Patient Attitudes About Light Therapy and Negative Ion Therapy for Nonseasonal Depression: An Online Survey Study
Orli S Hellerstein, Iman Lahouaoula, Victor W Li, Aidan Scott, Andre Do, Erin E Michalak, Jill K Murphy, Samantha Huang, Vanessa K Evans, Raymond W Lam

TL;DR
People with depression are aware of light and negative ion therapy and are open to using them as non-medication options for ongoing treatment.
Contribution
This study is the first to assess patient attitudes toward using light and negative ion therapy as maintenance treatments for depression.
Findings
Most participants were aware of light therapy (95%) compared to negative ion therapy (63%).
Participants found both therapies easy to use and were open to using them instead of antidepressants.
77% of participants would likely volunteer for a clinical trial on these therapies.
Abstract
Objective: No studies have evaluated the feasibility of light therapy or negative ion therapy as maintenance treatments after acute antidepressant treatment in major depressive disorder. To address this gap, we surveyed people with depression about their knowledge and attitudes about light therapy and negative ion therapy, and their willingness to participate in a clinical trial of maintenance treatment with these therapies. Methods: Participants with a self-reported diagnosis of depression completed a researcher-generated online survey, created for this study, examining awareness and effectiveness of light therapy and negative ion therapy, which included vignettes describing the use of these therapies for maintenance treatment. Participants were asked about the feasibility and reasons for wanting (and not wanting) to use the therapies instead of antidepressants. Response frequencies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
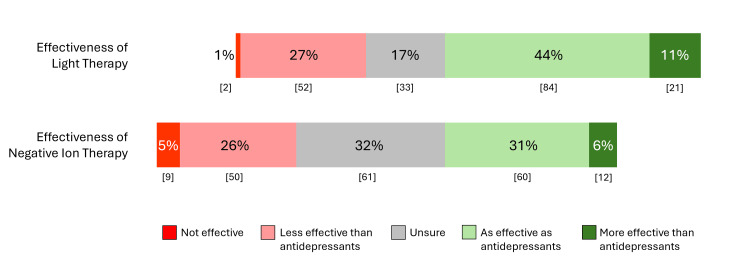 Figure 1
Figure 1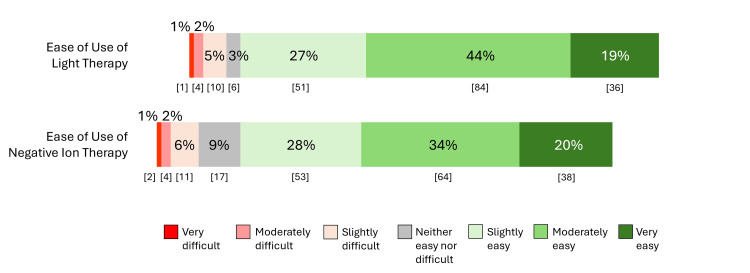 Figure 2
Figure 2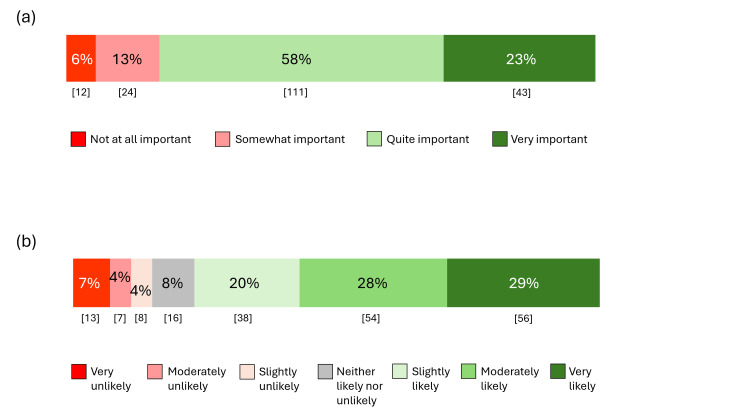 Figure 3
Figure 3| Category | Responses | Counts (n) | Percentage |
| Age in years (n=193) | 19-24 | 48 | 25 |
| 25-49 | 115 | 60 | |
| 50-64 | 30 | 15 | |
| Gender (n=193) | Woman | 125 | 65 |
| Man | 50 | 26 | |
| Transgender/Trans | 6 | 3 | |
| Another gender | 2 | 1 | |
| Prefer not to answer | 10 | 5 | |
| Ethnic Background (n=193) | Black, African, Caribbean | 5 | 3 |
| East Asian | 7 | 4 | |
| Latin American | 9 | 5 | |
| Indigenous | 4 | 2 | |
| Native American | 7 | 4 | |
| Middle Eastern | 5 | 3 | |
| South Asian | 0 | 0 | |
| White/European | 141 | 73 | |
| Other/Multiple | 12 | 6 | |
| Prefer not to answer | 2 | 1 | |
| Education (n=192) | Did not finish high school | 2 | 1 |
| High School | 20 | 10 | |
| Some post-secondary | 29 | 15 | |
| Post-secondary | 29 | 15 | |
| Undergraduate Degree | 89 | 46 | |
| Postgraduate degree or professional degree | 23 | 12 | |
| Employment Status (n=191) | Employed full-time | 81 | 42 |
| Employed part-time | 28 | 15 | |
| Self-employed | 32 | 17 | |
| Student | 16 | 8 | |
| Stay-at-home parent | 8 | 4 | |
| Not employed | 15 | 7 | |
| Disability leave | 5 | 3 | |
| Retired | 5 | 3 | |
| Other | 2 | 1 | |
| Living Area (n=190) | Urban | 105 | 55 |
| Suburban | 69 | 36 | |
| Rural or remote area | 16 | 8 |
| Category | Responses | Count (n) | Percentage |
| Taking Antidepressants (n=193) | Taking currently | 94 | 49 |
| Taken in the past | 92 | 48 | |
| Never taken | 7 | 4 | |
| Duration of Current Antidepressant Use (n=94) | Less than 6 months | 21 | 22 |
| 6-24 months | 28 | 30 | |
| More than 24 months | 45 | 48 | |
| Satisfaction with Current Antidepressant (n=94) | Very satisfied | 22 | 23 |
| Slightly satisfied | 40 | 43 | |
| Neither satisfied nor dissatisfied | 21 | 22 | |
| Slightly unsatisfied | 8 | 9 | |
| Very unsatisfied | 2 | 2 | |
| Knowledge about depression treatment (n=193) | Very knowledgeable | 56 | 29 |
| Moderately knowledgeable | 111 | 58 | |
| Somewhat knowledgeable | 25 | 13 | |
| Not at all knowledgeable | 0 | 0 |
| Category | Responses | Count (n) | Percentage |
| Wanting to use light therapy instead of medications* | It is a non-medication treatment | 72 | 37 |
| It has fewer side effects | 92 | 47 | |
| I don’t like taking medications | 61 | 32 | |
| I have side effects from medication | 50 | 26 | |
| It seems like a natural treatment | 46 | 24 | |
| Other | 12 | 6 | |
| Wanting to use negative ion therapy instead of medications* | It is a non-medication treatment | 67 | 35 |
| It has fewer side effects | 71 | 37 | |
| I don’t like taking medications | 71 | 37 | |
| I have side effects from medication | 61 | 32 | |
| It seems like a natural treatment | 32 | 17 | |
| Other | 7 | 4 | |
| What would stop you from using light therapy instead of medications?* | I’m worried it won’t work | 62 | 32 |
| I don’t like the side effects | 32 | 17 | |
| I don’t have time to do light therapy | 51 | 26 | |
| I can’t afford to buy a light device | 30 | 16 | |
| I’m worried about withdrawal effects from stopping the antidepressants | 48 | 25 | |
| Other | 10 | 5 | |
| What would stop you from using negative ion therapy instead of medications?* | I’m worried it won’t work | 73 | 38 |
| I don’t like the side effects | 33 | 17 | |
| I don’t have time to do negative ion therapy | 51 | 26 | |
| I can’t afford to buy a negative ion device | 31 | 16 | |
| I’m worried about withdrawal effects from stopping the antidepressants | 54 | 28 | |
| Other | 10 | 5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCircadian rhythm and melatonin · Treatment of Major Depression · Laser Applications in Dentistry and Medicine
Introduction
Major depressive disorder (MDD) affects approximately 264 million people worldwide and is one of the top three medical causes of years lived with disability [1]. Amongst the many evidence-based treatment options for MDD, antidepressants are recommended as first-line treatments for moderate to severe depression [2]. Once patients have recovered from an acute depressive episode, maintenance antidepressant treatment is recommended for 6-24 months, or longer, to prevent relapse and recurrence [2]. Several meta-analyses of randomized controlled trials (RCTs) have confirmed that maintenance antidepressants are effective in preventing relapse [3-5].
Despite the evidence for maintenance, patients often discontinue antidepressants too early after acute treatment [6]. This puts them at risk of relapse and consequent impairment in functioning and quality of life. Some studies suggest that less than 30% of patients continue antidepressants for more than three months [7]. Some patients stop antidepressants prematurely due to persistent side effects, including sexual dysfunction and weight gain; cost; adverse effects with long-term use of antidepressants (e.g., osteoporosis, gastrointestinal bleeding, and risk of drug interactions with medications for other medical conditions); and patient preference for non-medication treatments [8].
Given the reluctance for longer-term use of antidepressants, perhaps patients would consider using non-medication treatments such as bright light therapy and negative ion therapy to substitute for antidepressants during maintenance treatment. Light therapy involves daily exposure to bright light (e.g., 10,000 lux) from a light device usually constructed with fluorescent bulbs or light-emitting diodes [9]. Light therapy has long been considered a first-line treatment for seasonal affective disorder (SAD) [10,11], and increasing evidence supports its efficacy in nonseasonal MDD [12-14] and bipolar depression [15,16]. Negative ion therapy is delivered with a desktop ion generator, similar to an air purifier, that produces invisible air ions at a flow rate of 4.5 x 1014 ions/second or higher [17]. Studies of high-density negative ion treatment have also shown positive results in reducing depressive symptoms [18-21]. Both these treatments are safe and well-tolerated, with mild side effects that are less frequent and less severe than with antidepressants [9,19,22].
While light therapy and negative ion therapy seem promising for antidepressant substitution, neither treatment has been studied for maintenance treatment or relapse prevention. Rigorous RCTs are needed to demonstrate efficacy and safety, but it is unclear whether patients would find light therapy and negative ion therapy acceptable substitutes for maintenance treatments, given that they are not widely used in clinical practice. Patient engagement is now an established principle in all aspects of health research, including formulating research questions [23]. The current study examined participants' self-reporting a diagnosis of depression to determine (1) the importance of alternative non-medication treatment of MDD from a patient perspective, (2) their familiarity with light and ion therapy, and (3) the feasibility of conducting an RCT with light and ion therapy for maintenance treatment of MDD. A previous version of this article was deposited at the MedRxiv preprint server [24].
Materials and methods
Participants
This study received approval from the Behavioural Research Ethics Board at the University of British Columbia (H20-01244). This exploratory, cross-sectional survey study was conducted with a convenience sample between July 17th, 2020, and July 7th, 2021. Participants were recruited from various sources, including social media postings, newsletters, and research networks in Canada. Inclusion criteria were (1) age 19-65 years; (2) diagnosed with depression by a physician or psychologist, by self-report; (3) capable of informed consent; (4) access to an internet-enabled computer or mobile device; and (5) able to read and understand English. Any participants who did not meet the inclusion criteria were excluded.
Assessments
The authors created a questionnaire for this study, comprised of 3 sections (see Appendix). Section 1 included 16 questions on participant demographics, whether they had been diagnosed with depression by a physician or psychologist, and whether they were taking, or had taken in the past, antidepressant medications.
Section 2 contained four questions addressing self-reported knowledge, opinions, and attitudes about light and ion treatments. Information stems were first presented, such as “Light therapy is a treatment for depression that uses daily exposure to bright light from a light box device used at home. Light therapy usually has fewer side effects than antidepressant medications,” followed by the questions “Have you heard of light therapy for depression?” and “In your opinion, how effective is light therapy for depression treatment?” The latter question included the responses “More effective than antidepressants,” “As effective as antidepressants,” “Less effective than antidepressants,” “Not effective,” and “Unsure.” A similar stem and the same questions were presented for negative ion therapy.
Section 3 contained 11 questions addressing substitution treatments for antidepressants in maintenance treatment of depression (see Appendix). Following a vignette for antidepressant maintenance treatment, participants were asked, “In your opinion, how important is it to substitute an evidence-based non-medication treatment for antidepressants for maintenance treatment?” with responses of “Very important,” “Quite important,” “Somewhat important,” and “Not at all important.” Then, two vignettes with identical phrasing were presented for substituting light and ion therapy for maintenance treatment, each followed by a question, “How easy would it be for you to use light/ion therapy as described?”
The survey also included vignettes (Appendix, Vignettes 4 and 5) to illustrate an individual’s use of light/ion therapy, describing the cost, time frame, and schedule, each followed by a question, “How easy would it be for you to use light/ion therapy as described?” with responses on a 7-point Likert scale ranging from “Very easy” to “Very difficult.” Open-ended questions asked participants to write reasons why they would want or would not want the treatments. A final vignette was presented with the procedures for an RCT of active versus inactive treatment with light and ion therapy for maintenance treatment (Appendix, Vignette 6), followed by a question asking, “How likely would you be to volunteer for this study?” with responses on a 7-point Likert scale ranging from “Very likely” to “Very unlikely.”
Procedure
All survey data were collected electronically using Qualtrics. Participants provided informed consent before starting the online survey.
Statistical analysis
All statistical analysis was conducted using IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 29.0. Armonk, NY: IBM Corp. [25]. As this was an exploratory study, there was no precalculated sample size. The survey data are reported in counts and percentages, not including missing data. For some statistical comparisons of frequency of responses between groups, response categories were combined to create a unified measure, e.g., for perception of effectiveness of the treatments, we deemed treatment as “effective” by combining responses of “as effective as antidepressants” and “more effective than antidepressants.” Chi-square (χ2) tests were used to compare frequencies, with a significance level p set at less than 0.05.
Results
A total of 221 individuals responded to the survey. Of these individuals, 193 self-reported a diagnosis of depression and are included in the analysis. Table 1 shows the demographic data of this sample. The majority of the depressed sample identified as women (n=125, 65%), reported an age in the 25-49 years bracket (n=115, 60%), self-identified as white/European (n=141, 73%), had an undergraduate or postgraduate/professional degree (n=112, 58%), were employed (n=141 of 191 responses, 74%), and lived in an urban area (n=105 of 190 responses, 55%).
Table 2 shows treatment information for the respondents. Most of them were currently taking antidepressants (n=94, 49%) or had taken them in the past (n=92, 48%). Of those currently taking antidepressants (n=94), the majority had taken them for over 6 months (n=73, 78%). In regard to satisfaction with the antidepressant, 62 (66%) respondents were “very satisfied” or “slightly satisfied,” while only 10 (11%) respondents were “slightly unsatisfied” or “very unsatisfied. The majority of participants also reported that they were knowledgeable of depression treatments in general, with 167 (87%) responding “very knowledgeable” or “moderately knowledgeable.” Significantly more of the respondents had heard of light therapy (n=183 [95%]) for depression compared to negative ion therapy (n=121 [63%]; χ2=59.7, df=1, p<0.0001). Also, significantly more participants had used light therapy (n = 56 [29%]) than had used negative ion therapy (n = 32 [17%]; χ2 = 8.3, df = 1, p = 0.004).
Figure 1 displays the percentage responses for perceived effectiveness of light therapy and negative ion therapy (Appendix, Q18 and Q20). The number of respondents who regarded light therapy as “more effective” or “as effective” as antidepressants was significantly higher than for negative ion therapy (105 [54%] vs. 72 [37%], respectively; χ2=11.41, df=1, p<0.001). There were also significantly fewer respondents who were “Unsure” of the effectiveness of light therapy than negative ion therapy (33 [17%] vs. 61 [32%], respectively; χ2=11.04, df=1, p<0.001).
Responses on perceived effectiveness of negative ion therapy and light therapy (n = 192)Numbers in brackets indicate counts.
Figure 2 displays the responses for perceived ease of use of the two therapies for maintenance treatment (Appendix, Q22 and Q23). There was no significant difference in whether treatments were regarded as easy to use, with 171 (89%) of participants regarding light therapy as “slightly” to “very easy” to use compared to 155 (82%) for negative ion therapy (χ2=3.83, df=1, p >0.05).
Responses about perceived ease of use of light therapy (n = 192) and negative ion therapy (n = 188)Numbers in brackets indicate counts
Regarding the main reasons for wanting to use and reasons for not wanting to use light therapy or negative ion therapy for maintenance treatment, respondents were offered the opportunity to select as many responses as they wanted (Table 3). The top three individual reasons for wanting to use light or negative ion therapy instead of antidepressants were “it has fewer side effects,” “it is a non-medication treatment,” and “I don’t like taking medications.” The top three individual reasons for not wanting to use light therapy or negative ion therapy were “I’m worried it won’t work,” “I’m worried about withdrawal effects from stopping antidepressants,” and “I don’t have time to do the therapy.”
Figure 3(a) displays the responses about the importance of finding substitute non-medication treatments for maintenance treatment (Appendix, Q21). Generally, support for the need for non-medication therapies was strong, with 154 (81%) participants identifying it as either “very important” or “quite important”; only 12 (6%) viewed it as “not at all important.” Figure 3(b) displays the responses about an RCT for light and negative ion therapies for maintenance treatment (Appendix, Table 4, Vignette 6, and Q29). A total of 148 (77%) respondents endorsed that they would be “very likely,” “moderately likely,” or “slightly likely” to volunteer for the study.
(a) Importance of finding substitute non-medication therapies for maintenance treatment (n=190). (b) Likelihood to volunteer for the randomized study (n=192).Numbers in brackets indicate counts.
Discussion
Patient engagement in research shows evidence for a positive impact, even at early stages of formulating research questions [23,26]. Our online survey of participants who self-reported a diagnosis of depression examined their opinions about light therapy and negative ion therapy and the importance of a trial of maintenance treatment for MDD. The demographic profile of participants (middle-aged, female, White/European ethnicity, university educated) mirrors that of most RCTs for depression treatments. This sample of participants was generally familiar with both treatments, although a significantly higher percentage of participants had heard of light therapy than negative ion therapy (95% vs. 63%, p<0.0001) and had used light therapy (29% vs. 17%, p<0.004). Similarly, a significantly higher percentage of the sample believed that the effectiveness of light therapy was similar to or better than antidepressants compared to negative ion therapy (55% vs. 38%, p<0.001), with more “unsure” about the effectiveness of negative ion therapy (32% vs. 17%, p<0.001). These differences may be expected since light therapy has been widely reported in the media as an effective treatment for SAD and is endorsed by clinical guidelines for depression [2,27], whereas negative ion therapy is still largely limited to research studies.
Both treatments were regarded by respondents as easy to use, with no significant differences between the two. The reasons for wanting to use the treatments were similar across the two therapies, suggesting that they represent general attitudes about non-medication therapies versus medications rather than specifically for one therapy over the other. Having fewer side effects was the top reason for wanting to use both therapies. Reasons for not wanting to use light therapy and negative ion therapy were again similar for both, including apprehension about their effectiveness and about withdrawal effects from stopping antidepressants. Few respondents were concerned about the cost of the devices (16%) or about withdrawal effects when using the light device (25%) or the negative ion device (28%).
Finally, the sample felt strongly about the need for finding alternative non-medication treatments for relapse prevention of depression, with over three-quarters of the sample (81%) finding this an important question to study. A similar percentage of participants (77%) was likely to volunteer for an RCT for maintenance treatment using one of these therapies.
This study is the first to survey people with a diagnosis of depression about their self-reported knowledge, attitudes, and opinions of light and ion therapy as a treatment for depression. The study had limitations, including a non-representative convenience sample recruited by email and social media, which limited the participants to those with internet access. The survey used was researcher-generated, and the questions have not been validated. In addition, the diagnosis of depression was based on self-report, and it is unclear whether the treatments previously used were prescribed or supervised by health care professionals. Finally, as with most online survey studies, we were unable to assess the participants’ level of knowledge about the treatments, their level of engagement with the study vignettes and questions, or their continued focus throughout the process. Nonetheless, given these positive patient survey results, we are now conducting a multicenter RCT (ClinicalTrials, NCT05423275) to address the question of whether these non-medication therapies can substitute for antidepressants as maintenance treatments for depression.
Conclusions
In conclusion, this online survey showed that people with depression had good familiarity with light therapy and negative ion therapy. Participants expressed positive attitudes towards their potential for maintenance treatment of depression, especially their ease of use. There was endorsement of the importance of finding alternative non-medication treatments to substitute for antidepressants for maintenance treatment, and the majority would likely participate in a randomized study. The findings show that, from a patient perspective, it is important and feasible to investigate the efficacy and safety of light and ion treatments for relapse prevention in patients with MDD. Future research should include the views of patients in the design of clinical trials for these new treatments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 1789185839220183049610410.1016/S 0140-6736(18)32279-7PMC 6227754 · doi ↗ · pubmed ↗
- 2Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes Can J Psychiatry Lam RW Kennedy SH Adams C 6416876920243871135110.1177/07067437241245384 PMC 11351064 · doi ↗ · pubmed ↗
- 3Discontinuation of antidepressants after remission with antidepressant medication in major depressive disorder: a systematic review and meta-analysis Mol Psychiatry Kato M Hori H Inoue T 1181332620213270406110.1038/s 41380-020-0843-0PMC 7815511 · doi ↗ · pubmed ↗
- 4Relapse and its modifiers in major depressive disorder after antidepressant discontinuation: meta-analysis and meta-regression Mol Psychiatry Kishi T Sakuma K Hatano M 9749762820233656448810.1038/s 41380-022-01920-0PMC 10005929 · doi ↗ · pubmed ↗
- 5Prevention of relapse and recurrence in adults with major depressive disorder: systematic review and meta-analyses of controlled trials Int J Neuropsychopharmacol Sim K Lau WK Sim J 19201510.1093/ijnp/pyv 076PMC 477281526152228 · doi ↗ · pubmed ↗
- 6Continuity of antidepressant treatment for adults with depression in the United States Am J Psychiatry Olfson M Marcus SC Tedeschi M Wan GJ 10110816320061639089610.1176/appi.ajp.163.1.101 · doi ↗ · pubmed ↗
- 7Time to lack of persistence with pharmacological treatment among patients with current depressive episodes: a natural study with 1-year follow-up Patient Prefer Adherence Li K Wei Q Li G 220922151020162782202110.2147/PPA.S 109941 PMC 5096725 · doi ↗ · pubmed ↗
- 8Antidepressant self-discontinuation: results from the collaborative psychiatric epidemiology surveys Psychiatr Serv Samples H Mojtabai R 4554626620152593022310.1176/appi.ps.201400021 · doi ↗ · pubmed ↗