Effect of Chronic Pediatric Heart Conditions on Family Dynamics in Saudi Arabia: A Cross-Sectional Study
Aljuhara A Alsuayyid, Abdullah S Alosayl, Zahra H Al Dawood, Eman A Alzayer, Saleh S Alenazi, Yahya Almashham

TL;DR
This study explores how chronic heart conditions in children affect family life in Saudi Arabia, highlighting emotional and financial challenges and the need for better support systems.
Contribution
The study provides insights into family dynamics and coping strategies specific to Saudi Arabia's healthcare and cultural context.
Findings
Most families faced emotional stress and financial hardship due to the child's heart condition.
Over half of the families reported receiving emotional support from medical professionals but sought more specialized mental health help.
No significant demographic differences were found in the effects of the child's condition on families.
Abstract
Introduction: Chronic pediatric heart diseases significantly affect family dynamics, therefore affecting caregivers' emotional, financial, and social spheres of life. Understanding how healthcare systems and family structures differ in Saudi Arabia helps us improve support systems since they directly affect families. This study investigated how chronic pediatric cardiac diseases affected family dynamics and what elements supported caregivers' stress and coping strategies. Methods: Between February and March 2025, a cross-sectional survey was conducted at King Fahad Medical City (KFMC), Riyadh, Saudi Arabia. Through a self-administered survey, data were gathered from parents or main caregivers of children with chronic cardiac diseases, including congenital and acquired heart conditions. The aspects of family life evaluated in the survey were emotional effects, financial difficulty,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
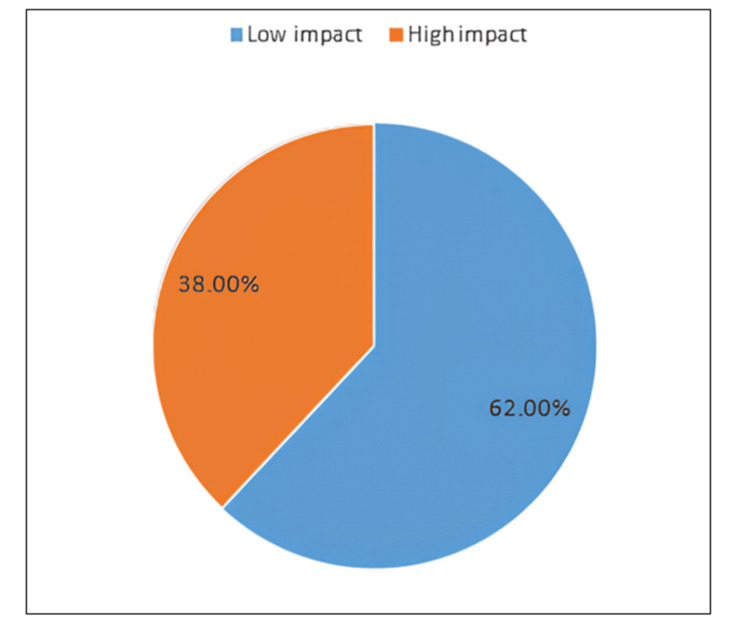 Figure 1
Figure 1| Count | Column N % | ||
| Age | Mean (SD) | 49.15 (52.7) | |
| Gender of child | Male | 58 | 58.0% |
| Female | 42 | 42.0% | |
| Nationality | Saudi | 92 | 92.0% |
| Non-Saudi | 8 | 8.0% | |
| Primary diagnosis | Septal defects | 59 | 59.0% |
| Right heart lesions | 10 | 10.0% | |
| Left heart lesions | 4 | 4.0% | |
| Coronary artery anomalies | 2 | 2.0% | |
| Electrophysiologic conditions | 6 | 6.0% | |
| Single ventricle | 10 | 10.0% | |
| CoA | 3 | 3.0% | |
| PDA | 6 | 6.0% | |
| Intervention | Not done | 59 | 59.0% |
| Surgery | 27 | 27.0% | |
| Catheterization | 10 | 10.0% | |
| Both | 4 | 4.0% | |
| Number of surgeries | Mean (SD) | 0.31 (0.48) | |
| Number of siblings | Mean (SD) | 3.02 (2.83) | |
| Count | Column, N% | ||
| Relation to child | Mother | 62 | 62.0% |
| Father | 36 | 36.0% | |
| Other (Aunt, Brother) | 2 | 2.0% | |
| Father's age | Mean (SD) | 40.3 (9.8) | |
| Father's education | NA | 3 | 3.0% |
| Illiterate | 2 | 2.0% | |
| Less than high school | 11 | 11.0% | |
| High school/Diploma | 37 | 37.0% | |
| Bachelor | 41 | 41.0% | |
| Master/PhD | 6 | 6.0% | |
| Father's job | NA | 3 | 3.0% |
| None | 2 | 2.0% | |
| Private sector | 28 | 28.0% | |
| Government | 33 | 33.0% | |
| Freelancer | 7 | 7.0% | |
| Military | 23 | 23.0% | |
| Retired | 4 | 4.0% | |
| Father alive | No | 2 | 2.0% |
| Yes | 98 | 98.0% | |
| Mother's age | Mean (SD) | 35.6 (8.2) | |
| Mother's education | NA | 2 | 2.0% |
| Illiterate | 3 | 3.0% | |
| Less than high school | 8 | 8.0% | |
| High school/Diploma | 32 | 32.0% | |
| Bachelor | 55 | 55.0% | |
| Master/PhD | 0 | 0.0% | |
| Mother's job | NA | 2 | 2.0% |
| None/Housewife | 76 | 76.0% | |
| Private sector | 6 | 6.0% | |
| Government | 5 | 5.0% | |
| Teacher | 8 | 8.0% | |
| Nurse | 3 | 3.0% | |
| Mother alive | No | 1 | 1.0% |
| Yes | 99 | 99.0% | |
| The child lives with | Both parents | 93 | 93.0% |
| Mothers | 6 | 6.0% | |
| Other (Aunt) | 1 | 1.0% | |
| Parents status | Married | 93 | 93.0% |
| Divorced | 5 | 5.0% | |
| Widow | 1 | 1.0% | |
| Both dead | 1 | 1.0% | |
| Time of diagnosis | Antenatal | 5 | 5.0% |
| Neonatal period | 64 | 64.0% | |
| Infancy | 18 | 18.0% | |
| After 1st year | 13 | 13.0% | |
| Never | Sometimes | Always | ||||
| Count | Row (N%) | Count | Row (N%) | Count | Row (N%) | |
| Stress due to the child's condition | 13 | 13.0% | 56 | 56.0% | 31 | 31.0% |
| Mood changes since diagnosis | 27 | 27.0% | 60 | 60.0% | 13 | 13.0% |
| Negative effect on the relationship with the partner | 76 | 76.0% | 20 | 20.0% | 4 | 4.0% |
| Strain due to the financial cost of treatment | 50 | 50.0% | 28 | 28.0% | 22 | 22.0% |
| Time for self-care activities | 28 | 28.0% | 54 | 54.0% | 18 | 18.0% |
| Experiencing guilt as a caregiver | 59 | 59.0% | 37 | 37.0% | 4 | 4.0% |
| Disrupted sleep due to the child's condition | 35 | 35.0% | 44 | 44.0% | 21 | 21.0% |
| Emotional support by healthcare professionals | 10 | 10.0% | 27 | 27.0% | 63 | 63.0% |
| Seeking professional support | 63 | 63.0% | 29 | 29.0% | 8 | 8.0% |
| Managing a child's needs confidently | 0 | 0.0% | 21 | 21.0% | 79 | 79.0% |
| Impact on family/future planning | 64 | 64.0% | 23 | 23.0% | 13 | 13.0% |
| Support from extended family | 12 | 12.0% | 26 | 26.0% | 62 | 62.0% |
| Frequent hospital admissions | 55 | 55.0% | 36 | 36.0% | 9 | 9.0% |
| Developmental impact | 53 | 53.0% | 30 | 30.0% | 17 | 17.0% |
| Impact | ||||||
| Low impact | High impact | P-value | ||||
| Count | Row (N%) | Count | Row (N%) | |||
| Gender of child | Male | 36 | 62.1% | 22 | 37.9% | 0.987 |
| Female | 26 | 61.9% | 16 | 38.1% | ||
| Nationality | Saudi | 59 | 64.1% | 33 | 35.9% | 0.137 |
| Non-Saudi | 3 | 37.5% | 5 | 62.5% | ||
| Primary diagnosis | Septal defects | 39 | 66.1% | 20 | 33.9% | 0.111 |
| Right heart lesions | 2 | 20.0% | 8 | 80.0% | ||
| Left heart lesions | 3 | 75.0% | 1 | 25.0% | ||
| Coronary artery anomalies | 2 | 100.0% | 0 | 0.0% | ||
| Electrophysiologic conditions | 3 | 50.0% | 3 | 50.0% | ||
| Single ventricle | 6 | 60.0% | 4 | 40.0% | ||
| CoA | 3 | 100.0% | 0 | 0.0% | ||
| PDA | 4 | 66.7% | 2 | 33.3% | ||
| Intervention | Not done | 39 | 66.1% | 20 | 33.9% | 0.548 |
| Surgery | 14 | 51.9% | 13 | 48.1% | ||
| Catheterization | 7 | 70.0% | 3 | 30.0% | ||
| Both | 2 | 50.0% | 2 | 50.0% | ||
| Father's education | NA | 2 | 66.7% | 1 | 33.3% | 0.473 |
| Illiterate | 0 | 0.0% | 2 | 100.0% | ||
| Less than high school | 8 | 72.7% | 3 | 27.3% | ||
| High school/Diploma | 22 | 59.5% | 15 | 40.5% | ||
| Bachelor | 27 | 65.9% | 14 | 34.1% | ||
| Master/PhD | 3 | 50.0% | 3 | 50.0% | ||
| Father's job | NA | 2 | 66.7% | 1 | 33.3% | 0.514 |
| None | 1 | 50.0% | 1 | 50.0% | ||
| Private sector | 16 | 57.1% | 12 | 42.9% | ||
| Government | 23 | 69.7% | 10 | 30.3% | ||
| Freelancer | 3 | 42.9% | 4 | 57.1% | ||
| Military | 16 | 69.6% | 7 | 30.4% | ||
| Retired | 1 | 25.0% | 3 | 75.0% | ||
| Father alive | No | 1 | 50.0% | 1 | 50.0% | 0.724 |
| Yes | 61 | 62.2% | 37 | 37.8% | ||
| Mother's education | NA | 1 | 50.0% | 1 | 50.0% | 0.083 |
| Illiterate | 0 | 0.0% | 3 | 100.0% | ||
| Less than high school | 3 | 37.5% | 5 | 62.5% | ||
| High school/Diploma | 20 | 62.5% | 12 | 37.5% | ||
| Bachelor | 38 | 69.1% | 17 | 30.9% | ||
| Master/PhD | 0 | 0.0% | 0 | 0.0% | ||
| Mother's job | NA | 1 | 50.0% | 1 | 50.0% | 0.371 |
| None/Housewife | 46 | 60.5% | 30 | 39.5% | ||
| Private sector | 2 | 33.3% | 4 | 66.7% | ||
| Government | 4 | 80.0% | 1 | 20.0% | ||
| Teacher | 6 | 75.0% | 2 | 25.0% | ||
| Nurse | 3 | 100.0% | 0 | 0.0% | ||
| Mother alive | No | 0 | 0.0% | 1 | 100.0% | 0.199 |
| Yes | 62 | 62.6% | 37 | 37.4% | ||
| The child lives with | Both parents | 57 | 61.3% | 36 | 38.7% | 0.245 |
| Mothers | 5 | 83.3% | 1 | 16.7% | ||
| Other (Aunt) | 0 | 0.0% | 1 | 100.0% | ||
| Parents' status | Married | 57 | 61.3% | 36 | 38.7% | 0.399 |
| Divorced | 4 | 80.0% | 1 | 20.0% | ||
| Widow | 1 | 100.0% | 0 | 0.0% | ||
| Both dead | 0 | 0.0% | 1 | 100.0% | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildhood Cancer Survivors' Quality of Life · Family and Patient Care in Intensive Care Units · Congenital Heart Disease Studies
Introduction
Chronic pediatric heart conditions, such as congenital heart defects, affect a significant number of children; these conditions can vary in severity and may require different treatments for each child [1,2]. While medical advances have improved survival rates, 95% of these children reach adulthood due to the success of modern treatment options [3]. Chronic pediatric heart conditions pose significant challenges for the child and their families. Parents of children with congenital heart disease (CHD) are more susceptible to psychological and social distress [4], high levels of parenting stress, poor sleep, and elevated psychological maladjustment [5]. The challenges the condition presents can affect the family at various stages, from diagnosis through childhood. The diagnosis of CHD, paired with subsequent surgical and interventional treatments and prolonged hospital stays, causes acute psychological distress and can lead to post-traumatic stress disorder (PTSD) [6]. The ongoing care and uncertainty often create emotional, financial, and social strains on family members. These strains can significantly impact their roles, relationships, and coping mechanisms, highlighting the profound effect of these conditions on family dynamics. Family socioeconomic status is an essential factor associated with health-related quality of life (HRQOL) in patients with critical congenital heart disease [7]. In addition to higher levels of anxiety and depression in CHD parents, they reported lower confidence in their abilities to parent. Clinicians must identify at-risk parents early to provide them with systematic support [6]. The National Institute for Health and Care Excellence (NICE) recommends that children with CHD and their families may need support and psychological help to cope with the emotional challenges that come with managing this condition [3]. Despite a wealth of research on medical outcomes, there is limited exploration of how these conditions affect family dynamics in Saudi Arabia. This study aims to fill this gap by examining how chronic pediatric heart conditions influence family interactions and overall functioning. The findings will enhance our understanding of these conditions and provide valuable insights to help healthcare providers, social workers, and policymakers create better support systems for affected families.
Materials and methods
This study employed a cross-sectional survey design, using a questionnaire to gather data from families of children with chronic heart conditions receiving treatment at King Fahad Medical City (KFMC). Data collection took place between February 2025 and March 2025. Families attending the pediatric cardiology department as inpatients and outpatients were approached to participate.
The target population for the study included parents or primary caregivers of children diagnosed with chronic heart conditions at KFMC. The inclusion criteria specified that families of children under 14 years who had a diagnosed chronic heart condition (e.g., congenital heart defects or acquired heart diseases) were eligible for participation. Both parents or caregivers were invited to participate, with the option of one or both completing the questionnaire.
The exclusion criteria included families of children not receiving care for heart conditions during the study period, syndromic patients, and children with non-cardiac diseases.
Data were collected through a self-administered questionnaire designed to assess various aspects of family dynamics, including the emotional, financial, and social impacts of caring for a child with a chronic heart condition. The questionnaire included both close-ended and open-ended questions to provide a comprehensive understanding of the family experience. Key areas of inquiry included emotional impact, social and relationship dynamics, financial burden, coping strategies, and the availability and effectiveness of support systems.
Close-ended questions provided quantitative data on stress levels, relationship changes, and financial strain, while open-ended questions allowed personal narratives and insights into family adjustment and coping mechanisms.
Following ethical approval by KFMC, families were approached during routine visits to the pediatric cardiology department. Parents and caregivers were fully informed about the purpose of the study, the voluntary nature of participation, and the confidentiality of the data. Those who agreed to participate were provided with the questionnaire, which they could complete at their own pace, either in the hospital or at home. The completed questionnaires were expected to be submitted by the end of the study period in March 2025.
The collected data were analyzed using descriptive statistics to summarize demographic information and assess the impact of chronic pediatric heart conditions on family dynamics. Frequencies, percentages, and mean scores were calculated for close-ended questions. Open-ended responses were subjected to thematic analysis, which involved identifying recurring themes and patterns related to family experiences and coping strategies. This analysis aimed to provide a deeper understanding of the emotional, social, and financial challenges faced by families.
The study adhered to ethical guidelines, ensuring all participants provided informed consent. Participants were made aware of the study's purpose, the voluntary nature of their involvement, and their right to confidentiality. All personal identifying information was kept confidential and securely stored in compliance with ethical and social research standards.
Results
As shown in Table 1, the study included 100 children with chronic heart conditions, with a mean age of 49.15 months (SD = 52.7). Males represented 58% (58) of the sample, while females accounted for 42% (42). Most of the children were Saudi nationals (92%), and the most common primary diagnosis was septal defects (59%), followed by right heart lesions (10%) and single ventricle conditions (10%). More than half of the children (59%) had not undergone any interventions, whereas 27 (27%) and 10 (10%) underwent catheterization. The average number of siblings was 3.02 (SD = 2.83), indicating that most children came from moderately sized families.
Table 2 summarizes the demographic characteristics of parents and caregivers. Most respondents were mothers (62%), followed by fathers (36%), with an average maternal age of 35.6 years (SD = 8.2) and paternal age of 40.3 years (SD = 9.8). Most fathers (41%) and mothers (55%) hold a bachelor's degree. Employment status varied, with 33% of fathers working in government jobs and 28% in the private sector, while most mothers (76%) were housewives. Almost all children (93%) live with both parents, and most parents were married (93%). Most children were diagnosed during the neonatal period (64%), reflecting early detection and management of cardiac conditions.
Table 3 illustrates the impact of chronic pediatric heart conditions on family dynamics. A significant proportion of parents reported experiencing stress due to the child’s condition, with 56% experiencing stress sometimes and 31% always. Mood changes since the diagnosis were also common, with 60% of respondents experiencing mood changes sometimes. The relationship with the partner was most often reported as unaffected (76%), although 20% of parents reported occasional negative effects. Financial strain due to treatment costs was a notable issue, with 50% of families reporting financial strain sometimes and 22% always. Regarding self-care, 54% of families sometimes struggled to find time for themselves. A significant number of parents (59%) experienced guilt as caregivers, with 37% reporting it sometimes. Disrupted sleep due to the child's condition was a concern for 44% of families. Support from healthcare professionals was highly valued, with 63% reporting always receiving emotional support. Despite this, a significant number of parents (63%) sought professional support for mental health. Managing the child’s needs with confidence was reported by 79% of respondents, reflecting high levels of coping confidence. Additionally, 64% of families reported that the child’s condition affected future family planning.
Figure 1 visually represents the overall impact of chronic pediatric heart conditions on family dynamics in Saudi Arabia. It shows that 62% of families reported a low impact, while 38% reported a high impact, indicating a substantial portion of families affected by the condition.
Impact of chronic pediatric heart conditions on family dynamics in Saudi Arabia
Table 4 explores the relationship between the impact of the child's condition and various demographic factors. The analysis revealed no significant difference in the effects based on the child’s gender (p = 0.987) or nationality (p = 0.137). Regarding the primary diagnosis, children with right heart lesions and coronary artery anomalies showed a higher proportion of high-impact responses (80% and 100%, respectively); however, these differences were not statistically significant (p = 0.111). The type of intervention also showed no significant association with the reported level of impact (p = 0.548). Similarly, the father’s education level and occupation, as well as the mother's education level, did not show significant differences in reported impact, with p-values ranging from 0.083 to 0.514. Family status was also not significantly associated with the impact level. This was reflected in the responses of children living with both parents (p = 0.245), divorced parents (p = 0.399), and children of widowed parents (p = 0.199).
Discussion
The findings of this research offer valuable insights into the demographic profile and the impact of chronic pediatric cardiac conditions on family dynamics in Saudi Arabia. The predominance of male patients (58; 58%) aligns with earlier research reporting a higher incidence of congenital heart abnormalities among males [8,9]. A large proportion of children were Saudi nationals, reflecting the demographic composition of the patient population served by KFMC. Consistent with international literature showing that septal defects are among the most prevalent congenital cardiac anomalies, septal defects were the most frequent primary diagnosis in this cohort (59; 59%), highlighting their common occurrence and the continuing need for targeted clinical and supportive intervention [10,11].
With regard to treatment patterns, the fact that a large proportion of children (59; 59%) had not undergone any intervention may reflect the variability in the severity of heart conditions and the availability of alternative management options, such as medication or regular monitoring [12]. Meanwhile, the number of children requiring invasive procedures is reflected in the relatively high proportion who underwent surgery (27; 27%) or catheterization (10; 10%) [13]. Medical procedures used to treat difficult pediatric heart diseases are typically performed in specialized hospitals. The mean number of surgeries per child (0.3) and the average number of siblings (3.02) are consistent with earlier research, reflecting moderate family sizes in the region and variability in surgical needs depending on each child’s condition and response to treatment [14].
A significant concern identified in this study was the financial burden, with 22 (22%) families reporting a high financial strain. This is consistent with global literature showing that families managing chronic pediatric illnesses often face substantial economic challenges, particularly in healthcare systems with mixed public-private structures [15].
Additionally, 54 (54%) families occasionally struggled to find time for self-care, and 44 (44%) reported disrupted sleep. These findings underscore the personal toll caregiving takes on parents, a topic widely documented in the caregiving literature [16-18].
Emotional support from medical professionals was reported as consistently helpful, with 63 (63%) respondents saying they always received emotional support. This underscores the importance of comprehensive care that addresses both the medical and emotional needs of the child and family [19]. However, despite receiving emotional support, 63 (63%) parents also sought professional mental health services, indicating that the existing support system may fall short of fully meeting the psychological needs of caregivers [20].
Despite these challenges, a significant number of parents reported high confidence in managing their child's condition, 79 (79%). This reflects the resilience and adaptive coping strategies frequently observed among parents of children with chronic illnesses [21].
Statistical analysis revealed no significant differences in the reported impact based on the child’s gender or nationality, suggesting that the burden of chronic pediatric heart conditions is broadly similar across these variables. However, families of children diagnosed with coronary artery anomalies or right heart lesions reported a higher proportion of severe impact, consistent with the more complex nature of these conditions and the need for intensive treatment. These cases may place increased emotional, financial, and logistical strain on families [22,23]. Interestingly, the type of intervention did not significantly influence the perceived impact, suggesting that the other factors, such as the child’s overall health status and the family’s coping mechanisms, play a more critical role in shaping family dynamics.
This study has several limitations. First, the relatively small sample size of 100 families makes it difficult to apply the findings to all families of children with chronic heart conditions in Saudi Arabia. Second, the cross-sectional design provides information from one point in time and cannot show how families' experiences or stress levels may change over time. Third, the study was conducted at a single tertiary care center, so the results may not reflect experiences in other regions or health care settings with different socioeconomic or cultural backgrounds. Finally, the reliance on self-reported data introduces the possibility of response bias, as participants may underreport or overreport emotional, financial, or social challenges. Despite these limitations, this study provides valuable preliminary insights into the emotional, social, and financial challenges faced by families of children with chronic heart conditions in Saudi Arabia. These findings highlight areas of further investigation and may serve as a foundation for future research using larger, multicenter, and longitudinal designs.
Conclusions
In essence, the findings of this research highlight that chronic pediatric heart conditions have significant emotional, social, and financial impacts on families in Saudi Arabia. These results underscore the need for more holistic healthcare approaches that encompass both medical treatment and comprehensive family support services. Such services should include caregiver education, stress management strategies, and a financial assistance program to help families navigate the challenges of caregiving.
Further research is needed to explore the long-term effects of these conditions on family relationships and to evaluate the effectiveness of support programs designed to assist families throughout the treatment journey.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heart failure in pediatric patients with congenital heart disease Circ Res Hinton RB Ware SM 97899412020172830274310.1161/CIRCRESAHA.116.308996 PMC 5391045 · doi ↗ · pubmed ↗
- 2Global, regional, and national epidemiology of congenital heart disease in children from 1990 to 2021 Front Cardiovasc Med Xu J Li Q Deng L Xiong J Cheng Z Ye C 15226441220254045424210.3389/fcvm.2025.1522644 PMC 12122482 · doi ↗ · pubmed ↗
- 3Current research status on the psychological situation of parents of children with congenital heart disease Cardiovasc Diagn Ther Biber S Andonian C Beckmann J 0769201910.21037/cdt.2019.07.07PMC 683793031737543 · doi ↗ · pubmed ↗
- 4Coping in parents of children with congenital heart disease: a systematic review and meta-synthesis J Child Fam Stud Lumsden MR Smith DM Wittkowski A 17361753282019
- 5Parenting stress, sleep, and psychological adjustment in parents of infants and toddlers with congenital heart disease J Pediatr Psychol Bishop MN Gise JE Donati MR Shneider CE Aylward BS Cohen LL 9809874420193132992610.1093/jpepsy/jsz 026 · doi ↗ · pubmed ↗
- 6Surgery-related posttraumatic stress disorder in parents of children undergoing cardiopulmonary bypass surgery: a prospective cohort study Pediatr Crit Care Med Helfricht S Latal B Fischer JE Tomaske M Landolt MA 217223920081847793610.1097/PCC.0b 013e 318166 eec 3 · doi ↗ · pubmed ↗
- 7Impact of family socioeconomic status on health-related quality of life in children with critical congenital heart disease J Am Heart Assoc Xiang L Su Z Liu Y Huang Y Zhang X Li S Zhang H 08201910.1161/JAHA.118.010616 PMC 640571030563422 · doi ↗ · pubmed ↗
- 8Gender differences in congenital heart defects: a narrative review Transl Pediatr Pugnaloni F Felici A Corno AF Marino B Versacci P Putotto C 175317641220233781471910.21037/tp-23-260PMC 10560357 · doi ↗ · pubmed ↗