Salvage of undeflatable intra-stent angioplasty-balloon-catheter with direct percutaneous needle puncture
Leonardo Pasquetti, Edoardo Pasqui, Giuseppe Galzerano, Elisa Lazzeri, Bruno Gargiulo, Gianmarco de Donato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
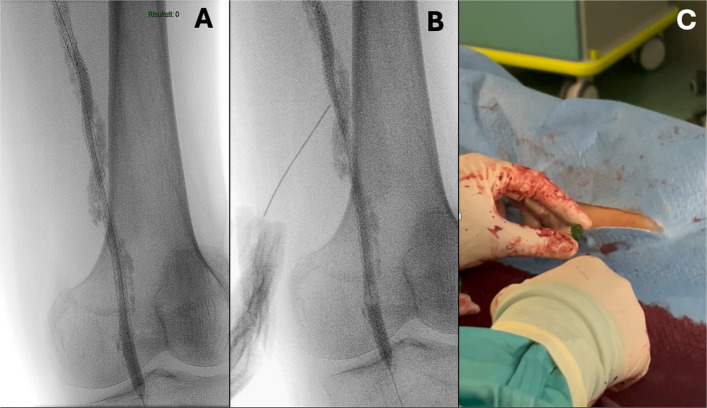 Figure 1
Figure 1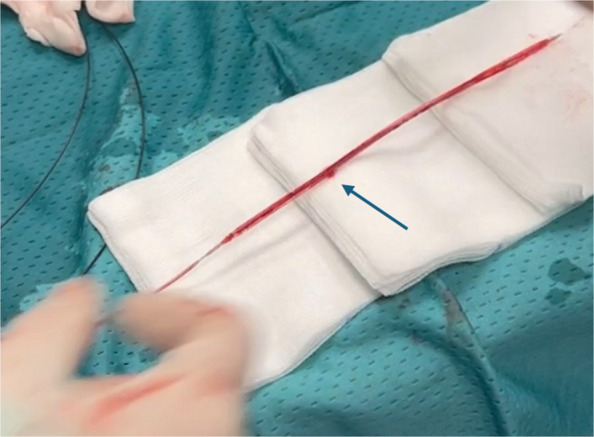 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Vascular Procedures and Complications · Coronary Interventions and Diagnostics
Main text
Background
To the Editor,
Balloon angioplasty and stenting are standard components of endovascular treatment for peripheral arterial disease. Although balloon inflation and deflation are routine steps, failure of a balloon to deflate is an exceptionally rare but potentially dangerous complication [1]. Evidence from coronary interventions exists, but applicability to peripheral vessels is limited due to differences in vessel calibre, calcium burden, and device design [2]. Here, we describe a case of balloon deflation failure inside a stented superficial femoral artery (SFA), successfully managed with a direct percutaneous puncture.
Case presentation
A 65-year-old man with diabetes, dyslipidaemia, heavy smoking history, and chronic limb-threating ischemia (Rutherford V) presented with recurrent ulceration of the left forefoot stump. Angiography showed chronic total occlusion (CTO) of a previously stented SFA. The lesion was crossed and prepared with plain-old balloons (Advance Serenity 5 × 150 mm and 6 × 150 mm, Cook Medical, Bloomington, IN, USA) and a non-compliant balloon (Dorado 7 × 150 mm, BD, Franklin Lakes, NJ, USA) and then relined with two 6 × 170 mm Pulsar-18 T3 stents (Biotronik SE&Co. KG, Berlin, Germany). Post-dilation was performed with the previously used 6-mm hydrophilic-coated over-the-wire balloon. At the end of inflation, the balloon failed to deflate despite repeated attempts with standard measures, including repeated flushing and inflation above the rated burst pressure. The fully expanded balloon obstructed blood flow and could not be withdrawn without risking stent deformation or vascular injury (Fig. 1A). A percutaneous bailout technique was adopted. Under fluoroscopic guidance in a single-plane projection, a 21-gauge, 7-cm microset puncture needle with a transitionless-tip design was advanced through the mid-thigh skin and vessel wall to directly puncture the balloon through the stent struts (Fig. 1B). Subsequently, back “bleeding” (the mix of saline and contrast medium) was observed (Fig. 1C). Passive deflation was insufficient, so aspiration with a 10-cc syringe enabled complete balloon collapse. The catheter was removed intact. Reinflation outside the body confirmed the puncture site without other structural defects (Fig. 2). Final angiography demonstrated no arterial injury or recoil, with restored SFA patency.Fig. 1. During stents post-dilation, upon completion of the inflation phase, the balloon failed to deflate despite repeated attempts using standard techniques. A The balloon catheter results in being undeflatable. B Direct puncture of the balloon catheter through the stent’s struts is performed under X-ray guidance. C: back “bleeding” (saline and contrast medium) is observed. Aspiration through the needle successfully facilitated the deflation of the balloon catheterFig. 2At the end of the procedure, by inflating the balloon catheter, the site of the percutaneous puncture is observed. The rest of the device appeared intact
Discussion
Entrapment or inability to deflate a balloon is exceedingly uncommon, especially in peripheral interventions. In the coronary field, multiple bailout techniques have been described: intentional rupture via overinflation, high tip-load guidewire puncture, cutting the hypotube to restore luminal continuity [3], guide extension-mediated puncture [4], buddy balloon displacement [5], and excimer-laser perforation [6]. In our case, conventional measures were ineffective. Therefore, we opted for the direct puncture technique. The most plausible mechanism of deflation failure was hypotube damage, which prevented pressure transmission to the balloon. Such damage may occur during retrieval and reinsertion or when advancing through stent struts, heavily calcified CTO [7], or tortuous vessels. The presence of stents likely increased the risk of kinking or microperforation of the shaft. This case highlights the importance of careful balloon manipulation, particularly in previously stented vessels, and the need to replace any device showing resistance or suspected structural damage. When balloon deflation failure does occur, direct puncture represents, in percutaneously accessible vessels, a simple, rapid, and reproducible bailout technique.