Acne in adulthood: A cross-sectional study of contributing hormonal, dietary, and environmental factors in adults in Puerto Rico
Itzamar Pastrana Echevarria, Alicia Báez Cruz, Alejandra Figueroa Moreda, Fabian Ramírez Rivera, Lymarie Aguila Gonzalez

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
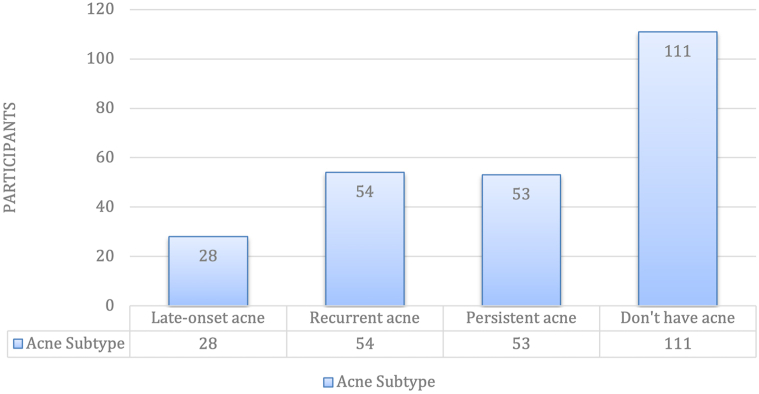 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcne and Rosacea Treatments and Effects · Traditional Chinese Medicine Studies · Contact Dermatitis and Allergies
To the Editor: Acne Vulgaris ranks eighth in disease prevalence, affecting 9.4% of the population.1 Although commonly triggered during adolescence, it can occur at any age.2 In the United States, adult acne incidence is rising, affecting up to 15% of women.2 While adolescent males are more commonly affected, this trend reverses in adulthood, with 26% of women and 12% of men reporting acne in their 40s.3
Various factors have been implicated in adult acne, including hormonal, dietary, hygiene-related, stress, sleep and environmental influences. Although no definitive cause has been established, this study assessed their association in the Puerto Rican population, where unique behavioral and contextual factors may differ from the mainland United States.
An anonymous 22-item REDCap survey was distributed via social media and in a dermatology clinic in Manatí, Puerto Rico through promotional flyers with a QR code between April and July 2025. This IRB approved cross-sectional study used a convenience sampling method. A total of 328 surveys were initiated and 298 were completed, yielding a response rate of 90.9%. After applying inclusion criteria, 246 participants were included in the final analysis. Adult acne was defined as onset at ≥ 25 years of age.
As participation was voluntary and the survey title referenced acne, individuals with acne may have been more inclined to respond, introducing potential selection and response bias. Descriptive statistics were used to summarize demographic and clinical variables. Associations between categorical variables were evaluated using chi-square test, with significance set at P < .05. Analyses were performed using IBM SPSS Statistics.
Of the 246 participants: 172 with self-reported adult acne and 126 without. All participants self-identified as Hispanic. The overall sample was predominantly female (72%); however, the proportion of males who reported acne (60.9%) was higher than that of females (52.5%), diverging from U.S. trends (Fig 1). Most cases occurred between ages 25-34 years. Persistent (21.5%) and recurrent (22%) acne subtypes were most common. Notably, 74% of participants had never consulted a dermatologist, suggesting underrecognition or access barriers to care.Fig 1. Prevalence of adult acne subtypes (n = 246). Recurrent (n = 54) and persistent (n = 53) were the most common subtypes, followed by late-onset acne (n = 28). A total of 111 participants reported not having acne.
Poor sleep quality was significantly associated with adult acne (P = .019), aligning with current literature.4 Inconsistent makeup removal also correlated with acne (P = .04), reinforcing clinical recommendations for proper skincare although no specific studies have evaluated a direct association between adult acne and not removing makeup at the end of the day.5 Use of non-comedogenic products showed a borderline association (P = .051), possibly reflecting reverse causality, though it remains advisable to avoid oil-based, pore-clogging products. Additionally, refined carbohydrates and dairy intake showed positive but non-significant trends, supporting hypotheses on diet-acne links. Moreover, environmental factors may contribute with nearly 30% reported flares during summer, aligning with data from tropical regions.
Future research using dermatologist confirmed diagnoses and prospective data could improve accuracy. This study offers novel insights into adult acne in Puerto Rico, emphasizing male prevalence, hormonal patterns, and lifestyle factors. These findings support culturally tailored approaches to acne care (Table I).Table IAssociation between stress level, sleep quality, and adult acne presence (n = 246)Variables (n)Acne developmentP-valueYes (n = 135)No (n = 111)Non-comedogenic skin care Didn’t know the existence (55)25 (45.5%)30 (54.5%).051 Don’t’ pay attention (61)28 (45.9%)33 (54.0%) Only when I see breakouts (24)16 (66.7%)8 (33.3%) Always use (106)66 (62.3%)40 (37.7%)Removal of makeup before sleep Doesn’t apply (55)21 (38.2%)34 (61.8%).04 Don’t use makeup (23)13 (56.5%)10 (43.5%) Sometimes (18)13 (72.2%)5 (27.8%) Generally, no (1)1 (100%)0 (0%) Yes, always (149)87 (58.4%)62 (41.6%)Bed pillow cover changing Don’t change them (12)6 (50%)6 (50%).912 2 times a month (27)16 (59.3%)11 (40.7%) Once a month (60)33 (55%)27 (45%) Once a week (121)64 (52.9%)57 (47.1%) Several times a week (26)16 (61.5%)10 (38.5%)Frequency of face-towel change Don’t change them (12)6 (50%)6 (50%).982 Once a month (24)13 9 (54.2%)11 (45.8%) Once a week (137)75 (54.7%)62 (45.5%) Several times a week (73)41 (56.2%)32 (43.8%)Using the same towel for body & face Use the same towel (141)38 (57.6%)28 (42.4%).822 Use them separately (66)75 (53.2%)66 (46.8%) Try to use them separately (39)22 (56.4%)17 (43.6%)Cleaning cellphone screen Rarely (48)30 (62.5%)18 (37.5%).312 When visibly dirty (87)51 (58.6%)36 (41.4%) Once a day (60)28 (46.7%)32 (53.3%) Multiple times a week (51)26 (51%)25 (49%)Frequency of facial washing a day Don’t do it often (10)2 (20%)8 (80%).074 When I need it (41)18 (43.9%)23 (56.1%) More than 2 times (22)14 (63.6%)8 (36.4%) Morning and when going to bed (115)68 (59.1%)47 (40.9%) Only in morning or night (58)33 (56.9%)25 (45.1%)Stress level Low (15)8 (53.3%)7 (46.7%).071 Moderate (137)67 (48.9%)70 (51.1%) High (94)60 (63.8%)34 (36.2%)Sleep quality Bad (51)36 (70.6%)15 (29.4%).019 Moderate (130)70 (53.8%)60 (46.2%)Chi-square analysis examining the relationship between perceived stress levels and sleep quality with adult acne presence. Values are shown as number of participants with acne (%). P = values < .05 were considered statistically significant.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tan J.K.Bhate K.A global perspective on the epidemiology of acne Br J Dermatol 172Suppl 1201531210.1111/bjd.1346225597339 · doi ↗ · pubmed ↗
- 2American Academy of Dermatology Skin conditions by the numbers [Internet]. Rosemont (IL): American Academy of Dermatologyhttps://www.aad.org/media/stats-numbers 2024
- 3Zaenglein A.L.Acne vulgaris N Engl J Med 3791420181343135210.1056/NEJ Mcp 170249330281982 · doi ↗ · pubmed ↗
- 4Putri W.E.Hilda N.F.Kusumah F.R.The relationship between fast food, sleep patterns, and facial hygiene with the severity of Acne vulgaris Biomol Health Sci J 722024889510.4103/bhsj.bhsj_3_24 · doi ↗
- 5American Academy of Dermatology. I have acne! is it okay to wear makeup? [Internet]. Rosemont (IL): American Academy of Dermatology Associationhttps://www.aad.org/public/diseases/acne/causes/makeup 2023