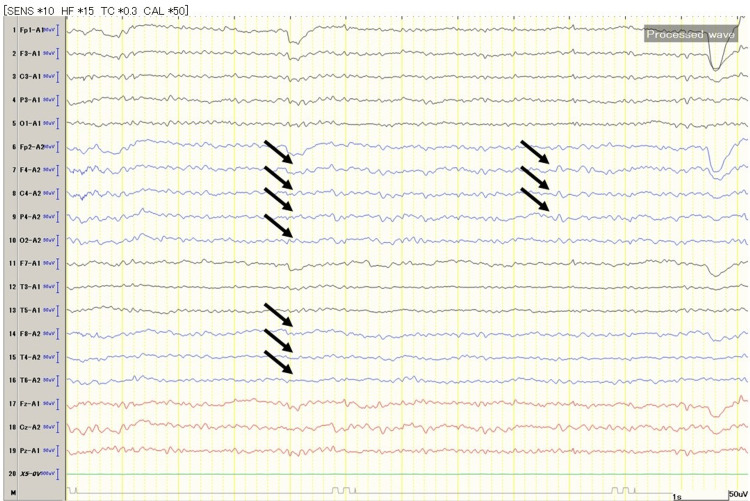 Figure 3
Figure 3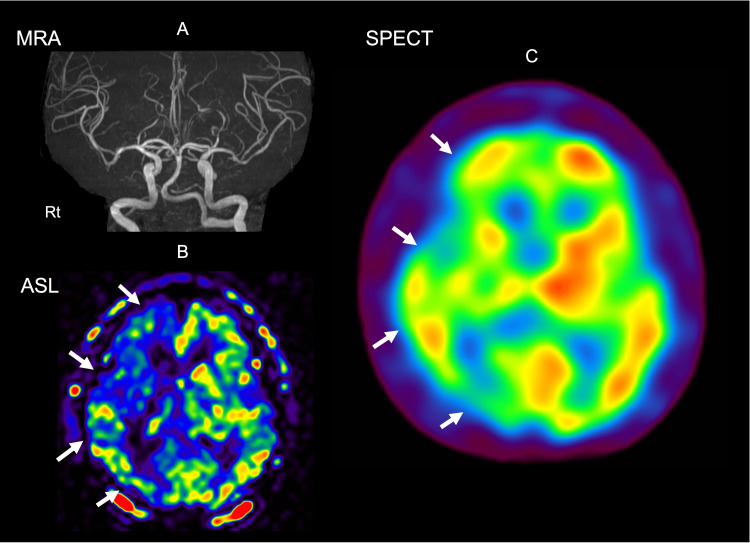 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpatial Neglect and Hemispheric Dysfunction · Hemispheric Asymmetry in Neuroscience · Vestibular and auditory disorders
Introduction
The anterior choroidal artery (AChA), a branch of the internal carotid artery, supplies several strategic deep brain structures, including the posterior limb of the internal capsule (PLIC), lateral geniculate nucleus (LGN), optic radiation, hippocampus, and cerebral peduncle [1]. AChA infarction is uncommon and typically presents with Monakow’s classical triad [2]. However, in the era of connectomics, subcortical lesions are increasingly understood as network-level disturbances rather than isolated focal injuries [3].
The concept of diaschisis, originally introduced by von Monakow, has been revitalized by modern neuroimaging, demonstrating that disruption of critical hubs or white-matter pathways can lead to distant cortical dysfunction [4,5]. The PLIC and LGN are now recognized as integrative hubs connecting motor, sensory, and attentional networks [6]. Injury to these structures may yield higher-order symptoms such as neglect or altered consciousness. We present a rare case of right AChA infarction with fluctuating consciousness and hemispatial neglect, supported by multimodal imaging evidence of widespread right-hemispheric functional suppression.
Case presentation
A 65-year-old right-handed man with untreated hypertension, chronic alcohol consumption, and long-term smoking awoke with left lower-limb weakness and difficulty using a tablet device. On admission, he was alert with stable vital signs (BP: 186/108 mmHg). Neurological examination revealed mild dysarthria, left lower-limb ataxia, and left-sided sensory impairment. Laboratory studies demonstrated impaired glucose tolerance and vitamin B12 deficiency.
Initial MRI showed no diffusion-restricted lesions, and magnetic resonance angiography (MRA) demonstrated no large-vessel stenosis. Hours after admission, he developed fluctuating consciousness (E4V5M6 → E3V3M6) and left visual inattention. On day 1, MRI revealed acute infarcts in the right PLIC and LGN. These became more prominent by day 6, confirming right AChA infarction (Figure 1).
Head MRI imagesDWI: diffusion-weighted imaging; PLIC: posterior limb of the internal capsule; LGN: lateral geniculate nucleus(A) DWI horizontal section on day 0 of onset. (B) DWI horizontal section on day 6 of onset. The white arrows indicate high signal intensity in the right PLIC and LGN, a finding not observed on day 0
No embolic source was identified, and atherothrombotic stroke was suspected. Aspirin (100 mg/day) and argatroban (60 mg/day) were initiated. Goldmann perimetry confirmed left homonymous hemianopia. Neuropsychological testing (star cancellation and line bisection) revealed significant left hemispatial neglect (Figure 2).
Neuropsychological testing(A) Goldman perimetry shows homonymous hemianopia in the left eye. (B) Alphabet deletion test: Only the right half of the alphabet is processed. (C) Line bisection test: Only the right half of the line is processed, showing a tendency for bisection to be biased to the right. (D) Figure copying: The left half of the flower is missing. (E) Pentagon copying: The left half of the pentagon is missing
An electroencephalogram (EEG) showed slowing over the right hemisphere without epileptiform discharges, suggesting functional suppression (Figure 3).
EEG showed slowing over the right hemisphereEEG recorded using the 10-20 system. Recorded using the monopolar recording method. The blue baseline indicates the right hemisphere, the black baseline indicates the right hemisphere. The yellow line represents one second, with a scale bar shown at the bottom right. The black arrows indicate delta wave activity compared to the left hemisphere, suggesting decreased brain function. This activity is occasionally observed in the right hemisphere.
Arterial spin labeling (ASL) perfusion MRI and IMP-SPECT both demonstrated widespread hypoperfusion throughout the right cerebral hemisphere, disproportionate to the small structural infarcts (Figure 4).
ASL perfusion MRI and IMP-SPECTASL: arterial spin labeling; MRA: magnetic resonance angiography; IMP-SPECT: N-isopropyl-p-[123I]iodoamphetamine single-photon emission computed tomography(A-B) Day 6 head MRI images. (A) The left image is an MRA image. (B) ASL image. While there is no difference in blood flow, extensive reduced blood flow is observed in the right cerebral hemisphere. The white arrow indicates the area with reduced blood flow. (C) Brain blood flow scintigraphy SPECT (¹²³I-IMP). Reduced blood flow is observed in the transition zone between the right frontal lobe and parietal lobe, and in the right occipital lobe. Red indicates increased blood flow; blue indicates decreased blood flow. The white arrow indicates the area with reduced blood flow
The patient was transferred for rehabilitation on day 20 with persistent hemianopia, neglect, mild weakness, and sensory deficits.
Discussion
Although AChA infarction is traditionally described by Monakow’s triad, contemporary series emphasize a broader clinical spectrum that reflects the strategic location of its perforators, especially toward the PLIC and the LGN. In particular, collateral supply to the PLIC is limited, so even small lesions can produce disproportionate deficits, while involvement of the LGN yields characteristic visual field syndromes [7,8].
From a systems perspective, both the PLIC and LGN act as network “bottlenecks” that integrate and relay high-throughput information between the cortex and subcortex. White-matter connectomics and white-matter functional studies suggest that the internal capsule, particularly the PLIC, participates in hub-like communication supporting motor, sensory, and attentional functions; thus, local damage can reduce global network efficiency out of proportion to lesion size. Similarly, human imaging demonstrates that the LGN is not a passive relay: its activity is modulated by figure-ground context and spatial attention, positioning it within a broader attentional network [9]. These observations provide a mechanistic bridge between a focal AChA lesion and the higher-order deficits (neglect, fluctuation in arousal).
Multimodal perfusion data in our case (ASL and IMP-SPECT) revealed widespread right-hemispheric hypoperfusion far beyond the structural infarct burden, consistent with functional diaschisis [10-12]. Perfusion MRI (ASL) and nuclear imaging can detect diaschisis within hours of stroke onset and track its resolution; importantly, diaschisis correlates with clinical impairments and functional outcomes. Thalamic and cerebellar diaschisis after supratentorial stroke has been characterized using ASL, SPECT, PET, and diffusion imaging, supporting the concept that focal subcortical lesions can depress remote cortical territories through network disconnection.
Hemispatial neglect is commonly attributed to right-hemispheric cortical lesions; however, multiple studies document subcortical neglect after thalamic, striatal, and internal capsule strokes, presumably via disruption of cortico-subcortical attention networks [13-15]. This literature supports the interpretation that our patient’s neglect reflects network-level disconnection rather than a large cortical infarct, with the PLIC and LGN acting as strategic nodes. These observations are consistent with recent network-level models of poststroke diaschisis and reorganization [16,17].
Conclusions
Right AChA infarction may cause higher-order deficits when small lesions involve strategic subcortical hubs such as the PLIC and LGN. This case demonstrates that even minor focal injury can induce widespread hemispheric suppression consistent with network-level diaschisis. Recognizing this mechanism has direct clinical implications: fluctuations in consciousness or neglect in deep infarcts should not be misinterpreted as infarct extension, seizure activity, or therapeutic failure. Instead, early use of multimodal imaging (ASL, SPECT) and artifact-free EEG can help identify network dysfunction, avoid unnecessary escalation of antiepileptic or antithrombotic therapy, and guide appropriate rehabilitation planning. Therefore, awareness of diaschisis-related physiological depression can meaningfully influence diagnostic accuracy and clinical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arterial territories of the human brain Front Neurol Neurosci Tatu L Moulin T Vuillier F Bogousslavsky J 991103020122237787410.1159/000333602 · doi ↗ · pubmed ↗
- 2Anterior choroidal artery-territory infarction. Report of cases and review Arch Neurol Helgason C Caplan LR Goodwin J Hedges T 3rd 681686431986372974610.1001/archneur.1986.00520070039015 · doi ↗ · pubmed ↗
- 3Predicting human resting-state functional connectivity from structural connectivity Proc Natl Acad Sci U S A Honey CJ Sporns O Cammoun L Gigandet X Thiran JP Meuli R Hagmann P 2035204010620091918860110.1073/pnas.0811168106 PMC 2634800 · doi ↗ · pubmed ↗
- 4Diaschisis Stroke Feeney DM Baron JC 817830171986353243410.1161/01.str.17.5.817 · doi ↗ · pubmed ↗
- 5Diaschisis: past, present, future Brain Carrera E Tononi G 2408242213720142487164610.1093/brain/awu 101 · doi ↗ · pubmed ↗
- 6A lateralized brain network for visuospatial attention Nat Neurosci Thiebaut de Schotten M Dell'Acqua F Forkel SJ Simmons A Vergani F Murphy DG Catani M 124512461420112192698510.1038/nn.2905 · doi ↗ · pubmed ↗
- 7Exploring the functional connectome in white matter Hum Brain Mapp Li J Biswal BB Wang P Duan X Cui Q Chen H Liao W 433143444020193127626210.1002/hbm.24705 PMC 6865787 · doi ↗ · pubmed ↗
- 8A populational connection distribution map for the whole brain white matter reveals ordered cortical wiring in the space of white matter Neuroimage Lee D Park HJ 11916725420223537828710.1016/j.neuroimage.2022.119167 · doi ↗ · pubmed ↗