Bridging ancient wisdom and modern technology: an AI and multi-omics framework for three causes tailored treatment in personalized medicine
Xuewen Diao, Hao Zhang, Shiqi Wang, Qi Zhang, Zulong Wang

TL;DR
This paper proposes combining AI and multi-omics data with traditional Chinese medicine principles to create a personalized, time-sensitive healthcare approach.
Contribution
The novel contribution is integrating the TCTT principle with AI and multi-omics for a dynamic, personalized medicine framework.
Findings
Multi-omics data can quantify individual, temporal, and environmental health dimensions.
AI models can integrate complex interactions across omics, chronomics, and exposome data.
The framework offers a translational roadmap for context-aware clinical decision support.
Abstract
The ‘one-size-fits-all’ therapeutic model is inadequate to address individual patient variability, creating an urgent need for an integrative framework for precision medicine. The ‘Three Causes Tailored Treatment’ (TCTT) principle from traditional Chinese medicine offers a time-tested, holistic blueprint that simultaneously considers the individual, temporal, and environmental dimensions of health. Here, we argue that the synergy of artificial intelligence (AI) and multi-omics technologies is the key to transforming this ancient wisdom into a modern, quantitative clinical paradigm. We demonstrate how multi-omics data provides the foundational layers to quantify the TCTT principle—for instance, using integrated omics (e.g., genomics, proteomics, microbiome) to establish the individual’s molecular baseline (“Who”); chronomics to capture temporal fluxes (“When”); and the exposome to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
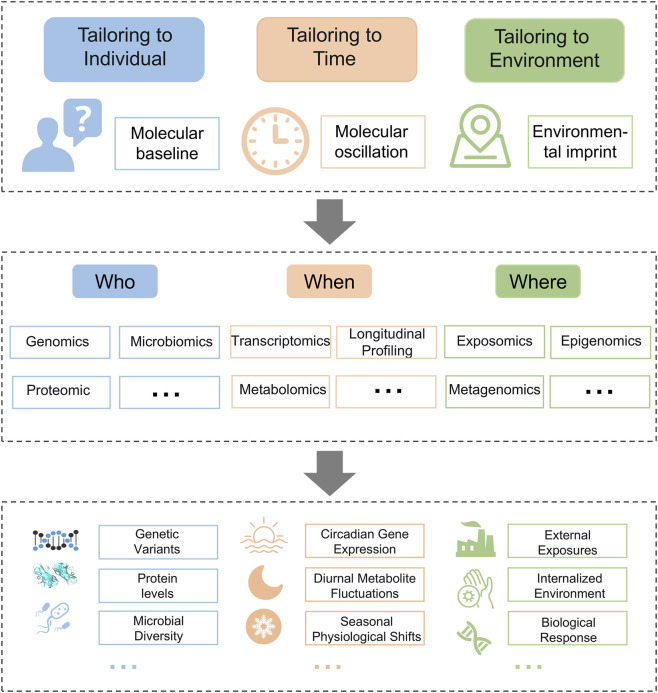 FIGURE 1
FIGURE 1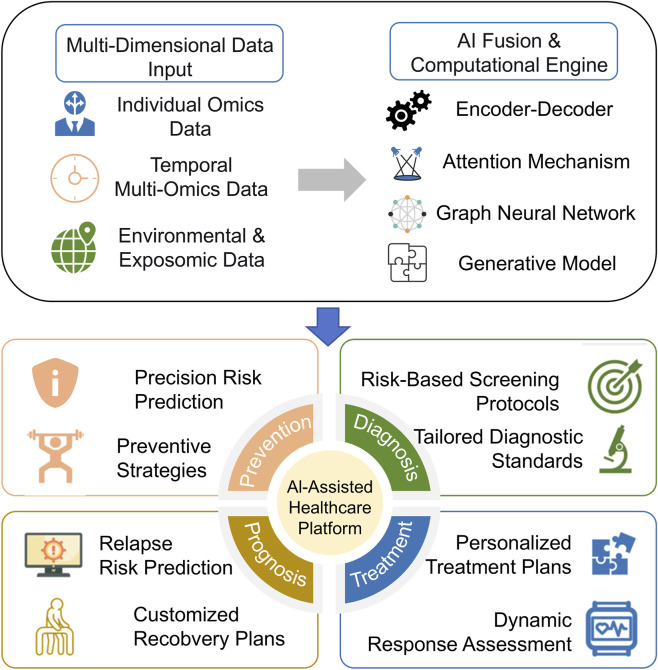 FIGURE 2
FIGURE 2| Data type | Key findings | Application | References |
|---|---|---|---|
| Proteomics | Developed a model to predict the 10-year risk of 218 diseases | Risk assessment and prevention |
|
| cfDNA and proteomics | Achieved high accuracy in early ovarian cancer detection using combined cfDNA and protein biomarkers | Early diagnosis |
|
| Single-cell sequencing | Revealed drug resistance in lung metastasis; explored combination therapy | Optimizing targeted therapy |
|
| Multi-omics | Identified a high-risk subgroup (C1) in t (8; 21) AML patients linked to poor prognosis and lower chemotherapy responsiveness | Prognostic stratification |
|
| Multi-omics | Predicted immune-related adverse events in PD-1/PD-L1 therapy | Enhancing immunotherapy safety |
|
| Data type | Key findings | Application | References |
|---|---|---|---|
| Transcriptomics | Seasonal gene expression changes; winter increases pro-inflammatory markers linked to cardiovascular risks | Seasonal disease risk prediction |
|
| Lipidomics | Diurnal lipid metabolism differences in type 2 diabetes vs. non-diabetic individuals, especially in the morning | Time-sensitive disease diagnosis |
|
| Transcriptomics | Circadian patterns in pancreatic cancer cells reveal potential chronotherapeutic targets | Chronotherapy for pancreatic cancer” |
|
| Single-cell multi-omics | Real-time immune monitoring post-transplant; guides therapy to reduce rejection | Real-time management of transplant patients |
|
| Metabolomics and proteomics | Exercise timing influences multi-tissue metabolome and skeletal muscle proteome; afternoon exercise enhances skeletal muscle lipid and mitochondrial content more than morning exercise | Timing exercise for metabolic health |
|
| Data type | Key findings | Application | References |
|---|---|---|---|
| Expotomics | Serum exposome reveals toxins linked to chronic diseases; region and age are key factors | Predicting disease risks from environmental exposures |
|
| Microbiome and metabolomics | Gut microbiota changes and altered metabolites linked to Kashin-Beck disease severity | High-risk group identification |
|
| Multi-omics | Humidity and heat increase psychiatric emergencies; gut microbiota changes contribute to anxiety | Mental health intervention under environmental stress |
|
| Proteomics | Hypoxia at high altitude affects blood-brain barrier proteins, impacting drug transport | Optimizing drug delivery strategies in hypoxic environments |
|
| Metabolomics | Forest NAI exposure enhances HRV and reduces inflammation, benefiting heart health | Cardiovascular prognosis improvement |
|
| Fusion strategy | Core mechanism | Role in TCTT integration |
|---|---|---|
| Encoder-decoder | Projects multimodal inputs into a latent feature space via an encoder and reconstructs or predicts outcomes via a decoder | Facilitates the construction of cross-scale joint representations by embedding heterogeneous data from the “Three-Factor” framework into a unified semantic space |
| Attention mechanism | Dynamically assigns importance weights to input elements, allowing the model to adaptively attend to the most contextually relevant information | Enables dynamic, context-aware modeling by quantifying the relevance and contribution of each “Three-Factor” component within specific clinical decision-making contexts |
| Graph neural network | Models data as graphs (nodes represent entities, edges represent relations) and learns node embeddings through neighborhood aggregation (message passing) | Explicitly captures the complex interdependencies and interaction networks among the “Individual-Time-Environment” triad |
| Generative model | Learns the underlying joint probability distribution of multimodal data to infer deep, intrinsic cross-modal relationships, thereby supporting robust data fusion and synthesis | Enhances robustness and inferential power in data integration, effectively addressing the prevalent issue of incomplete or missing modalities in real-world clinical settings |
- —National Natural Science Foundation of China10.13039/501100001809
- —Natural Science Foundation of Henan Province10.13039/501100006407
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraditional Chinese Medicine Studies · Health, Environment, Cognitive Aging · Machine Learning in Healthcare
Introduction
1
Adverse drug reactions represent a significant global public health challenge. They underscore the limitations of ‘one-size-fits-all’ therapeutic paradigms and highlight the urgent need for precision solutions that address individual variability (Bouvy et al., 2015; Moyer et al., 2019).
Personalized medicine seeks to meet this need by integrating genetic, environmental, and lifestyle factors (Balistreri et al., 2024). This vision is reflected in global initiatives like the “All of Us” research program and the framework of P4 medicine (Hood and Friend, 2011). However, a core challenge remains: the lack of a cohesive framework to operationalize this multidimensional integration in clinical practice.
This integration challenge finds a powerful parallel in ancient wisdom. The ‘Three Causes Tailored Treatment’ (TCTT) principle from traditional Chinese medicine provides a pre-existing, holistic framework. Rooted in the Huangdi Neijing and refined through millennia of practice, it is a pragmatic system. It posits that effective intervention must account for the patient’s unique constitution (e.g., Yin-Yang balance), circadian and seasonal rhythms, and geographical-living context. This systems-thinking approach shares conceptual ground with other holistic models, such as Ayurvedic Prakriti and modern chronomedicine (Huang et al., 2022; Potter and Wood, 2020).
We argue that TCTT provides the structural blueprint precision medicine needs. However, its clinical application has been limited by a fundamental issue: its core concepts are qualitative. Diagnoses like “Qi deficiency” rely on subjective observation and lack the objective biomarkers required for modern drug development and reproducible trials. This lack of a quantitative basis has prevented its full scientific validation and clinical translation.
This review articulates a novel path to bridge this gap. We propose that artificial intelligence (AI) and multi-omics technologies are pivotal not only in quantifying the TCTT dimensions but, crucially, in modeling their interactions (Gao et al., 2022; He et al., 2023; Mukherji et al., 2024). Evidence for this integration is emerging, from using AI to model TCM diagnostics to applying multi-omics to decode the molecular basis of traditional phenotypes (Kale et al., 2024; Wang, 2025; Wei et al., 2025).
The feasibility of this approach stems from a direct mapping: individual constitution corresponds to a multi-omic baseline (genome, proteome, metabolome, microbiome); temporal dynamics to chronomics; and environmental context to the exposome and its biological response (e.g., in the epigenome and microbiome).
This review is designed for a broad audience of precision medicine researchers, bioinformaticians, and clinical scientists. It aims to examine how AI and multi-omics can be employed to quantify and interconnect the three causes described in TCTT.
Integration of the “three causes tailored treatment” principle in the omics era
2
The TCTT principle offers a structured and holistic framework for personalized medicine. It systematically accounts for an individual’s unique constitution, temporal dynamics, and environmental context. However, a major challenge persists: translating this conceptual framework into a quantitative and clinically actionable paradigm. Here, we define the ‘operationalization’ of TCTT as a process that deconstructs its integrative vision into three discrete, data-driven dimensions. Each dimension addresses a pivotal question in precision medicine. These are: “Who” is being treated (Individual), “When” to intervene (Time), and “Where” the patient is situated in terms of life context (Environment).
Modern omics technologies furnish the data-driven building blocks essential for this operationalization. They deliver high-resolution, molecular-scale measurements, providing the robust evidence needed to objectify and quantify each TCTT dimension. This mapping establishes a clear correspondence:
The ‘Individual’ dimension is operationalized through the comprehensive molecular baseline of a person. This integrates data—from the static genome to the dynamic proteome, metabolome, and microbiome—to answer “Who”. It defines the individual’s unique health status, disease susceptibility, and potential treatment response.
For instance, the multi-omic study by Watanabe et al. demonstrated that such a molecular portrait can move beyond crude clinical metrics like Body Mass Index to precisely define an individual’s unique metabolic health status, identify hidden susceptibilities (e.g., distinguishing metabolically unhealthy individuals within a normal-weight population), and predict their differential responses to lifestyle interventions (Watanabe et al., 2023).
The ‘Time’ dimension is operationalized through temporal multi-omics fluxes (chronomics), capturing rhythmic oscillations (e.g., circadian, seasonal) in molecular profiles. It answers “When” by identifying how biological timing affects health outcomes and therapeutic windows.
As exemplified by a multi-tissue study in mice (Xin et al., 2021), chronomic profiling revealed distinct kinetics in how diurnal transcriptomes and metabolomes in peripheral organs (e.g., liver vs. heart) entrain to inverted feeding schedules. This quantifies how an intervention’s timing is critically linked to its efficacy, providing a molecular basis for chronotherapy.
The ‘Environment’ dimension is operationalized through the internalized environmental imprint, quantified via the exposome and the host’s biological response (e.g., in the epigenome and microbiome). It answers “Where” by decoding how an individual’s specific living context shapes their health trajectory.
A randomized crossover trial on traffic-related air pollution illustrates this approach (Zhang et al., 2022). By integrating personal exposure monitoring with multi-omics profiling, the study quantified how a specific environmental exposure induces systemic inflammation, oxidative stress, and endothelial dysfunction, directly linking a “where” context to molecular and physiological changes.
The following sections will systematically explore this translation based on the above mapping. We will demonstrate how specific omics technologies generate the data types necessary to parameterize these three critical dimensions, thereby illustrating how the TCTT framework bridges a holistic perspective with the measurable data of modern biology. This Figure 1 visually maps how multi-omics provide the quantitative data streams for the Individual, Time, and Environment dimensions, respectively.
Integration of the ‘three causes tailored treatment’ principle with omics technologies.
Omics integration for tailoring to individuals: constructing an individual’s multi-omic portrait across the disease care continuum
2.1
- The “tailoring to individuals” principle originates from the concept that intervention strategies must account for the patient’s unique constitution. Modern omics technologies operationalize this principle by constructing a quantifiable, multi-omic molecular portrait. This portrait integrates the static genome with dynamic, individually distinctive layers, such as the proteome, metabolome, and microbiome. Together, these layers define an individual’s comprehensive molecular baseline. As illustrated in Figure 1, this integrated portrait enables precision medicine across the entire disease care continuum, from prospective risk stratification and early diagnosis to tailored treatment and dynamic prognosis management.
In the phase of risk assessment and prevention, this portrait begins to take shape, focusing on predictive layers. Omics technologies bridge the gap left by traditional population-average strategies by defining individual risk profiles (Merlo et al., 2017; Pastorino et al., 2021). For example, combining plasma proteomics with polygenic genomic analysis significantly refines colorectal cancer risk stratification (Sun et al., 2024), while specific microbiomic profiles serve as biomarkers to identify high-risk individuals, enabling targeted primary prevention (Frey et al., 2018; Ratiner et al., 2024; Zeybel et al., 2022).
For individuals identified as high-risk, early diagnosis critically relies on detecting active signatures in the molecular portrait. Here, omics technologies move beyond traditional screening by capturing real-time molecular signals with superior sensitivity (Olivier et al., 2019). The application of liquid biopsy combined with omics analysis has proven successful in the early detection of cancers such as pancreatic and ovarian cancer by analyzing circulating genomic and proteomic biomarkers (Zhao Y. et al., 2023; Medina et al., 2024), and shows clear advantages in identifying early metabolomic and proteomic signals of neurological and cardiovascular diseases (Dang et al., 2018; Nurmohamed et al., 2022).
Following diagnosis, personalized treatment strategies leverage the functional and mechanistic dimensions of the portrait. This involves decoding how the individual’s unique biology will interact with therapy. Pharmacogenomics predicts drug sensitivity and resistance by analyzing genomic polymorphisms, such as variations in CYP450 genes that influence warfarin metabolism (Dávila-Fajardo et al., 2019; Manceau et al., 2017). In addition, gut microbiomics plays a crucial role in drug metabolism and overall therapeutic response (Kamble et al., 2024; Zhao Q. et al., 2023). Concurrently, emerging synthetic biology approaches demonstrate the potential for precisely engineering microbial systems. For instance, bacterial strains can be engineered for radiation-induced lysis and the local delivery of therapeutic agents, such as immune checkpoint inhibitors (Green et al., 2019; Kamble et al., 2022). Furthermore, technologies such as single-cell and spatial omics reveal heterogeneity in the disease microenvironment, and metabolomic profiling can identify novel therapeutic targets (Fu et al., 2024; Jiang Y. et al., 2024; Liu B. et al., 2024). Collectively, these insights explain distinct drug responses among patients with similar genetic profiles, thereby guiding the development of personalized combination therapies.
Finally, in prognosis management, the individual’s molecular portrait enables refined risk stratification and outcome prediction. The focus shifts to long-term outcome optimization, which is achieved by leveraging the baseline portrait to forecast future trajectories. Multi-omics analysis can identify poor-prognosis subtypes in acute myeloid leukemia by integrating genomic and transcriptomic features (Liu Y. et al., 2024). Radiomics can predict post-surgical recurrence risk in hepatocellular carcinoma by interpreting tumor phenotype (Kang et al., 2023). Integrated proteomic and immunomic profiling can predict adverse events in immunotherapy (Jing et al., 2020). In this phase, the portrait serves as a definitive map for stratifying patients into distinct management pathways.
- Collectively, by sequentially decoding and integrating individual-specific characteristics across this continuous care cycle, omics technologies complete the data-driven loop of personalized care. The resulting multi-omic portrait is not static but evolves with the individual’s health journey, serving as the foundational compass for all clinical decisions. To ground this discussion in contemporary research, Table 1 summarizes selected studies that exemplify the generation and application of multi-omics data under the ‘Tailoring to Individuals’ principle.
Omics integration for tailoring to time: harnessing temporal dynamics for predictive and adaptive care
2.2
The “tailoring to time” principle emphasizes the profound influence of temporal dynamics—from circadian rhythms to seasonal cycles—on health and disease. Modern omics technologies, particularly through the lens of chronomics (temporal multi-omics), operationalize this principle by systematically mapping these biological rhythms. This process converts the abstract concept of time into a quantifiable, molecular data stream (Lincoln et al., 2003). This high-resolution temporal data layer answers the critical question of “When” to intervene, enabling a shift from static to dynamic healthcare across the entire care continuum.
In the realm of prevention, this approach allows for proactive defense aligned with an individual’s biological calendar. Omics analyses can identify individuals with heightened susceptibility to seasonal health threats, such as winter peaks in cardiovascular events, enabling targeted risk mitigation (Dopico et al., 2015; Bhatia et al., 2017). Furthermore, by quantifying the molecular risks of circadian disruption, omics technologies inform the precise timing of interventions (Li Q. et al., 2021). For instance, vaccination schedules or exercise regimens can be personalized to coincide with peaks in immune responsiveness, thereby maximizing their protective efficacy (de Bree et al., 2020; Sato et al., 2022).
For early diagnosis, the temporal dimension refines detection strategies by pinpointing windows of peak molecular signal (Hood and Amir, 2017). The approach moves beyond what to detect to when to detect it. For instance, the metastatic potential of circulating tumor cells peaks during the sleep phase, establishing a temporal window of maximum detectability for liquid biopsy (Diamantopoulou et al., 2022). Similarly, circadian variations in lipid metabolism offer time-specific diagnostic biomarkers for conditions like type 2 diabetes, pointing to optimal morning hours for screening (Sinturel et al., 2023).
The principle finds one of its most direct applications in chronotherapy, where treatment timing is synchronized with biological rhythms to maximize efficacy and minimize toxicity (Plasqui et al., 2003; Tsuruta et al., 2022). Omics data provide the molecular rationale for this synchronization. For example, circadian transcriptomics in cancer is being used to identify temporal windows that improve the efficacy of immunotherapy while reducing side effects (Fang et al., 2015; Sharma et al., 2024). This extends to seasonal rhythms. Omics can illuminate the underlying physiological shifts that occur with the seasons, revealing when therapies need dynamic adjustment. A key example is modifying anticoagulant dosing during seasons when drug clearance is reduced (Lee et al., 2014). Looking forward, the temporal dimension will be equally critical for guiding next-generation therapies. Emerging research, including the use of engineered probiotics for time-specific, epitope-independent radionuclide therapy or for stromal remodeling to enhance immunotherapy, underscores the potential to build temporal control directly into the therapeutic mechanism itself (Siddiqui et al., 2023; Thomas et al., 2022).
Finally, in prognosis management, real-time multi-omics monitoring creates a closed-loop system for adaptive care. The integration of wearable devices with serial molecular profiling generates a continuous stream of time-stamped data, enabling preemptive interventions (Braig, 2022). For example, in organ transplant recipients, single-cell multi-omics can track immune recovery in real-time, guiding precise therapy adjustments (Wang et al., 2024). Similarly, in cancer rehabilitation, longitudinal serum proteome and metabolome profiling allows clinicians to fine-tune nutritional and lifestyle interventions (Braun and Harris, 1983; Li X. et al., 2021). Critically, this dynamic data stream enables chronotherapeutic optimization, such as timing exercise to align with a patient’s daily physiological rhythms to maximize metabolic benefits (Savikj et al., 2022).
This transforms clinical practice from a series of episodic, static decisions into a dynamic, predictive, and adaptive process. This new paradigm respects the intrinsic temporal architecture of health and disease, and will be essential for managing novel and dynamic therapies, such as engineered microbial agents. Table 2 summarizes selected studies that exemplify the generation and application of multi-omics data under the ‘Tailoring to Time’ principle.
Omics integration for tailoring to environment: decoding the biological imprint of context for precision health
2.3
The “tailoring to environment” principle posits that health cannot be understood in isolation from an individual’s geographic, climatic, and lifestyle context. Modern omics technologies put this principle into practice. They do this by systematically reading the biological signals left by environmental exposures, using fields like exposomics and environment-responsive molecular profiling. This profiling turns a person’s surroundings into a quantifiable data layer. This data answers the critical “Where” question of their life context. In doing so, it establishes the final pillar needed for a fully integrated TCTT model.
In risk assessment, this approach moves beyond static genetics to deliver a dynamic, context-aware risk profile. Multi-omics analyses quantify the interplay between genetic susceptibility and environmental exposure. For instance, the integration of geographic exposure mapping, personal sensor data, and multi-omics analysis enables a highly granular understanding of individual risk in inflammatory bowel disease (Agrawal et al., 2022). Similarly, multi-omics approaches can identify and predict cardiovascular risks associated with pollutants, noise, and light exposure, facilitating targeted preventive interventions (Riggs et al., 2018).
For early screening, the focus shifts to the pre-symptomatic detection of environmental and occupational illnesses. This strategy maps the continuum from exposure to preclinical molecular change. In endemic Kashin-Beck disease, exposomics monitoring of regional soil and water, combined with proteomic and metabolomic profiling of individuals, constructs a regional risk atlas for early intervention (Wang et al., 2021). Similarly, for pneumoconiosis, exposomics of workplace dust combined with metabolomic and transcriptomic analysis establishes a molecular signature of early-stage lung injury, enabling action before irreversible damage occurs (Huang et al., 2018; Chen et al., 2022).
Critically, this principle extends to treatment optimization, where omics decode how specific environments alter physiology to guide therapy personalization. For example, omics analyses reveal that high-temperature, humid environments can induce anxiety-like disorders. This effect is mediated through gut microbiota dysbiosis and subsequent metabolic alterations, a discovery that opens avenues for microbiota-targeted interventions (Weng et al., 2024). Similarly, in high-altitude hypoxic environments, omics insights into hypoxia-induced changes in blood-brain barrier protein expression provide a mechanistic basis for devising altitude-adjusted drug administration protocols (Liu G. et al., 2024).
Finally, in prognosis management, the environment itself can be leveraged as a therapeutic modality. Multi-omics data provides the mechanistic basis for prescriptive environmental recommendations (Liu et al., 2023). Exposure to forest environments has been shown to improve cardiopulmonary function, while specific altitude climates can enhance recovery for asthma and coronary heart disease patients (Fieten et al., 2022; Liu et al., 2022; Yan et al., 2024). Furthermore, omics-based analyses elucidate how moderate ultraviolet exposure regulates immune function in autoimmune conditions, enabling the optimization of exposure (Milliken et al., 2012).
In summary, omics technologies quantify how a person’s surroundings affect their biology. This includes harmful exposures and beneficial environments. By adding this dimension, omics complete the integrative vision of TCTT. This empowers a form of precision medicine that is not only personal and timely but also profoundly context-aware, ensuring interventions are optimally tailored to the specific environments in which people live and heal. Table 3 summarizes selected studies that exemplify the generation and application of multi-omics data under the ‘Tailoring to Environment’ principle.
AI and multimodal models: the computational engine for integrating the three causes tailored treatment
3
The quantification of the TCTT framework through multi-omics provides the essential data-driven building blocks. However, turning this data into an integrated health model is challenging (Mirza et al., 2019; Saliba et al., 2024). The data types are diverse, ranging from static genomes to dynamic environmental exposures. Furthermore, the interactions between an individual’s biology, temporal rhythms, and environment are complex and nonlinear. Finally, the high-dimensionality of omics data often exceeds the size of typical research cohorts. These characteristics present formidable obstacles for traditional statistical methods. In this context, AI, particularly through multimodal learning, emerges as a powerful computational engine for this integration task, offering a viable path to transform the TCTT framework from a qualitative principle into a quantitative, actionable model (Shao et al., 2023).
Multimodal AI models for three causes tailored treatment
3.1
Integrating high-dimensional and heterogeneous “Three-Cause” data demands computational approaches capable of effectively modeling nonlinear relationships and complex interactions, a task that extends beyond the scope of traditional statistical methods. Multimodal artificial intelligence thus serves as the core computational engine for operationalizing the TCTT framework. This section focuses on four key technical architectures that drive multimodal integration: the attention mechanism, graph neural networks, generative models, and encoder-decoder structures (Zhao et al., 2024). The roles of these key AI architectures are summarized in Table 4.
Cutting-edge research increasingly demonstrates the power of these computational engines to integrate the core dimensions of the TCTT framework.
For instance, an encoder-decoder framework can fuse static individual characteristics with dynamic longitudinal imaging data, thereby jointly modeling the ‘Individual’ and ‘Time’ dimensions within a unified latent space (Gao et al., 2024). This approach enables the dynamic prediction of a patient’s treatment response, moving beyond static assessments. Complementing this, Transformer architectures utilize attention mechanisms to integrate complex multi-omics data. By dynamically weighting the contribution of distinct genomic elements, these models sharpen risk prediction at the ‘Individual’ level, effectively identifying the most salient molecular signals within a high-dimensional dataset (Zhou et al., 2025). Spatial analyses further showcase this integration. Bai et al. employed graph neural networks to explicitly model the interplay between the tumor spatial microenvironment and the host’s molecular characteristics, which form the ‘Individual’ basis of the disease (Bai et al., 2025). Similarly, the generative model soScope enhances data resolution by coherently merging spatial localization (Environment) with molecular profiles (Individual), demonstrating how generative AI can resolve multi-scale biological complexity (Li B. et al., 2024).
In practice, these engines achieve their fullest potential synergistically. A leading example is a high-resolution exposome mapping framework that combines an encoder-decoder structure with an attention mechanism. This integrated strategy successfully fuses multi-source data corresponding directly to the complete ‘individual-time-environment’ triad, providing a powerful blueprint for computational TCTT integration (Luan and Daoyu, 2025).
Towards three causes tailored treatment-informed AI platform: a conceptual framework
3.2
With the widespread adoption of AI in healthcare, AI-assisted platforms are becoming a cornerstone of personalized medicine. Existing platforms, such as IBM Watson Health and Google DeepMind, have demonstrated remarkable potential in areas like medical imaging and diagnostic assistance (Ting et al., 2019; Park et al., 2023). However, these platforms often focus on specific data types or limited clinical applications. To fully realize the vision of the TCTT, we envision a next-generation, comprehensive AI-driven healthcare platform. This conceptual framework, as depicted in Figure 2, is built upon multimodal AI models and omics data, designed to integrate diverse data sources—including genomic, clinical, environmental, and temporal information—to deliver dynamic, context-aware health management.
A conceptual framework for three causes tailored treatment-informed precision medicine.
The proposed framework comprises four key functional modules. Risk Prediction: This module would analyze genetic predispositions (Individual), environmental risk factors (Environment), and seasonal patterns (Time) to offer comprehensive health assessments. For example, integrating omics data with lifestyle information could identify individuals at high risk for diabetes, providing actionable recommendations on diet and exercise that are tailored to their specific circumstances and time of year (Carletti et al., 2025).
Intelligent Diagnosis: Multimodal AI models within this module could enhance diagnostic precision by analyzing diverse datasets. Multimodal models have shown efficacy in evaluating diseases like cancer and Parkinson’s disease, empowering personalized screening strategies for high-risk populations and enabling early interventions (You J. et al., 2024; Liang et al., 2024).
In personalized treatment, multimodal models integrate patient data to predict therapeutic responses and identify optimal treatment regimens. For instance, multimodal analyses have been applied in gastric cancer to predict responses to anti-HER2 therapy and select the most effective treatment plans (Chen et al., 2024). Furthermore, machine learning models might predict circadian time to optimize the timing of drug administration, thereby maximizing efficacy and minimizing toxicity (Hesse et al., 2020).
Prognosis Management: This module envisions closing the loop on continuous, adaptive care by actively managing an individual’s recovery within their environmental context. It would evaluate recurrence risks and tailor follow-up plans by integrating clinical data, omics profiles, and real-time data from wearable devices. For instance, multimodal models can stratify cardiovascular patients into risk groups, allowing for tailored rehabilitation plans that consider environmental factors like air quality and seasonal changes (Castronuovo et al., 2023). This approach is supported by research using multimodal models to stratify patients into risk groups for tailored recurrence management (Jiang Y. Z. et al., 2024).
The synergistic potential of this conceptual framework can be illustrated by envisioning a response to a complex clinical challenge, such as treatment-resistant hypertension. In a future implementation, the platform could first assess a patient’s risk by hypothetically integrating her polygenic score with a gut microbiome signature indicative of impaired bile acid metabolism (Individual) (Xu et al., 2025). If conventional treatment failed, the platform might then analyze longitudinal metabolomic data (Time) to explore whether blood pressure spikes correlate with precursor metabolites, potentially leading to a recommendation for a mechanism-targeted therapy like a bile acid sequestrant. Finally, by incorporating real-time air quality data (Environment), it could generate personalized advice to mitigate environmental risks. This conceptual application demonstrates the TCTT-AI framework’s potential to move beyond siloed data analysis.
It is important to note that the realization of such an integrated platform faces significant challenges, including the technical hurdles of multimodal data fusion, data privacy, standardization, and clinical integration. This conceptual framework thus serves not as a description of an existing tool, but as a roadmap for future research and development, outlining how the TCTT principle can be systematically operationalized through AI to advance precision medicine.
Challenges and future outlook
4
The path toward translating the TCTT-informed precision medicine vision into clinical practice is promising yet fraught with multifaceted challenges that span technical, clinical, and socio-ethical domains. While the TCTT framework provides a compelling integrative structure, each of its pillars—individual, time, and environment—faces unique and significant barriers to operationalization that extend beyond the general challenges of precision medicine. Thoughtfully addressing these hurdles is paramount for the framework’s successful integration into mainstream healthcare.
Technical bottlenecks in data integration and modeling
4.1
The operationalization of the TCTT framework is primarily hampered by significant technical hurdles. The integration of highly heterogeneous and high-dimensional data across its three core dimensions (individual, time, and environment) presents a formidable obstacle for model development and validation (Jurisica, 2024).
The “Individual” Dimension: Constructing a dynamic multi-omic portrait is not merely a data aggregation exercise. A major limitation is our incomplete understanding of how to distinguish causal drivers of disease from incidental correlations within these vast datasets (Schadt, 2009). For instance, while we can identify microbial signatures associated with disease, determining whether they are a cause or a consequence remains a challenge, complicating targeted interventions.
The “Time” Dimension: Capturing temporal dynamics through chronomics is resource-intensive and analytically complex. Longitudinal sampling at the required frequency (e.g., hourly for circadian rhythms) is impractical for large cohorts and poses a significant patient burden (Price et al., 2017). Furthermore, deconvoluting the effects of aging, disease progression, and reversible rhythmic changes presents a monumental modeling task.
The “Environment” Dimension: Quantifying the exposome is arguably the most nascent pillar. Many environmental exposures are episodic, poorly measured, and interact in complex ways. Current tools often fail to capture the full breadth and personal nature of environmental exposures, from chemical mixtures to psychosocial stressors, limiting the accuracy of this data layer (Wild, 2012).
This “curse of dimensionality” is exacerbated by the relatively small cohort sizes in most current multi-omics studies, increasing the risk of overfitting. Furthermore, the “black-box” nature of many sophisticated AI models raises critical concerns regarding interpretability (Rudin, 2019). For clinicians to trust and act upon AI-generated recommendations, they require understandable rationales. Future efforts must prioritize the development of explainable AI techniques that can elucidate why a specific personalized intervention was recommended, for example, by highlighting that a dosage adjustment was driven 60% by the patient’s pharmacogenomic profile (‘Individual’), 30% by their circadian phase (‘Time’), and 10% by local air quality data (‘Environment').
Data privacy, infrastructure, and standardization
4.2
Beyond technical barriers, the framework’s reliance on aggregating sensitive multimodal data inevitably raises profound concerns about patient privacy and data security (Sung, 2023). The implementation of privacy-preserving techniques like federated learning offers a promising path (Li H. et al., 2024). Concurrently, the lack of standardized protocols for data collection across diverse omics platforms and environmental exposures creates significant interoperability issues. This is particularly acute for TCTT, which requires harmonizing data standards across traditionally separate fields—from genomic sequencing to environmental sensor networks. Establishing international consortia and harmonized ethical-regulatory frameworks is imperative to promote data sharing and build the large-scale, diverse datasets needed to train robust and generalizable models.
Clinical translation and validation hurdles
4.3
A critical gap lies in proving the clinical utility and cost-effectiveness of this complex approach.
Lack of Trial Evidence: To date, there are no large-scale, prospective clinical trials that simultaneously test interventions tailored to all three TCTT dimensions. The vast combinatorial space of possible “Individual-Time-Environment” interventions makes traditional randomized controlled trials (RCTs) financially and logistically prohibitive.
Novel Trial Designs: Designing trials capable of validating such a dynamic approach is exceptionally difficult (Krassowski et al., 2020). Novel designs, such as adaptive platform trials, N-of-1 series, or “microrandomized” trials, are needed to generate the requisite evidence base.
The Cost-Benefit Question: A stark, unresolved challenge is the overwhelming cost of comprehensive multi-omics profiling and continuous monitoring. The healthcare economics of this approach are unproven, creating a high risk of exacerbating the “biomedical divide,” where such advanced care is only accessible to the affluent (Joyner and Paneth, 2015).
Workflow Integration: Moreover, integrating such a platform into existing clinical workflows poses significant practical challenges. A poorly designed user interface could increase, rather than reduce, the cognitive load on clinicians, hindering adoption (Adams and Petersen, 2016).
Ethical equitability and algorithmic bias
4.4
The vision of TCTT-informed precision medicine also introduces pressing ethical considerations. There is a critical risk that AI models could perpetuate or even amplify existing health disparities if they are trained on non-representative datasets primarily from affluent populations, leading to biased and suboptimal outcomes for underrepresented groups (Yang et al., 2024). Proactive measures, such as auditing algorithms for bias and purposefully curating diverse training datasets, are essential to ensure that the benefits of personalized medicine are distributed equitably. Furthermore, the potential for “digital phenotyping” and environmental monitoring to intrude on personal autonomy and lifestyle choices necessitates careful ethical scrutiny and robust informed consent processes. Additionally, the significant costs associated with multi-omics profiling and continuous monitoring raise concerns about economic equity and the potential creation of a “biomedical divide.”
Looking forward: a concerted multi-domain roadmap
4.5
Overcoming these hurdles requires a concerted, multi-stakeholder effort. Technological innovation must focus on developing robust, interpretable, and privacy-aware multimodal fusion models. A critical first step is to run pilot studies demonstrating proof-of-concept for individual TCTT dimensions, such as a trial showing that time-of-day-specific dosing (Time) improves outcomes in a genetically stratified (Individual) subgroup. Clinicians, researchers, TCM experts, and regulators must collaborate to establish new standards for data, evidence generation, and the bio-digital translation of traditional concepts. Ethicists and policymakers must work alongside technologists to create governance frameworks that safeguard against bias, protect individual rights, and promote equitable access. By viewing these challenges not as insurmountable barriers but as defined research and implementation priorities, the field can systematically build the technical, ethical, and collaborative foundations needed to realize the full potential of TCTT-driven precision medicine, ultimately delivering on the promise of healthcare that is truly personal, predictive, and participatory.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams S. A. Petersen C. (2016). Precision medicine: opportunities, possibilities, and challenges for patients and providers. J. Am. Med. Inf. Assoc. JAMIA 23, 787–790. 10.1093/jamia/ocv 215 26977101 PMC 9396673 · doi ↗ · pubmed ↗
- 2Agrawal M. Allin K. H. Petralia F. Colombel J. F. Jess T. (2022). Multiomics to elucidate inflammatory bowel disease risk factors and pathways. Nat. Reviews. Gastroenterology and Hepatology 19, 399–409. 10.1038/s 41575-022-00593-y 35301463 PMC 9214275 · doi ↗ · pubmed ↗
- 3Bai Z. Osman M. Brendel M. Tangen C. M. Flaig T. W. Thompson I. M. (2025). Predicting response to neoadjuvant chemotherapy in muscle-invasive bladder cancer via interpretable multimodal deep learning. NPJ Digital Medicine 8, 174. 10.1038/s 41746-025-01560-y 40121304 PMC 11929913 · doi ↗ · pubmed ↗
- 4Balistreri C. R. Vinciguerra C. Magro D. Di Stefano V. Monastero R. (2024). Towards personalized management of myasthenia gravis phenotypes: from the role of multi-omics to the emerging biomarkers and therapeutic targets. Autoimmun. Reviews 23, 103669. 10.1016/j.autrev.2024.103669 39426579 · doi ↗ · pubmed ↗
- 5Bhatia S. Bhatia S. Mears J. Dibu G. Deshmukh A. (2017). Seasonal periodicity of ischemic heart disease and heart failure. Heart Fail Clin. 13, 681–689. 10.1016/j.hfc.2017.05.004 28865777 · doi ↗ · pubmed ↗
- 6Bouvy J. C. De Bruin M. L. Koopmanschap M. A. (2015). Epidemiology of adverse drug reactions in Europe: a review of recent observational studies. Drug Safety 38, 437–453. 10.1007/s 40264-015-0281-0 25822400 PMC 4412588 · doi ↗ · pubmed ↗
- 7Braig Z. V. (2022). Personalized medicine: from diagnostic to adaptive. Biomed. J. 45, 132–142. 10.1016/j.bj.2019.05.004 35590431 PMC 9133264 · doi ↗ · pubmed ↗
- 8Braun D. P. Harris J. E. (1983). Serial immune function testing to predict clinical disease relapse in patients with solid tumors. Cancer Immunol. Immunother. 15, 165–171. 10.1007/BF 00199159 6352007 PMC 11039147 · doi ↗ · pubmed ↗