Persistent Esophageal Parakeratosis With Recurrent Candida Esophagitis in a Virally Suppressed Person With HIV
Rizgar Hama-Salih, Mohammad Alsaadony, Kushal Panja, Deepa Bai, Madiha Erashdi, Emil Salmo

TL;DR
A person with HIV experienced persistent esophageal changes resembling cancer, but tests showed no malignancy, highlighting the need for careful diagnosis and tailored management.
Contribution
This case highlights the rare presentation of esophageal parakeratosis in a virally suppressed HIV patient and emphasizes diagnostic and management considerations.
Findings
Serial biopsies showed parakeratosis without malignancy despite alarming endoscopic appearance.
Symptoms improved partially with acid suppression, antifungal treatment, and micronutrient supplementation.
Esophageal manometry was considered to evaluate motility due to ongoing dysphagia.
Abstract
Esophageal parakeratosis is an uncommon histopathologic finding that can closely mimic malignancy endoscopically and has been linked to micronutrient deficiency states and chronic reflux. We report a 57-year-old man with well-controlled HIV (stable viral suppression and robust CD4 count) who developed progressive dysphagia with malignant-appearing esophageal plaques over a long segment of the mid-to-distal esophagus. Serial biopsies repeatedly showed parakeratosis/hyperkeratosis without dysplasia or malignancy, with intermittent Candida on histology. Despite the alarming appearance, cross-sectional imaging revealed no mass or nodal disease. Management included high-dose acid suppression, short courses of fluconazole for Candida esophagitis, and empiric zinc and riboflavin supplementation; the endoscopic extent of keratinization reduced but persisted, and dysphagia fluctuated without a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
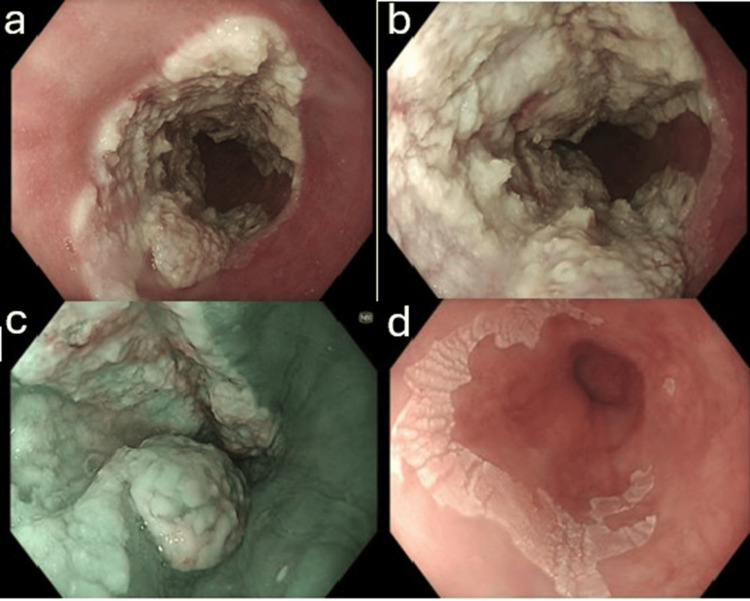 Figure 1
Figure 1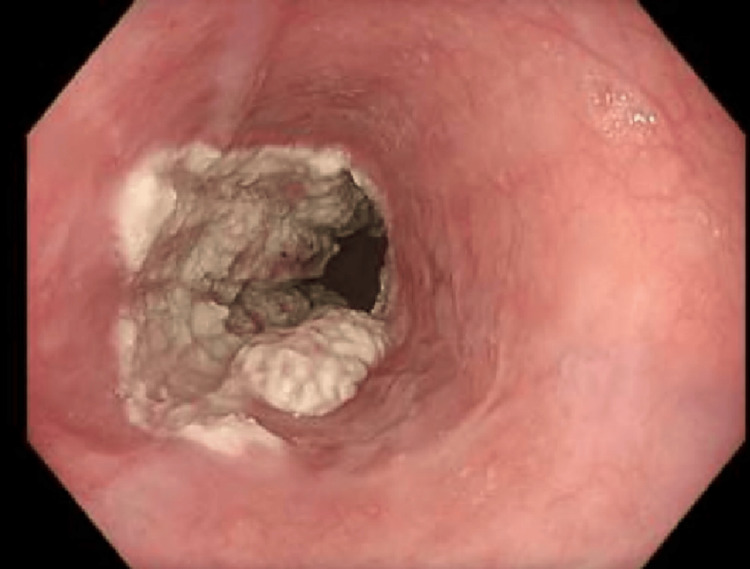 Figure 2
Figure 2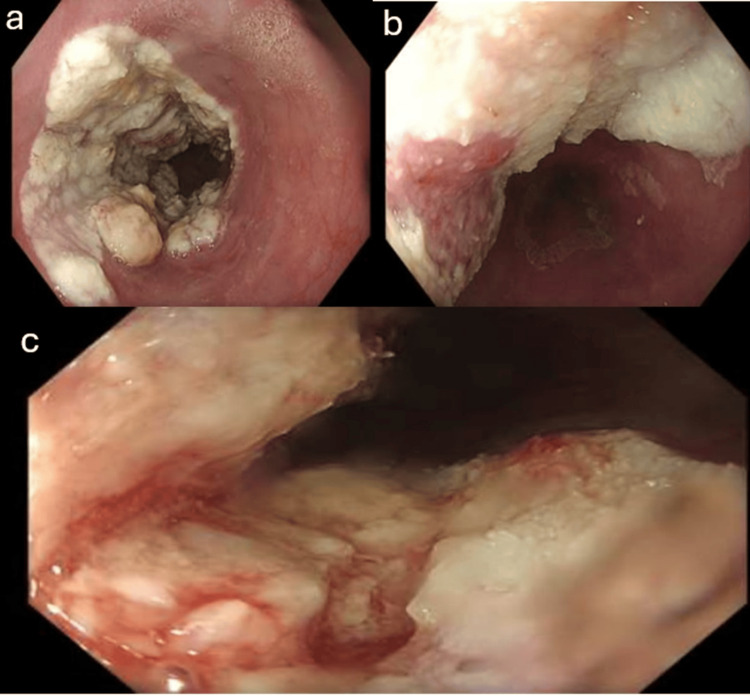 Figure 3
Figure 3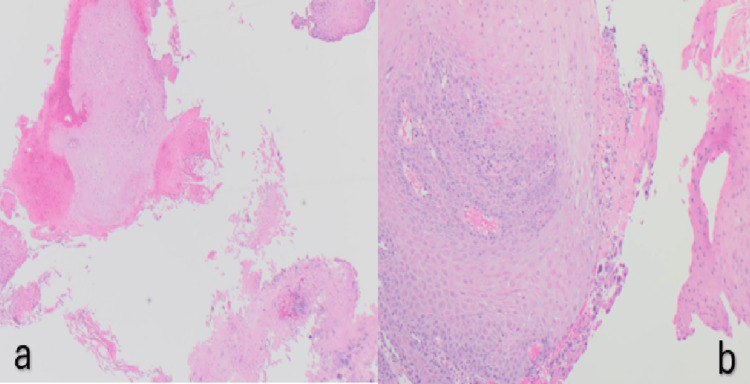 Figure 4
Figure 4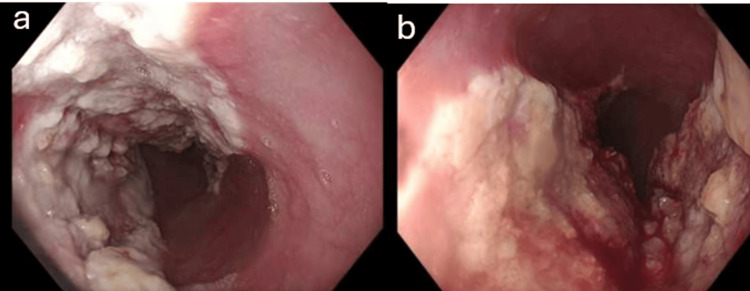 Figure 5
Figure 5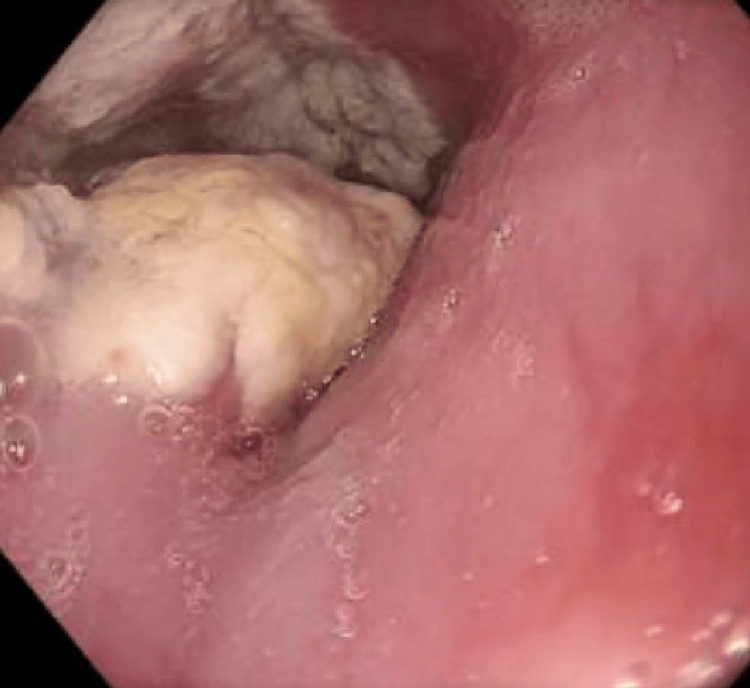 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Cytomegalovirus and herpesvirus research · HIV-related health complications and treatments
Introduction
Esophageal parakeratosis is a rare finding characterized histologically by a hyperkeratinized squamous epithelium with retained pyknotic nuclei, often presenting endoscopically as white plaques or thickened mucosa that can closely mimic dysplasia or early neoplasia [1]. In the limited case literature, some reports have linked its development to micronutrient deficiencies, particularly riboflavin and zinc, and observed partial regression after repletion [2,3].
Candida esophagitis (CE), classically associated with immunocompromise, is increasingly recognized among patients without profound immunosuppression. In a cohort of “immunocompetent” patients, proton-pump inhibitor (PPI) use was identified as the most common associated risk factor (odds ratio (OR) ~1.69) [4]. A larger Japanese cross-sectional study of 7,736 patients undergoing endoscopy found PPI use (OR 1.69), diabetes, atrophic gastritis, and gastrectomy to be independent risk factors for CE even in patients without overt immunodeficiency [5]. In a clinical series, 63-81% of esophageal candidiasis cases had coexisting exposure to PPIs, underlining the strong pharmacologic association [6]. These data suggest that acid suppression may predispose to fungal overgrowth via hypochlorhydria and local mucosal changes.
Given the striking endoscopic mimicry of neoplasia in parakeratosis, the paucity of surveillance guidelines, and the potential overlap with CE, even in adequately immunocompetent or virologically suppressed hosts, this case offers an opportunity to refine practical strategies in diagnosis, management, and follow-up.
Case presentation
A 57-year-old man with HIV-1 diagnosed in 2008 (consistently virologically suppressed) had longstanding reflux symptoms beginning in 2016. He also had intermittent episodes of esophageal candidiasis over the years and comorbidities, including cleared hepatitis B infection, gastroesophageal reflux disease, irritable bowel syndrome, steatotic liver disease with a normal FibroScan in 2017, psoriasis, chronic obstructive pulmonary disease (COPD)/asthma, and hypertension.
The patient was not receiving systemic corticosteroids, inhaled corticosteroids, biologic agents, or any form of immunosuppressive therapy. His COPD/asthma was managed only with an as-needed salbutamol inhaler. His psoriasis was mild and well-controlled without systemic treatment. His antiretroviral therapy consisted of a non-boosted regimen (tenofovir disoproxil fumarate, emtricitabine, and doravirine).
In August 2019, an esophagogastroduodenoscopy (OGD) performed for symptoms of dysphagia showed esophagitis. In February 2022, a repeat OGD revealed a white patch in the mid esophagus; biopsies confirmed candidiasis, and a 14-day course of fluconazole led to symptomatic improvement.
In May 2024, he developed a recurrence of progressive dysphagia with dyspepsia and weight loss. An OGD was performed, which showed malignant-appearing, severe grade D esophagitis spanning 31-39 cm from the incisors, with a separate superficial patch at 41 cm (Figure 1).
OGD showing a malignant-appearing, exophytic, passable lesion with severe grade D esophagitis, with invasive esophageal candidiasis in the mid esophagus from 31 cm to 39 cm, and a separate superficial patch at 41 cm.(a and b) Severe grade D esophagitis and possible invasive esophageal candidiasis. (c) Malignant-appearing exophytic lesion. (d) Superficial patch at 41 cm.OGD, esophagogastroduodenoscopy
Histology showed signs of candidal infection and bacterial clusters. No dysplasia or malignancy. A computerized tomography (CT) scan of the thorax/abdomen/pelvis in May 2024 demonstrated no mass, no mediastinal or abdominal lymphadenopathy, and no sinister lesions; notably, the endoscopic lesion was not appreciable on CT. At the radiology and upper gastrointestinal (GI) multidisciplinary team (MDT) meeting later that month, high-dose PPI, a 14-day fluconazole course, empiric Helicobacter pylori eradication, and a repeat OGD were recommended.
A repeat OGD in July 2024 described a “keratectatic fungoid” 5-cm lesion at ~30 cm. The differential included esophageal papillomatosis versus keratosis (Figure 2). Histopathology ruled out papillomatosis and confirmed keratosis.
OGD showing a keratectatic/fungoid 5-cm lesion at approximately 30 cm.OGD, esophagogastroduodenoscopy
By October 2024, OGD demonstrated moderate erythematous mucosa with plaque in the lower third of the esophagus (Figure 3).
OGD showing esophageal parakeratosis with moderately erythematous mucosa and a plaque in the lower third of the esophagus.(a and b) Esophageal parakeratosis extending from 34 cm to 39 cm from the incisors, with some areas partially circumferential and causing slight luminal narrowing. (c) Moderate erythematous mucosa with a plaque in the lower third of the esophagus.OGD, esophagogastroduodenoscopy
Biopsies showed hyperkeratosis/parakeratosis and no fungal or bacterial infection or dysplasia (Figure 4). Supplementation with zinc and riboflavin (vitamin B2) was initiated alongside ongoing acid suppression.
Histopathological slides (a and b) showing prominent esophageal parakeratosis.
On February 5, 2025, OGD showed the known parakeratosis now spanning roughly 34-40 cm, covering up to ~75% of the circumference but still easily traversable, along with pangastritis; the duodenum was normal (Figure 5).
OGD showing parakeratosis spanning roughly 34-40 cm, covering up to about 75% of the circumference.OGD, esophagogastroduodenoscopy
Histology showed squamous mucosa with persistent parakeratosis in the superficial layer and no evidence of active inflammation, eosinophilic infiltration, intestinal metaplasia, dysplasia, or malignancy. Zinc and vitamin B2 were continued.
OGD in July 2025 again found the parakeratosis (32-38 cm) with easy passage and no fixed stricture (Figure 6).
OGD showing parakeratosis (32-38 cm) with easy passage and no fixed stricture.OGD, esophagogastroduodenoscopy
Histology identified mild esophagitis and Candida. He received fluconazole 100 mg once daily for 14 days; nighttime famotidine and sucralfate were added to reduce mucosal irritation. Because dysphagia persisted despite the lack of a structural narrowing, esophageal manometry was requested to assess for a motility disorder. Given repeatedly benign histology, a surveillance OGD interval was proposed, with the caveat that earlier reassessment would occur if symptoms evolved.
Discussion
In our patient, the initial endoscopic appearance of an exophytic, keratinizing, near-circumferential lesion over a long esophageal segment strongly suggested malignancy. However, multiple targeted biopsies consistently revealed hyperkeratosis/parakeratosis without dysplasia or carcinoma. This underscores a critical principle: in suspicious esophageal lesions without a mass on imaging, repeated histologic sampling is essential to avoid premature oncologic intervention.
The linkage of parakeratosis to micronutrient deficiency finds some support in the literature. In a classic animal model, riboflavin deficiency induced marked hyperkeratosis, acanthosis, and pseudocarcinomatous changes in the esophagus, which resolved with riboflavin repletion [3]. In human intervention trials, such as the randomized study by Muñoz et al. in high-risk Chinese populations, supplementation with riboflavin, retinol, and zinc was associated with improvements in markers of esophageal cell integrity, including a reduction in micronuclei frequency; however, these studies did not specifically demonstrate regression of parakeratosis itself [7]. In addition, dietary zinc deficiency in rodent models has been shown to promote proliferative changes in esophageal squamous epithelium [8]. Thus, empiric supplementation with zinc and riboflavin in this patient is biologically plausible, especially given the benign histology, and may contribute to the regression of keratinized mucosa over time. The recurrent identification of Candida on biopsy, despite robust HIV viral suppression and a strong CD4 count, is not unprecedented.
Importantly, the patient was not receiving systemic or inhaled corticosteroids, biologics, or other immunosuppressive medications, and his psoriasis and COPD/asthma did not require therapies that would compromise immunity. Given sustained virological suppression and a strong CD4 count, he remained immunocompetent, making recurrent CE more likely related to local esophageal factors and chronic acid suppression rather than systemic immunosuppression.
In the cohort of immunocompetent patients (no overt immunodeficiency), PPI use emerged as the strongest risk factor associated with CE, with many patients previously treated for reflux [4]. In the Japanese endoscopy series, PPI use was again independently associated with CE (OR 1.69) after controlling for comorbidities [5]. In clinical practice, 63-81% of esophageal candidiasis cases are reported in patients with concurrent PPI use, reflecting a potent pharmacologic association [6]. The mechanistic rationale is plausible: sustained acid suppression may enable Candida overgrowth by altering the esophageal microenvironment, reducing acidity, and disrupting fungal control mechanisms. These findings reinforce the need for careful balancing of PPI use in patients at risk of fungal complications.
In managing CE, standard practice supports systemic azole therapy, commonly fluconazole, for 14-21 days per Infectious Diseases Society of America guidelines; recurrent disease may warrant a suppressive regimen [9]. In people with HIV, drug interactions must be considered, but in our case, moderate-duration fluconazole was feasible. His antiretroviral regimen consisted of tenofovir, emtricitabine, and doravirine, which is a non-boosted combination; therefore, clinically significant drug-drug interactions with azole antifungals such as fluconazole were not anticipated.
Because the patient’s dysphagia persisted without a fixed stricture and the scope traversed easily, an esophageal manometry is planned for the upcoming appointments, as an underlying motility disorder might magnify symptom burden. Surveillance in parakeratosis without dysplasia remains undefined. Given the large segment involved and morphological changes over time, shorter intervals (e.g., 6-12 months) seem safer until stability is documented. Serial endoscopic assessment with generous mapping biopsies remains the best available strategy in the absence of published guidelines.
Conclusions
Esophageal parakeratosis can convincingly masquerade as malignancy yet represent a benign keratinization disorder, often with potential links to micronutrient deficiency. In people with well-controlled HIV, recurrent CE can still occur, particularly with chronic PPI exposure, and should be managed with guideline-based systemic therapy while minimizing predisposing factors where feasible. This case highlights four practical principles: obtain repeated and generous biopsies before labeling a lesion malignant; consider targeted micronutrient repletion (zinc, riboflavin, and assessment of B vitamins) when parakeratosis is found; rationalize acid suppression and use mucosal protectants to mitigate Candida risk; and individualize surveillance intervals in the absence of formal guidance, with a lower threshold for shorter follow-up when lesions are extensive or morphologically dynamic. Together, these steps minimize overtreatment, prioritize patient safety, and acknowledge the current evidence gaps that warrant future prospective study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diffuse esophageal parakeratosis Endoscopy Tu CH Tai CM Chang CY Chiang TH Lee CT Lin JT 02039 Suppl 1200710.1055/s-2006-94517317440850 · doi ↗ · pubmed ↗
- 2Dysphagia resolved with vitamin B 12 therapy: a case of esophageal parakeratosis Endoscopy Kayhan B Olmez S Ozaslan E Uner E Turhan N Koseoglu T Purnak T 043201110.1055/s-0030-125628521773960 · doi ↗ · pubmed ↗
- 3The vulnerable esophagus: riboflavin deficiency and squamous cell dysplasia of the skin and the esophagus J Natl Cancer Inst Foy H Kondi A 941948721984 https://pubmed.ncbi.nlm.nih.gov/6584669/6584669 · pubmed ↗
- 4Possible risk factors for Candida esophagitis in immunocompetent individuals Gastroenterology Res Nassar Y Eljabbour T Lee H Batool A 1951991120182991562910.14740/gr 1019 w PMC 5997470 · doi ↗ · pubmed ↗
- 5Risk factors for the development of esophageal candidiasis among patients in community hospital Sci Rep Ogiso H Adachi S Mabuchi M 206631120213466719810.1038/s 41598-021-00132-w PMC 8526817 · doi ↗ · pubmed ↗
- 6Course of esophageal candidiasis and outcomes of patients at a single center Clin Gastroenterol Hepatol Hoversten P Otaki F Katzka DA 2002021720192970229710.1016/j.cgh.2018.04.035 · doi ↗ · pubmed ↗
- 7Effect of riboflavin, retinol, and zinc on micronuclei of buccal mucosa and of esophagus: a randomized double-blind intervention study in China J Natl Cancer Inst Muñoz N Hayashi M Bang LJ Wahrendorf J Crespi M Bosch FX 687691791987 https://pubmed.ncbi.nlm.nih.gov/3477659/3477659 · pubmed ↗
- 8Effects of dietary zinc deficiency on esophageal squamous cell proliferation and the mechanisms involved World J Gastrointest Oncol Chen Y Liu FX Liu H 175517651320213485364810.4251/wjgo.v 13.i 11.1755 PMC 8603456 · doi ↗ · pubmed ↗