Targeted 19F MRI for molecular imaging of the immune response and its theranostics
Pascal Bouvain, Sebastian Temme, Ulrich Flögel

TL;DR
This review discusses how 19F MRI can be used to visualize and treat inflammation, focusing on its potential for diagnosing and managing diseases like colitis.
Contribution
The paper highlights recent advances in using fluorine-based MRI for targeted theranostic applications, particularly in manipulating immune responses.
Findings
19F MRI allows for the detection of inflammation with minimal background signal.
Recent strategies using 19F MRI have shown significant improvements in treating acute colitis by manipulating neutrophils.
The integration of diagnosis and therapy through 19F MRI is promising for various disease models.
Abstract
The in vivo visualization of inflammatory processes offers not only the possibility of localizing disease but also of monitoring its progression over time. Among available imaging modalities, combined 1H/19F MRI has emerged as a powerful technique, as it enables the detection of inflammation with minimal background signal. Beyond diagnosis, however, there is increasing interest in using this platform to initiate targeted therapeutic interventions. The integration of these two components—diagnosis and therapy—is commonly referred to as theranostics. In this review, we provide an overview of the potential of fluorine-based MRI and highlight a range of targeted theranostic applications across different disease models. Particular emphasis is placed on recent strategies to manipulate neutrophils during acute colitis, which have demonstrated significant improvements in disease outcome.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
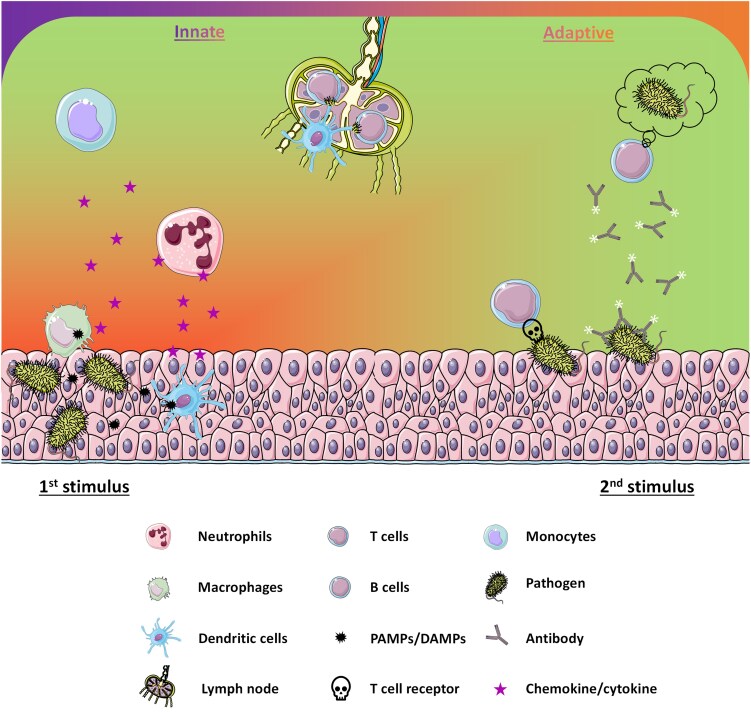 Figure 1
Figure 1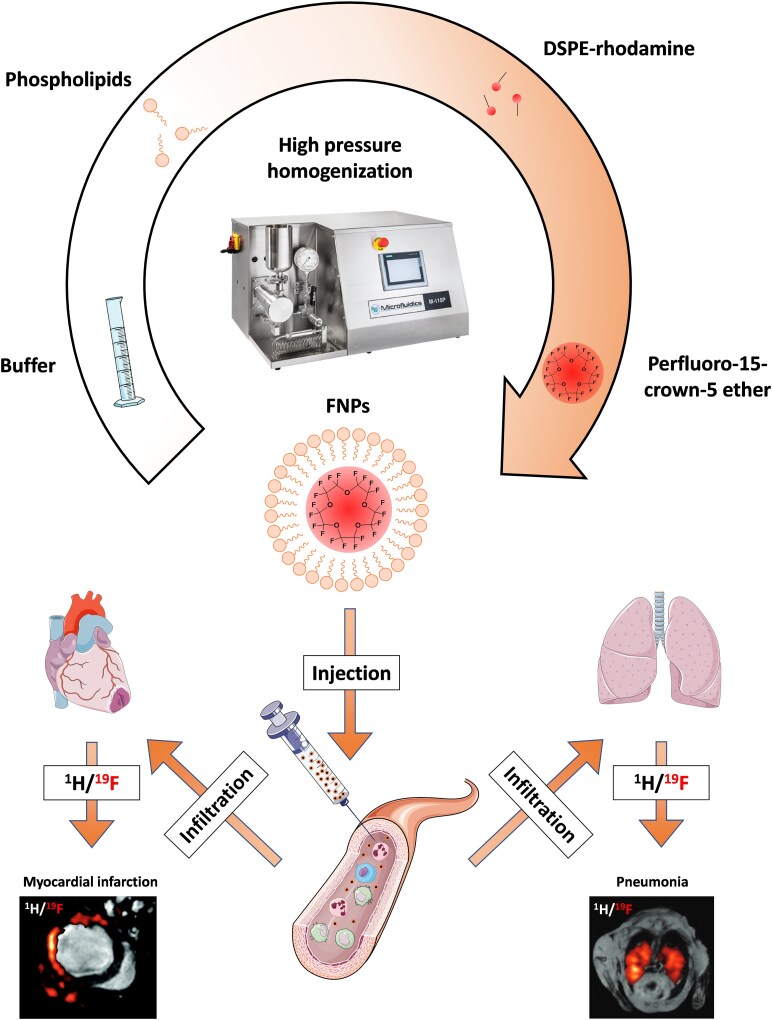 Figure 2
Figure 2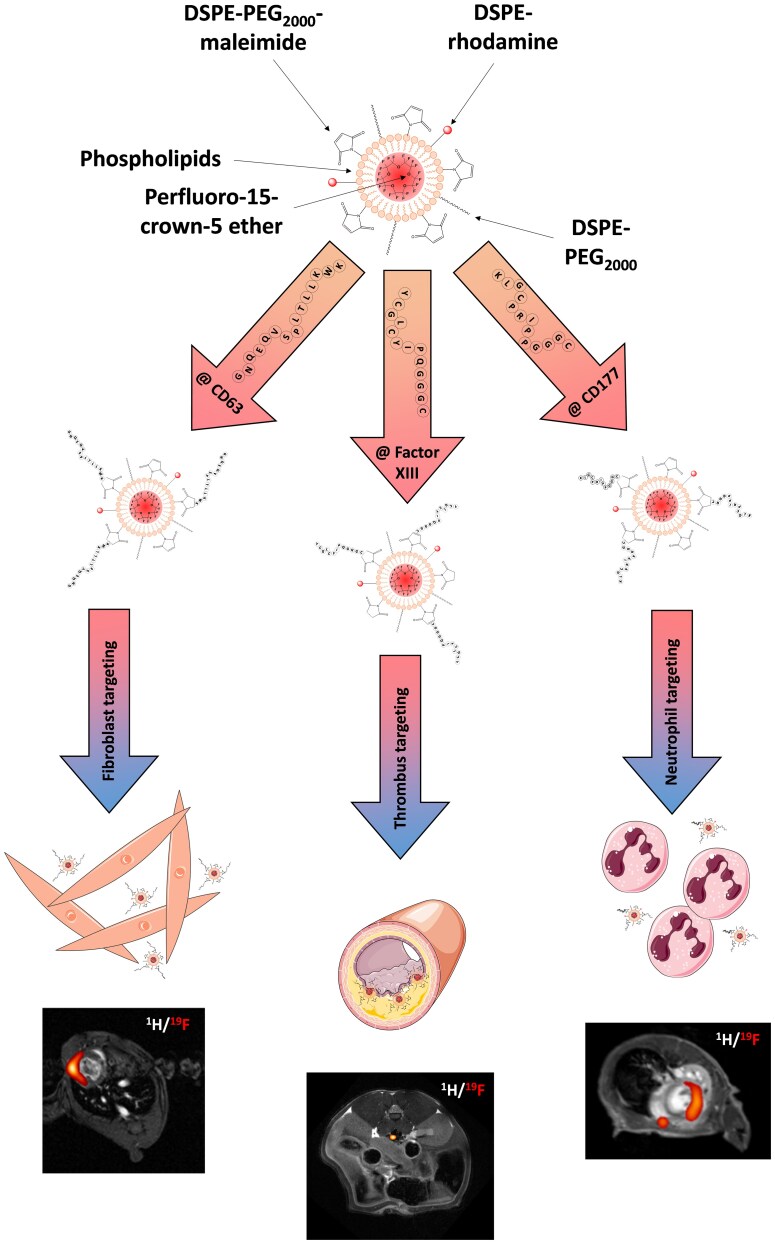 Figure 3
Figure 3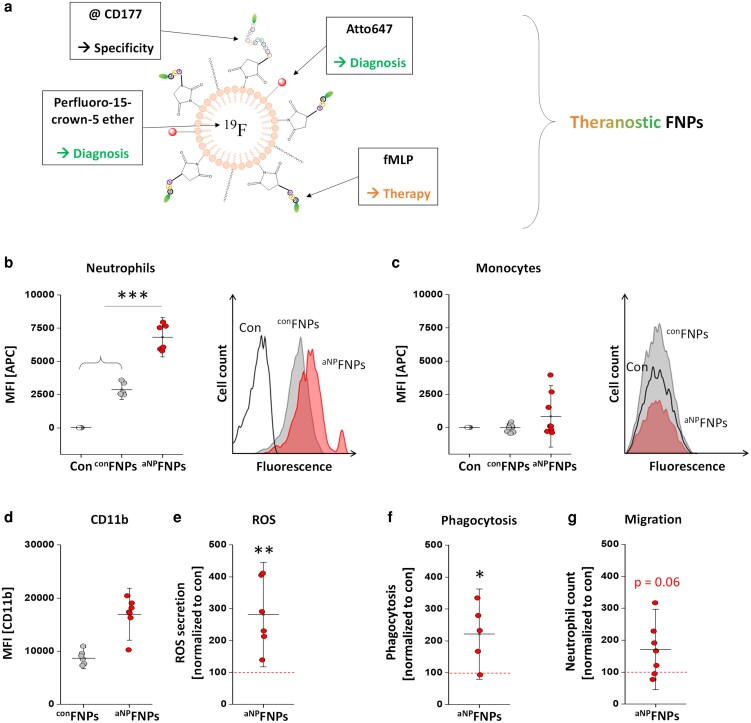 Figure 4
Figure 4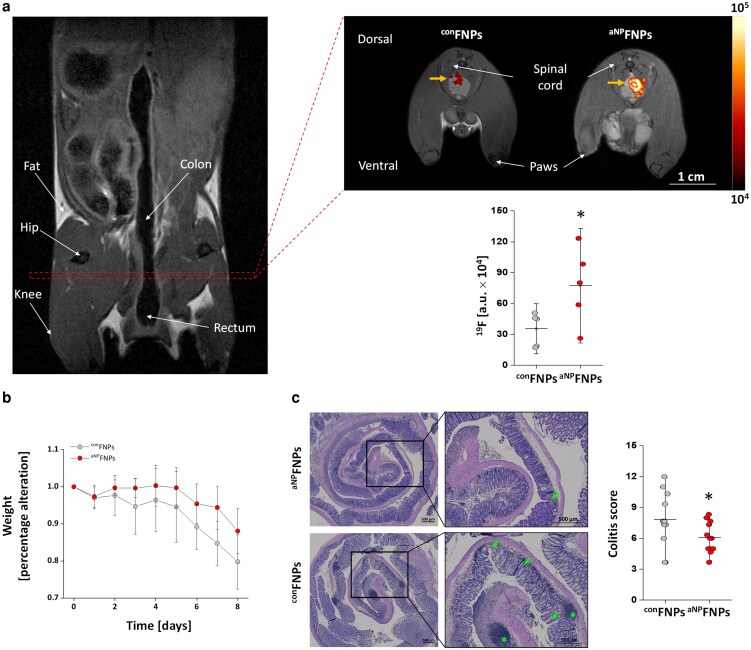 Figure 5
Figure 5| MR contrast | Target | Ligand | Therapeutic drug/therapy | Disease | Brief summary | Reference |
|---|---|---|---|---|---|---|
| IO-NPs | GLUT | Glucuronic acid | Iron oxide (hyperthermia) | Cancer | IO-NPs were functionalized with glucuronic acid (NPs@GlcA) to target glucose transporters (GLUT) expressed on brain endothelial cells and glioblastoma. Systemic administration of NPs@GlcA resulted in transcytosis | Caro |
| IO-NPs | Tumor | Cancer cell membrane (homotypic targeting) | Lycorine hydrochloride | Cancer | IO-NPs enwrapped by HT29 cell membrane and loaded with lycorine hydrochloride reduced growth of HT29 colorectal cancer in mice. | Li |
| IO-NPs | P-Selectin | Fucoidan | Fucoidan | Cancer | Fucoidan coated IO-NPs target P-selectin on the lung cancer cell line A549 leading to higher ROS-production, increased cytotoxicity and less migration/invasion | Ho |
| IO-NPs | PDGFR | PDGF | Glucose oxidase/FePt | Cancer | Nanoliposomes targeted against platelet-derived growth factor receptor (PDGFR) that contain IO-NPs, glucose oxidase and platinum increased ROS production and induced apoptosis/ferroptosis. Treatment of mice with a breast cancer xenograft (MDA-MB-231) reduced tumor size. | Zhang |
| IO-NPs | Sialic acid | Phenylboronic acid | Phototherapy | Cancer | Targeting of sialic acid on tumor cells with IO-NP-containing particles that led to enhanced photothermal response and strongly reduced tumor volume (ovarian cancer) in mice. | Lu |
| IO-NPs | αvβ3-Integrin | RGD peptide | Doxorubicin/indocyanine green | Cancer | IO-NPs functionalized with RGD to target αvβ3-integrin on U87MG tumor cells and doxorubicin/indocyanine green for enhanced photothermal and chemotherapy that strongly reduced tumor size in mice. | He |
| IO-NPs | Transferrin receptor | Transferrin | Doxorubicin/high intensity ultrasound | Cancer | Iron-platinum nanoparticles are encapsulated together with doxorubicin in nanobubbles (NB) functionalized with transferrin. High intensity focused ultrasound breaks the NBs, opens the blood brain barrier and enables the targeting of the glioblastoma in mice. | Chan |
| IO-NPs | Fibronectin | CREKA peptide | SQ photosensitizer near infrared = NIR | Cancer | IO-NPs functionalized with the peptide CREKA to target fibronectin in the ECM of tumors as well as the photosensitizer SQ. Growth of MDA-MB-231 tumors was clearly reduced in mice treated with these NPs in combination with NIR laser irradiation. | Wang |
| IO-NPs | Hsp70 | GranzymB | GrB/Hsp70 induction of apoptosis | Cancer | Hsp70 containing IO-NPs that bind to GranzymB on the surface of tumor cells which is followed by internalization and induction of apoptosis. Treatment of mice with HT1339 lung tumors or U87 glioma with Hsp70-IO-NPs increased the overall survival time. | Shevtzov |
| IO-NPs | Fibrin/ | CREKA peptide | Iron oxide (hyperthermia) | Cancer | Small IO-NPs with CREKA peptide as targeting moiety in combination with magnetic hyperthermia resulted in strongly reduced tumor growth in a murine 4T1 breast tumor model. | Du |
| IO-NPs | CD44 | Hyaluronic acid | Chlorin e6 photodynamic therapy | Cancer | IO-NPs with hyaluronic acid on the surface to target CD44 were further functionalized with the photosensitizer chlorin e6 which resulted in high toxicity after laser irradiation in BL6F1 cell | Dehvari |
| IO-NPs | Folic acid receptor | Folic acid | Doxorubicine released in redox response | Cancer | Micellar nanoparticles with folic acid as targeting ligand and IO-NPs and doxorubicin. Intravenous injection into HeLa tumor bearing mice massively reduced tumor size particularly in combination with magnetic targeting. | Wei |
| IO-NPs | EGFR | Anti-EGFR mAb | Magnetic resonance-guided focused ultrasound surgery (MRgFUS) | Cancer | Anti-EGF receptor antibody (Cetuximab) was attached to IO-NPs and used to treat nude rats with H460 lung cancer xenografts with MRgFUS. Application of anti-EGFR-IO-NPs reduced energy for MRgFUS and led to smaller tumor sizes. | Wang |
| IO-NPs | Urokinase plasminogen activator receptor (uPAR) | Amino-terminal fragment of urokinase plasminogen activator (ATF) | Cisplatin | Cancer | Milk protein coated IO-NPs loaded with Cisplatin and functionalized with ATF to bind to uPAR. Treatment of mice with orthotropic pancreatic tumors in mice with these IO-NPs strongly reduced the tumor weight. | Huang |
| Mn | αvβ3-Integrin | cRGDyK peptide | Mn2+−STING activation and anti-PD-L1 | Cancer | MnFe2O4 NPs labeled with RGD bind to αvβ3-integrins strongly expressed in many tumors. Treatment of mice with RGD-MnFe2O4 NPs inducted the STING pathway and resulted in a reduced tumor growth (B16F10, CT26, 4T1) in particularly in combination with αPD-L1 therapy. | Shi |
| Mn | Tumor tissue | Cancer cell membrane (homotypic targeting) | Doxorubicin | Cancer | Manganese dioxide coated gold nanorods loaded with doxorubicin were enwrapped in cancer cell membrane. Application in 4T1 breast tumor-bearing mice enhanced the efficacy of photothermal therapy and led to reduced tumor size. | Zhang |
| Mn | Transferrin receptor | Apoferritin | Doxorubicin | Cancer | MnO2 apoferritin NPs that target the transferrin receptor were loaded with doxorubicin. Treatment of 4T1 tumor bearing mice led to a strongly reduced tumor growth which was supposed to be based on a synergistic effect of MnO2 to increase the oxygen level and doxorubicin. | Veroniaina |
| Gd | Folate receptor | Folic acid | Titanium (Ti)/ROS-production | Cancer | NPs that incorporated Gd, Ti, and a near infrared dye into tannic acid (TA). NPs were further functionalized with folic acid to target the FA-receptor. Interestingly, administration of Gd-Ti-FA-TA NPs to mice with 4T1 tumors reduced tumor progression only in combination with 18FDG. | Huang |
| Gd | CD44 | Hyaluronic acid (HA) | Rosuvastatin (RST) | Atherosclerosis | Cerasomes modified with HA and RST selectively target CD44-positive cells in atherosclerotic plaques. Injection of these NPs in ApoE−/− mice on a high fat diet reduced plaque burden | Ma |
| Gd | VEGF receptor | VEGF mimetic peptide | QK peptide | Myocardial infarction | Gd-doped carbon dots (CD) were functionalized with the VEGF mimetic peptide QK that stimulates vascularization. Intravenous application of Gd-CD-QK NPs reduced adverse cardiac remodeling after myocardial ischemia/reperfusion injury in mice. | Li |
| Gd | αvβ3-Integrin | RGD peptide | Chlorin e6 (Ce6) | Cancer | DSPE-PEG2000 was modified with a peptide and DTPA (diethylenetriamine pentaacetic acid = Gd chelator) to generate organic NPs that contain Ce6 and Gd. These DSPM@Ce6@Gd NPs in combination with photodynamic therapy strongly inhibited the growth of A549 tumors in mice. | Yang |
| Gd | PS receptor | Phosphatidylserine (PS) | Liraglutide (GLP-1R agonist) | Atherosclerosis | Multilayered NPs decorated with PS and coated with PEG and gelatin. Liraglutide was inserted between the core and the gelatin layer. Intravenous injection of NPs into | Maiseyeu |
| Gd | αvβ3-Integrin | RGD peptide | Camptothecin (CPT)/NIR-photosensitizer (PPa-SH) | Cancer | A theranostic nanoprobe (Co-NP-RGD) with RGD-peptides for tumor targeting, a near infrared photosensitizer and CPT. Co-NP-RGD disassemble in the tumor releasing CPT/PPa-SH for chemo- and photodynamic therapy. Repetitive treatment of U87MG glioma mice with Co-NP-RGD and irradiation reduced tumor growth and increased the survival of the animals. | An |
| Gd | Methotrexat (MTX) | Folate receptor | Artesunate (ASA)/Methotrexat | Cancer | MTX, ASA and Gd were assembled into NPs (ASA-MTX-GdIII) for combined chemo-dynamics (ROS-production) and chemotherapy. NPs are taken up | Fan |
| Gd/IO | αvβ3-Integrin | RGD peptide | Docetaxel (DTX) | Cancer | Preparation of a Gd-containing IO-nanocluster further functionalized with RGD for targeting the integrin αvβ3 and docetaxel for therapy (cRGD-GdIO-DTX). NPs degrade in the acidic tumor environment and release DTX. Systemic application of cRGD-GdIO-DTX to mice with implanted Panc-1 pancreatic cancer cells strongly impaired tumor growth. | Wang |
| MR-Contrast | Target | Ligand | Therapeutic drug/therapy | Disease | Brief summary | Reference |
|---|---|---|---|---|---|---|
| PFOB | Rapamycin | Duchenne muscular dystrophy | Rapamycin-loaded NPs restore autophagy and improve muscle and cardiac function in mdx mice beyond conventional treatment. | Bibee | ||
| PFOB | Celecoxib | Neuroinflammation | Celecoxib nanoemulsions target macrophages, reduce PGE2 and inflammation, and relieve neuropathic pain with minimal systemic exposure. | Janjic | ||
| PFOB | siRNA | Pulmonary fibrosis | PFOB-NE enhance pulmonary siRNA delivery, effectively silencing STAT3/CXCR4 and inhibiting lung fibrosis progression. | Ding | ||
| HFBA | siRNA | Osteosarcoma | F-PCX@PFC nanoemulsions deliver siSTAT3 to lungs, inhibit immunosuppression, and prolong survival in metastatic osteosarcoma models. | Li | ||
| PFTBA | PD-L1 | PD-1 | Membrane vesicles of salmonella typhimurium | Tumor | Hybrid membrane-coated nanoemulsions enhance targeted PD-L1 blockade, photothermal therapy, and T cell immunity to inhibit tumor growth and metastasis. | Zhang |
| PFOB | Folate receptor | Folic acid | Doxorubicin | Nasopharyngeal tumor | Folate-targeted PLGA-PEG NPs co-deliver Dox and imaging agents, enabling targeted chemotherapy and dual 19F MRI/NIR tumor tracking. | Vu-Quang |
| F68 | High intensity focused ultrasound | Tumor | 19F MRI tracks PFC-NE in tumors, optimizing HIFU ablation efficacy and necrosis based on PFC-NE accumulation. | Shin | ||
| PFOB | Integrin | αVβ3 | Rapamycin | Stenosis | αvβ3-targeted rapamycin NPs reduce vascular stenosis after balloon injury without impairing endothelial healing in rabbits. | Cyrus |
- —Deutsche Forschungsgemeinschaft10.13039/501100001659
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLanthanide and Transition Metal Complexes · Atomic and Subatomic Physics Research · Nanoparticle-Based Drug Delivery
Introduction
The immune system
Pathogenic challenges are daily threats for every organism. In normal circumstances, it is difficult for microbes to pass the anatomical and physiological barriers of the human body. However, pathogenic bacteria and viruses can infect the tissue via the epithelial lining of the mucosal tissue and induce an inflammation. Inflammatory environments are governed by different immune cells infiltrating the inflammatory hot spot as well as the release of pro-resolving factors to challenge invading pathogens leading from a pro- to an anti-inflammatory state while recognizing the host organism and limiting damage to itself. In the recent years, it has become more and more clear that the coordination of these complex immune processes is of huge medical relevance. On the one hand, a proper orchestration of the inflammatory response is essential to fight against pathogenic microorganisms, on the other hand, the immune system is also crucially involved in the development and progression of multiple diseases which are not caused by pathogens like myocardial infarction [1], atherosclerosis [2], or even schizophrenia [3].
Innate and adaptive immunity
Over millions of years, the immune system has repeatedly adapted and developed to changing circumstances. The immune system in vertebrates is roughly divided into two complementary arms: the innate and the adaptive immune systems. The innate immune system serves as the body’s first line of defense against invading pathogens. It consists of anatomical and physiological barriers, antimicrobial enzymes like lysozymes in saliva and mucus and a diverse population of immune cells. In addition, the skin and gut microbiota contribute to host protection by outcompeting pathogenic microbes. The critical role of innate immunity becomes evident in individuals with immunodeficiencies, who are more susceptible to severe and life-threatening infections [4]. Upon tissue injury or pathogen invasion, danger-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs) are released [5]. These molecules are recognized by innate immune cells such as macrophages and dendritic cells, which initiate an inflammatory response through the secretion of cytokines and chemokines. This process activates endothelial cells and promotes the recruitment of immune cells from the bloodstream into the damaged tissue. Neutrophils are one of the first responders and play a central role in pathogen clearance through mechanisms such as phagocytosis, the release of reactive oxygen species and NETosis. Monocytes, which arrive shortly after neutrophils, differentiate into macrophages or dendritic cells at the site of inflammation and further coordinate the immune response (Fig. 1, left). If the innate response is insufficient or if the body encounters the same pathogen again, the adaptive immune system is activated. This system features highly specific T and B lymphocytes capable of recognizing antigens presented by antigen-presenting cells. Dendritic cells play a pivotal role in this process by migrating to lymph nodes, where they present processed antigens via MHC (major histocompatibility complex) molecules to CD4^+^ helper T cells and CD8^+^ cytotoxic T cells. The latter eliminate infected cells, while helper T cells support B cell activation and antibody production, as well as macrophage function at the inflammation site. A hallmark of the adaptive immune system is the development of immunological memory, allowing for faster and more effective responses upon re-exposure to the same pathogen (Fig. 1, right). This feature is the foundation of vaccination, which aims to induce long-lasting protection against infectious agents. Together, the innate and adaptive immune systems form a highly coordinated and dynamic network essential for maintaining immune surveillance, eliminating pathogens, and resolving inflammation.
The immune system is divided into the innate and adaptive immune response. In response to bacterial infections, pathogen-associated molecular patterns (PAMPs) are released that activate surrounding immune cells like tissue macrophages or dendritic cells. These cells secrete cytokines/chemokines to attract other immune cells such as neutrophils and later also monocytes. This first innate response is usually sufficient to control most of the invading pathogens. In parallel, dendritic cells become activated and migrate into the draining lymph nodes to present antigenic peptides or lipids of the pathogens to T and B cells. In the event of further infection, the adaptive immune system is directly involved and B as well as T cells are able to remember the pathogens and either secrete antibodies or eliminate cells infected by these pathogens.
Imaging of inflammation
As outlined above, the innate and adaptive immune response is a highly complex system that is constantly changing and interacting with the environment in order to suppress the onset of disease. It is therefore obvious that the visualization of immune cells in vivo covers an important area of clinical research in order to be able to make a timely statement about the current status and also the course of a disease. This urgency is not only the case for acute diseases caused by pathogens but also in in chronic states such as cardiovascular diseases, neurodegenerative disorders or even cancer. For this reason, it is important to be able to visualize inflammatory processes in vivo. This not only enables the exact localization of the site of inflammation but also allows for long-term studies to monitor the further development of a disease. Various imaging modalities are available for this purpose, such as positron emission tomography (PET), single-photon emission computed tomography (SPECT), or magnetic resonance imaging (MRI), which enable long-term examination of a disease and have a sufficient penetration depth. However, beside PET and SPECT which both rely on radioactive nuclides, MRI provides superior soft tissue contrast and has proven to be a very versatile tool for tracking specific inflammatory processes in vivo by combining the conventional proton imaging (^1^H) with different contrast agents like gadolinium (Gd), manganese (Mn), superparamagnetic iron oxide nanoparticles (IO-NPs), or fluorine (^19^F).
Conventional contrast agents for 1H MRI
Gadolinium (Gd^3+^) is a highly paramagnetic ion; the presence of seven unpaired electrons confers a substantial magnetic moment, resulting in a strong T1-relaxation enhancement of adjacent water protons. Gd-based contrast agents (GBCAs) are the most widely used MR-CAs with ∼63 million doses in 2023 [6]. However, free Gd^3+^ is highly toxic and is associated with the development of nephrogenic fibrosis in patients with impaired kidney function [7]. More recently, it has been found that GBCAs accumulate in the brain of patients with normal kidney function who received repetitive Gd-based MRI examinations which has again questioned the safety of GBCAs [8]. Nevertheless, the overall safety-profile of GBCAs is good with only few adverse events [8]. GBCAs are mostly used for diagnostics of the brain, the cardiovascular system, the abdomen, and the musculoskeletal system [6].
Manganese (Mn^2+^) is another paramagnetic MR-contrast agent with five unpaired electrons. Similar as GBCAs, accumulation of Mn^2+^ ions induce bright signals in T1-weighted images but also darkens T2-weighted MR-images and therefore has also been used as dual-mode agent [9]. For contrast enhanced MRI, Mn^2+^ can be used as salt (MnCl_2_). Soluble Mn^2+^ enters the cells via Ca^2+^ channels and has been used for visualization of viable myocardium after myocardial infarction in mice [10].
Iron oxide nanoparticles (IO-NPs) exhibit strong superparamagnetic behavior when placed in an external magnetic field. This effect disturbs the local magnetic field and enhances the dephasing of the spins of the surrounding water molecules which results in a strong decay of the T2 signal and leads to the darkening of the anatomical ^1^H MR image [11]. Some IO-NPs are avidly taken up by phagocytic immune cells and have been used in preclinical, but also clinical studies to visualize the accumulation of monocytes/macrophages in inflammatory lesions [12]. One important advantage of IO-NPs is the very high sensitivity which has enabled even single-cell tracking of monocytes in the brain [13].
Despite excellent sensitivity, all these approaches have the disadvantage that local deposition of those CAs creates hypo/hyperintense regions in affected tissues with the entire anatomy of the investigated object as background signal, which makes an unambiguous identification in vivo difficult or even impossible.
Detection of inflammation by combined 1H and 19F MRI
As an alternative, ^19^F MRI has emerged in the recent years as a powerful tool for imaging of inflammatory processes. A major advantage of this technique is that fluorine is virtually absent from the human body, meaning that externally administered fluorine-containing contrast agents can be clearly detected without any significant background interference. Moreover, the resulting fluorine signal can be easily merged with anatomical ^1^H MR images, enabling its precise localization. However, a limitation of fluorinated compounds with a high payload of ^19^F nuclei is their hydrophobic nature, making them insoluble in water and most other biological fluids (e.g. blood). To overcome this, they must be formulated as nanoemulsions through high-pressure homogenization to form fluorine-based nanoparticles (FNPs) (Fig. 2, top). In a groundbreaking paper Ahrens et al. demonstrated that dendritic cells can be labeled ex vivo with such FNPs and subsequently tracked in vivo following intramuscular injection [16]. A few years later, our working group went one step further and applied the FNPs directly in vivo. After intravenous injection, these nanoemulsions are taken up by phagocytic immune cells in the bloodstream, particularly monocytes and neutrophils. In the presence of inflammation, these labeled immune cells migrate to the inflammatory foci, where they can be visualized using combined ¹H/¹⁹F MRI. This approach allows for the tracking of immune cell infiltration across a wide range of diseases, including myocardial infarction [14], graft rejection [17], or pulmonary inflammation [15] (Fig. 2, bottom). However, some studies have also shown that, under certain conditions, other cell types—such as neutrophils [18] or even specific stem cell populations in the heart [19]—can also be labeled upon intravenous administration of FNPs, depending on the time point of injection. Beyond this passive labeling by phagocytosis, cells and other epitopes can also be actively targeted via specific ligands that have been coupled to the FNPs.
FNPs are prepared by mixing buffer with lipids, fluorescent-labeled lipids for flow cytometry or microscopy and the perfluoro-15-crown-5 ether followed by high pressure homogenization at 1000 bar. Upon injection into the blood stream, FNPs are taken up by different immune cells from the blood, e.g. monocytes and neutrophils. In case of an inflammation these labeled cells infiltrate into the inflammatory hot spot and can be visualized via combined 1H/19F MRI. Adapted from Flögel et al. 2008 (left; myocardial infarction) [14] and Ebner et al. 2010 (right; pneumonia) [15].
Active targeting of FNPs
Active targeting of FNPs makes use of the binding properties of specific ligands such as antibodies, peptides, sugars or nanobodies. These can be coupled to the FNP surface via functional groups. A common method is to couple the ligands to maleimide-functionalized lipids (Fig. 3, top), which is either incorporated directly into the FNPs or can be integrated into the pre-formulated FNPs at a later stage via the sterol-based post insertion technique (SPIT) [23]. In this way, a wide variety of cells can be targeted, provided, of course, that the ligand has a high specificity for the selected epitopes. In addition, it must first be ensured that those targeted FNPs are not also passively taken up by phagocytic cells. The common gold standard for protection of NPs against phagocytosis is surface PEGylation (Fig. 3, top). The long PEG chains prevent the binding of serum proteins, a process which normally leads to formation of a protein corona facilitating their phagocytosis by monocytes/macrophages. If serum proteins bind to the nanoemulsions through van der Waals or other electrostatic forces, the PEG chains are compressed, absorb energy, and then release it again by repelling the serum proteins [24]. Thus, PEGylation makes recognition of NPs by phagocytic cells more difficult [25]. Furthermore, the surface charge becomes more neutral, another factor that reduces non-specific uptake [26]. However, a potential drawback is, that repeated administration of PEGylated NPs can induce the formation of anti-PEG antibodies, which may lead to rapid particle clearance or, in severe cases, anaphylactic reactions [27]. Consequently, ongoing research is exploring alternative strategies, such as the use of CD47 as a ‘don’t eat me’ signal [28]. Another interesting approach is the utilization of zwitterionic coating of FNPs to prevent the building of a protein corona resulting in less uptake by the reticuloendothelial system (RES) [29, 30]. Beyond accumulation in the RES, it is important to note that most NPs, aside from their surface modifications, tend to accumulate in the spleen and liver, which poses a significant challenge for various diagnostic and therapeutic applications. It is therefore essential to reduce this enrichment as much as possible in order to also enable imaging/therapy in these organs without side effects in the future.
For active targeting approaches, FNPs with a functional maleimide group on their surface as well as a PEG chain are prepared. After coupling of different peptides (@ CD63, @ factor XIII, @ CD177) to the maleimide group on the surface of the FNPs they can be injected intravenously. With this approach it is possible to target activated cardiac fibroblasts (@ CD63), thrombi (@ factor XIII) or neutrophils (@ CD177). Adapted from Martinez et al. 2025 (left) [20], Temme et al. (middle) [21], and Bouvain et al. (right) [22].
Despite these limitations, this approach enables the targeted labeling of specific cell populations or tissue structures. As an example, we demonstrated that the coupling of targeting peptides—such as those directed against α2-antiplasmin or fibrin—allows for the active targeting of acute and chronic thrombi. These can be detected in vivo using combined ^1^H/^19^F MRI [21] (Fig. 3, middle). α2-antiplasmin-decorated FNPs bind to fibrin through crosslinking by activated factor XIII during the early stages of thrombus formation and were administered to mice in which thrombi had been induced in the vena cava using FeCl_3_ (Fig. 3, bottom middle) [21]. Beyond this, within the cardiovascular field, several other applications were reported using targeted FNPs. Waters et al. [31] prepared α_v_β_3_-specific FNPs to image aortic valve disease in a rabbit model while Southworth et al. [32] designed VCAM-1-specific FNPs to target general inflammation in the context of atherosclerosis. Another important field of FNP-based molecular imaging is oncology. Several years ago, Bae et al. [33] employed folate receptor-targeted FNPs to visualize nasopharyngeal tumors. In addition, angiogenesis during tumor progression was successfully monitored in a brain tumor model using FNPs also functionalized with an α_v_β_3_-specific ligand [34].
In addition to this tissue selective approaches, distinct cell populations can also be visualized using this approach. We recently demonstrated that activated cardiac fibroblasts can be specifically labeled and subsequently detected within the infarcted heart (Fig. 3, bottom left) via upregulation of CD63 on their cell surface [20]. Moreover, by employing a peptide binding to CD177, we successfully labeled neutrophils in the bone marrow using targeted FNPs. Following the induction of acute experimental myocardial infarction, we were able to monitor the mobilization of neutrophils from the bone marrow and track their migration into the inflamed heart tissue in vivo [22] (Fig. 3, bottom right).
Theranostics
Beyond ‘just’ imaging, the combination of imaging and direct therapeutic intervention—commonly referred to as theranostics—is an important development. This approach offers the advantage of not only visualizing biological processes but also inducing targeted functional changes within the affected tissue at the same time.
Targeted theranostics and magnetic resonance imaging in general
MRI-based theranostics has been mostly used for preclinical cancer models but also for imaging and treatment of cardiovascular diseases. Similarly as pointed out above, the most widely used MRI CAs that were used for theranostics are IO-NPs, Mn or Gd, whereby Mn or Gd are either complexed in chelates or are also doped/encapsulated in NPs. In the following, we briefly describe some general aspects for theranostic applications with these CAs and then describe few examples of targeted theranostics in more detail. A broader overview about studies on MRI-based theranostics is provided in Table 1.
Iron oxide nanoparticles
Analogous to FNPs, the surface of IO-NPs can also be functionalized with targeting ligands like antibodies, antibody-derivatives, peptides or other small molecular ligands and have similarly been used for targeted cell tracking or thrombus imaging [60] as well as been doped or functionalized with drugs for therapeutic purposes [61]. For the latter, applications for treatment of anemia, chemotherapy, hyperthermia, chemodynamic-, or immunotherapy have been reported [11]. For example, ferumoxytol is approved for treatment of patients with anemia and chronic kidney diseases [62]. Another interesting observation is that exposure of tumor-associated macrophages to IO-NPs shifts their polarization towards an pro-inflammatory phenotype with elevated production of reactive oxygen species (ROS) that supports the immune response against cancer [63]. Other therapeutic approaches are magnetic hyperthermia where an alternating external magnetic field produces heat that enhances the local immune response against tumors and also drives tumor-cells into apoptosis [64].
Beyond those rather non-specific approaches, targeting of IO-NPs enables a more directed delivery of the imaging agent as well as the therapeutic substance to a certain site of the body or specific cell-types or structures. This enhances the local concentration of the drug, increases the efficiency and also reduces side effects. Active targeting of IO-NPs can be conducted by functionalization of the nanoparticle surface with targeting ligands or magnetic targeting. For magnetic drug targeting a strong magnet is placed above the target site that attracts and locally fixes the IO-NPs and thereby enhances the local accumulation of the drug-loaded IO-NPs [64]. On the other hand, for specific targeting, Schleich et al. [65] modified IO-containing nanoparticles with paclitaxel (PTX) and a tripeptide composed of arginine-glycine-aspartic acid (RGD) for targeting α_v_β_3_-integrins. Paclitaxel is a chemotherapeutic drug that inhibits the proliferation of tumor cells by binding to β-tubulin which blocks the degradation of microtubuli and arrests the cells in the G2-/M-phase. The linear RGD peptide motive is found in many molecules involved in cell adhesion or signaling like fibronectin, vitronectin, or fibrinogen and binds to different integrin molecules [66]. Due to the fact that integrins like α_v_β_3_ or α_v_β_5_ are overexpressed in the vasculature of tumors, but are also found on the surface of tumor cells, RGD-targeting has been widely used for tumor imaging, but also for targeted drug delivery. Here, CT26-tumor bearing mice were treated with RGD-targeted SPIO/PTX-NP (or control NPs) which revealed that RGD-targeting in combination with magnetic targeting strongly reduced the tumor growth and elevated the survival rate. Interestingly, RGD- or magnetic-targeting had a similar effect that was higher as untargeted controls. This was in agreement with T2-weighted (T2w) MRI of the tumor which showed dark spots with heterogeneous distribution within the tumor after application of RGD-targeted NPs, magnetic targeting or both.
In a more recent study, Wang et al. [59] prepared IO-NPs that contain docetaxel as anti-cancer drug and a cyclic version of the RGD peptide (cRGD) for integrin targeting on pancreatic cancer cells. Of note, the authors also incorporated Gd to generate a T1-T2 dual-mode imaging (Gd/IO) nanocluster. Docotaxel (DTX) is also an anti-cancer drug that belongs to the same group of molecules as paclitaxel (taxanes). It has a similar mode of action and blocks the proliferation of cells by binding and stabilizing microtubuli and by induction of apoptosis. In vitro, application of cRGD-GdIO-DTX targeted NPs had a stronger negative effect on cell viability of Panc-1 cells than untargeted GdIO-DTX. Quite impressive results were obtained in vivo, where application cRGD-GdIO-DTX nearly completely inhibited the growth of subcutaneously implanted Pac-1 tumor cells in nude mice. Finally, MRI revealed that injection of cRGD-GdIO-DTX resulted in enhanced T1w and darkened T2w images.
IO-NPs have also been utilized in regenerative medicine for example to load and track therapeutic cells. De Vries et al. [67] labeled autologous immature dendritic cells with SPIOs and reinjected them into the lymph nodes of stage-III melanoma patients and subsequently investigated the localization and migration by scintigraphy or MRI. Interestingly, MRI was superior to assess the precise localization of DCs in or outside of lymph nodes which is important for the proper induction of an immune response. Furthermore, iron oxide labeled scaffolds (e.g. collagen or vascular grafts) have been developed where the proper localization as well was the stability of the device can be analyzed over time by MRI [68, 69].
Manganese
Mn-based MRI has been used for diagnostic purposes (see above) but also for therapeutics and theranostics [70]. Mn^2+^ in the cytosol can for example induce Fenton-like reactions that generate ROS and therefore has been used for chemodynamic therapy [71]. Mn has also been shown to stimulate the innate immune system by activation of the cGAS-STING pathway [72] that can be exploited for immunotherapy [70]. Furthermore, Mn-NPs can also be loaded with drugs for therapy. For example, Pan et al. generated BSA (bovine serum albumine)-MnO_2_ NPs functionalized with paclitaxel for chemotherapy against cancer [73].
A targeted approach has been conducted by Zhou et al. [74] who generated Mn-CaPO_4_ NPs loaded with doxorubicin that were functionalized with the EGFR-specific antibody C225. These NPs were efficiently internalized by EGFR-positive BxPC-3 cancer cells and exhibited toxic effects after uptake. Conjugation of mAb C225 to the nanoparticles further enhanced the cellular toxicity about 1.5-fold.
Shi et al. 2024 generated RGD-targeted magnetic Mn-containing ferrite NPs (MnFe_2_O_4_) and exploited their utility for anti-cancer therapy. The authors found that RGD-MnFe_2_O_4_ showed increased accumulation in tumors and was retained inside the tumor tissue for longer periods of time. Moreover, these nanoparticles stimulated the cGAS-STING pathway in an immortalized dendritic cell line which was assessed by analysis of phosphorylated TBK1 and the translocation of STING from the cytoplasm to the nucleus. Treatment of several tumors revealed that exposure to RGD-NPs or anti-PDL1 decreased tumor growth, which was strongly increased when RGD-NPs were used in combination with anti-PDL1. Furthermore, treatment of mice bearing CT26 tumors with RGD-NPs plus anti-PDL1 resulted in higher numbers of CD8^+^/CD4^+^ T cells, activated CD69^+^ T cells and CD86^+^ dendritic cells in the tumor tissue.
Gadolinium
In addition to the normal use of GBCAs (e.g. first pass or late Gd enhancement (LGE)) they have also been combined with therapeutic molecules for MR theranostics [75]. Wang et al. [59] generated iron- and Gd-containing nanocluster that were functionalized with the peptide cRGD as well as the anti-tumor drug docetaxel (DTX → cRGD-GdIO-DTX) for targeting of α_v_β_3_ integrins on the surface of Panc-1 pancreatic cancer cells. Here, the inhibition of proliferation of Panc-1 or SW1990 cells was much stronger than that by untargeted particles. Furthermore, in nude mice with a human pancreatic cancer xenograft, cRGD-GdIO-DTX slowed tumor development and in parallel showed signal enhancement in MRI. In another study, Ma et al. [53] generated hyaluronic acid (HA) containing cerasomes (HA-CC) that selectively recognize CD44-positive cells within atherosclerotic plaques. Cerasomes are liposome-like NPs that were generated by a combination of organoalkoxysilane lipid 1, phosphoethanolamine, and phosphatidylcholine. HA was linked to the surface of the nanoarticles and for therapeutic purposes, the authors also incorporated the rosuvastatin (RST) into the hydrophobic layer to produce HA-CC-RST. RST is a hydrophobic drug that belongs to the group of statins and inhibits the biosynthesis of cholesterol by blocking the conversion of HMG-CoA to mevalonate via the enzyme HMG-CoA reductase. Importantly, recent data indicates that statins also have anti-inflammatory or immunomodulatory effects that could reduce the plaque burden [76]. To visualize the accumulation of these nanoparticles within atherosclerotic plaques, Gadodiamide was also inserted into the CCs. T1w MRI revealed an increased accumulation of HA-CCs in the aortic wall of ApoE^−/−^ mice fed with a high-fat diet leading to an enhanced MRI contrast in atherosclerotic plaques compared to non-targeted CCs. Furthermore, treatment of ApoE^−/−^ mice with HA-CC-RST significantly decreased the amount of atherosclerotic lesions by ∼56% and also the overall proinflammatory profile. Of note, HA-CC-RST was more effective than the systemic administration of RST.
Taken together, a wide range of theranostic applications has already been investigated using conventional MRI CAs, but as mentioned above, none of the three classic agents (IO-NP, GBCAs, manganese) are inert in themselves, which means that they can trigger (undesirable) signal cascades.
FNP-based theranostics
In addition to the broad potential of theranostic applications, numerous approaches have recently emerged that utilize ¹⁹F MRI for diagnostic purposes. One of the main challenges in this context lies in the physicochemical nature of FNPs. Due to their fluorophilic and hydrophobic core, water-insoluble drugs cannot simply be incorporated via conventional emulsification techniques. However, this limitation has been successfully addressed through the development of triphasic systems [77–79] or double emulsions [80–82], which allow for the integration of otherwise incompatible compounds. This advancement has already enabled the successful implementation of several theranostic strategies. For instance, small molecules such as rapamycin have been employed to treat muscular dystrophy [83], while celecoxib has been used to target neuroinflammation [84]. In addition to small molecules, other bioactive compounds have also been incorporated into FNPs. For example, siRNA targeting the STAT3 signaling pathway has shown therapeutic efficacy in both idiopathic pulmonary fibrosis [85] and lung metastatic osteosarcoma [86]. Furthermore, proteins and peptides, such as those targeting lactate oxidase, have been utilized in the treatment of breast cancer [87]. Recently, Vu-Quang et al. made use of dual-labeled near infrared and ^19^F NPs for delivery of doxorubicin to nasopharyngeal tumors via folate receptor targeting. They could show that killing of cancer cells was significantly improved in comparison to non-folate targeted nanoparticles [88].
A completely different strategy has been explored through the combination of FNPs with high-intensity focused ultrasound (HIFU), enabling both imaging and therapeutic applications. This is used to treat tumors and has already been approved by the FDA for the treatment of certain types of cancer, such as prostate cancer [89]. The method is based on the bundling of sound waves to destroy tissue through overheating. Current research is focusing on microbubbles to reduce treatment time and the acoustic energy. However, microbubbles have only a blood half-life of several minutes which significantly complicates the infusion into the tumor. For this reason, Shin et al. used FNPs. This enables precise imaging of the tumor through accumulation of the FNPs and also allows the concentration to be determined on site. It was found that a concentration of 2–3 mg/ml FNPs had the most promising effect in combating the tumor [90]. An overview of all studies is given in Table 2.
Simultaneous imaging and functional modification of neutrophils
Most recently, we have further developed the neutrophil imaging technology into a theranostic approach. In order to advance the pure targeting of neutrophils into a theranostic approach, we additionally equipped the surface of the FNPs with fMLP to generate neutrophil-activating ^aNP^FNPs. The fMLP moiety activates cells via the G protein-coupled receptor FPR1. Although FPR1 is not exclusively expressed on neutrophils, our data show that CD177-mediated binding predominates, preserving high targeting specificity. Importantly, we investigated whether this system could also induce neutrophil activation. Indeed, incubation with ^aNP^FNPs increased the expression of activation markers, enhanced reactive oxygen species production, and promoted both E. coli phagocytosis and migration into inflamed tissue (Fig. 4) [92].
a) For combining therapy and diagnosis we modified the neutrophil-specific FNPs with an additional fMLP for functional activation of neutrophils to form aNPFNPs. b + c) Although fMLP binds to the FPR1 receptor, which is expressed not exclusively by neutrophils but also monocytes, the aNPFNPs still predominantly target neutrophils. Beside their binding we could detect an increase in the surface activation marker CD11b (d) due to the treatment as well as increased production of reactive oxygen species (e), phagocytosis of E. coli particles (f) and stronger migratory capacities (g). Adapted from Bouvain et al. [92].
After confirming that this approach selectively activates neutrophils while leaving other immune cells largely unaffected, we evaluated its therapeutic potential in an established disease model. In acute colitis—characterized by intestinal epithelial cell death and subsequent bacterial translocation—neutrophils are among the first responders. Via non-invasive mapping we could find strong neutrophil influx into the affected gut. Pre-activation with ^aNP^FNPs markedly improved disease outcome, as evidenced by reduced weight loss and significantly improved histological colitis scores compared to control-treated mice (Fig. 5) [92].
a) Shown is the intestinal tract of mice suffering from DSS-induced acute colitis. Neutrophils in the inflamed intestine can be detected by injecting neutrophil-specific FNPs (conFNPs) and the theranostic variant, which was additionally functionalized with fMLP on its surface (aNPFNPs). Treatment with aNPFNPs not only shows increased migration of neutrophils to the affected area, but also an improved outcome after colitis. This was quantified on one hand by lower weight loss over time (b) and on the other hand by a significantly lower colitis score (c), which reflects the severity of colitis based on histological evaluation. Adapted from Bouvain et al. [92].
Future perspective
^19^F MRI for molecular imaging purposes has developed at remarkable speed. Since the first demonstrations of in vivo imaging of inflammatory processes nearly two decades ago, the field has advanced enormously. Today, it is possible not only to visualize distinct immune cell populations in vivo but also to simultaneously address multiple targets by employing different FNP formulations. Moreover, the field has evolved beyond pure diagnostics: fluorine-based nanoplatforms can now be harnessed for therapeutic purposes, enabling functional modulation of immune cells and targeted intervention in disease processes. With continuous advances, the implementation of this technology in clinical practice is getting closer and promises a new era of precise and personalized theranostics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weiss JN, Goldhaber JI, Ji S. Oxygen free radicals in the pathophysiology of myocardial ischemia/reperfusion. In: Tarr M, Samson F (eds.), Oxygen Free Radicals in Tissue Damage. Boston, MA: Birkhäuser, 1993, 250–66.
- 2Aronova A, Tosato F, Naser N et al Innate immune pathways in atherosclerosis—from signaling to long-term epigenetic reprogramming. Cells 2023;12:2359. 10.3390/cells 1219235937830572 PMC 10571887 · doi ↗ · pubmed ↗
- 3Khandaker GM, Cousins L, Deakin J et al Inflammation and immunity in schizophrenia: implications for pathophysiology and treatment. Lancet Psychiatry 2015;2:258–70. 10.1016/S 2215-0366(14)00122-926359903 PMC 4595998 · doi ↗ · pubmed ↗
- 4Shoenfeld Y, Gershwin ME. Contemporary Challenges in Autoimmunity, Vol. 1173. Boston, MA: John Wiley & Sons, 2009.
- 5Bianchi ME . DAM Ps, PAM Ps and alarmins: all we need to know about danger. J Leukoc Biol 2007;81:1–5. 10.1189/jlb.0306164 · doi ↗
- 6Quattrocchi CC, Rovira À, van der Molen AJ et al ESR essentials: gadolinium-wise MRI—practice recommendations by the European Society for Magnetic Resonance in Medicine and Biology. Eur Radiol 2025;35:3347–53. 10.1007/s 00330-024-11214-439702634 PMC 12081572 · doi ↗ · pubmed ↗
- 7Hasebroock KM, Serkova NJ. Toxicity of MRI and CT contrast agents. Expert Opin Drug Metab Toxicol 2009;5:403–16. 10.1517/1742525090287379619368492 · doi ↗ · pubmed ↗
- 8Kim H-K, Lee GH, Chang Y. Gadolinium as an MRI contrast agent. Future Med Chem 2018;10:639–61. 10.4155/fmc-2017-021529412006 · doi ↗ · pubmed ↗