Impacts of continuing education for health professionals in primary health care: A scoping review
Laianny Krizia Maia Pereira, José Adailton da Silva, Eva Emanuela L. Cavalcante Feitosa, Alexandre R. Caitano, Janaína Luana R. da Silva Valentim, Manoel Honorio Romão, Natalia Araújo do N. Batista, Lyane Ramalho Cortez, Karilany Dantas Coutinho, Aline de Pinho Dias

TL;DR
This review examines the impact of continuing education for health professionals in Brazil's primary health care system, finding it beneficial for training and service quality, though more research is needed on long-term health outcomes.
Contribution
The study provides a scoping review of CHE impacts in Brazil's PHC, highlighting gaps in evaluating long-term health outcomes and the potential of technology-mediated training.
Findings
Most CHE actions were in-person, though online and hybrid methods are increasing.
CHE positively affects professional practice and service quality, but health outcome impacts are under-researched.
Flexible training strategies can improve access to education and align with SDGs.
Abstract
Continuing Health Education (CHE) is an essential strategy for the continuous qualification of Primary Health Care (PHC) professionals, promoting knowledge updating and improving the quality of services. In Brazil, this process is especially relevant given the challenges faced by the Unified Health System (SUS) and the need for training aligned with local demands. Understanding the impact of CHE actions in PHC is crucial to identify their effects on professional practice and health outcomes. To identify and analyze the evidence on the impacts of CHE for health professionals in the context of Primary Health Care in Brazil. This is a scoping review conducted according to the Joanna Briggs Institute (JBI) guidelines and reported based on the PRISMA-ScR checklist. The search was performed in MEDLINE/PubMed, SciELO, LILACS, EMBASE, and Web of Science, and in gray literature through Google…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
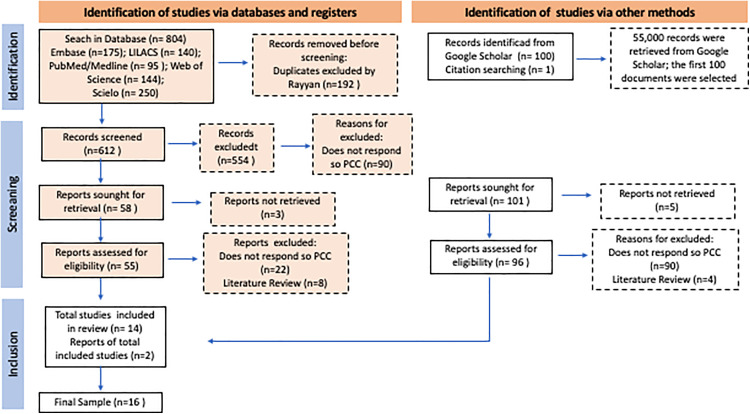 Fig 1
Fig 1- —Brazilian Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth, Nursing, Elderly Care · Phytochemistry Medicinal Plant Applications · Male Reproductive Health Studies
The protocol for this review was registered with the Open Science Framework (OSF) under DOI [https://doi.org/10.17605/OSF.IO/784ED] – available at https://osf.io/784ed/.
1. Introduction
Continuing Health Education (CHE) in the Brazilian National Health System (SUS) requires significant efforts to promote and coordinate health services, educational institutions, and the work environment [1]. These efforts are particularly challenging due to the country’s territorial extension, cultural diversity, and regional asymmetries, as well as the large number of health workers—over four million—and approximately one hundred thousand health establishments opera`ting continuously [2]. Despite the progress made, challenges remain, including the need to further encourage the use of new educational technologies in the training of health professionals and to address the growing demands of public health.
In an attempt to respond to the constant need for training and updating professionals, in 2004, the Brazilian Ministry of Health proposed the National Policy for Continuing Education in Health (PNEPS) [3–5]. This initiative seeks to promote advances in health work, especially in the training of human resources, by restructuring educational practices in the field of health [6].
It is important to highlight that, in the Brazilian context, Permanent Health Education (Educação Permanente em Saúde) goes beyond the traditional concept of continuing education. It is a political-pedagogical approach that integrates education, healthcare services, and management, aiming to transform health practices based on the concrete needs of each territory [5].
The policy is based on activities that are part of everyday work and the realities experienced by professionals, using reflection on practice as a tool for qualifying and solving problems faced on a daily basis [7–9]. With the creation of the Policy, continuing education began to play a central role in the construction of knowledge and in the transformation of training and assistance processes [10].
Primary Health Care (PHC), recognized as the main gateway to the SUS, plays a strategic role in promoting health, preventing diseases, and managing comprehensive care, being capable of solving around 85% of the population’s health problems [11–13]. However, for this level of care to effectively achieve its objectives, it is essential that professionals are continually trained to deal with the challenges imposed by epidemiological, social, and technological changes [14].
In the context of PHC, continuing education stands out as an approach that incorporates the principles of problematization, contextualization of reality, innovative pedagogies, and reflective thinking [14]. In this way, it guarantees the updating of knowledge and the improvement of health workers’ skills, directly impacting the quality of the services provided [15]. In addition, by focusing on the problems that emerge from the daily lives of health teams, Continuing Health Education has promoted changes in the reality of the population in the territories [5,8,16,17].
Although Continuing Health Education (CHE) is essential for the qualification of health professionals, studies indicate that the evaluation and monitoring of CHE actions are still insufficient [18,19]. Furthermore, even with its great potential to impact the quality of care, there is still a gap in the literature regarding the real effects of CHE on improving care practice in PHC. In this context, there is a need to monitor and measure the effects of the actions implemented, as well as the impact of training processes on the provision of health services and on meeting the targets of the Sustainable Development Goals (SDGs) of the United Nations (UN) 2030 Agenda [20,21].
Thus, this study aims to identify and analyze evidence on the impact of Continuing Health Education for health professionals in PHC in Brazil. Specifically, this scoping review seeks to map the thematic areas addressed, the methodological strategies employed, and the indicators used to measure their impacts, contributing to the improvement of continuing education policies and practices in the country.
2. Materials and methods
This study was pre-registered in the Open Science Framework (OSF) under DOI [https://doi.org/10.17605/OSF.IO/784ED] (available at https://osf.io/784ed/).
This is a scoping review that aims to answer research questions, based on a rigorous, transparent and reliable synthesis of knowledge, guided by the methodology proposed by the Joanna Briggs Institute – JBI [22] and its reporting was guided by the Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [23] to ensure transparency and methodological rigor.
The choice of this method is based on the need for a broad mapping of the literature on the subject. The methodological design of this study consists of six consecutive stages, as described in the previously published research protocol [24]: (1) define of the objectives and scope of the review; (2) identifying search terms; (3) establishing inclusion and exclusion criteria; (4) extracting data; (5) analyzing the results; and (6) presenting the findings.
It is important to note that this study did not directly involve human participants, and ethical approval was not required.
2.1. Step 1: Define of the objectives and scope of the review
Considering the objective of this study, it was structured according to the PCC mnemonic – (Population – health professionals; Concept – continuing education; Context – primary health care).
Thus, the general objective of this scoping review was to identify evidence on the impacts of CHE initiatives directed toward health professionals working in Primary Health Care. Specifically, the review aimed: (1) to map the thematic areas addressed in CHE initiatives for PHC professionals; (2) to describe the methodological strategies used in CHE activities within the PHC context; and (3) to identify the work process and health outcome indicators used to measure the impacts of these educational strategies.
2.2. Step 2 – Choosing search terms
The search strategies were designed according to each database, following keywords from three controlled health vocabularies (DeCS, MeSH, and Emtree), together with Boolean operators to obtain a broader result. Non-controlled words were also used to increase the sensitivity of the strategy. Articles identified in the references of the studies selected by the searches carried out and which are related to the objective of this review could be included.
The databases included in this study were MEDLINE (via PubMed), SciELO, LILACS, Embase, and Web of Science. The selection of these databases was justified by their high credibility, as they index journals of recognized academic reputation and are widely used as references for scientific research in the field. Google Scholar was also considered for the analysis of the first 100 documents retrieved, which were evaluated as potential sources of gray literature relevant to the objectives of this review. The literature searches were conducted in June 2024.
The complete search strategy, including all keywords, descriptors, and Boolean combinations used for each database, is available in Supplementary File 2.
The literature searches were conducted by one of the authors (LKMP)
2.3. Stage 3 – Definition of inclusion/exclusion criteria
The inclusion and exclusion criteria were structured according to the PCC framework: Population (P) – health professionals; Concept (C) – continuing education; and Context (C) – primary health care (PHC).
We chose to include publications from primary studies and gray literature: books, manuals, protocols, short communications, dissertations, and theses, which deal with continuing education for health professionals in PHC in Brazil, and which answer the question of the study. The survey included papers available in full and in electronic format, without language limitations, and published between 2007 and 2024. Duplicate publications, letters to the editor, expanded abstracts, editorials, and articles that were unavailable even after contacting the authors were excluded.
2.4. Step 4 – Data extraction
The process of selecting studies was guided by the path proposed in the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA-ScR) [23]. The Rayyan management software (Rayyan Systems Inc., Doha, Qatar) was used as a tool to support the selection of studies. Two independent reviewers (LKMP and EELCF) conducted the screening in two sequential stages: (1) title and abstract screening and (2) full-text review, both against the predefined inclusion/exclusion criteria.
The studies selected by title and abstract were retrieved in full and exported to a database in the Microsoft Excel® program. Discrepancies between the two reviewers at any stage were discussed, and when consensus could not be reached, a third reviewer (JAS) acted as arbiter. The paired review ensured the relevance of the studies and took place from July to September 2024.
After reading the full texts and validating the final sample, an assessment of the compatibility and relevance of the evidence with the aim of the review was performed.
A flowchart (Fig 1) was drawn up containing information on the screening and selection of studies included and excluded from this scoping review. Data extraction was performed independently by two reviewers (LKMP and EELCF) using a structured form developed by the authors, as presented in the published protocol [24]. The form included the following fields: publication title, authors, year of publication, country, language, study design, study population, study objectives, addressed themes, methodology used, and indicators of work process and health outcomes. Any discrepancies identified between the reviewers were discussed and resolved by consensus, with no need for third reviewer intervention.
Selection of sources of evidence (adapted PRISMA 2020). Source: Research data, 2024.
It is worth noting that a pilot test was conducted before starting the study selection and data extraction to ensure alignment of the procedures. Both reviewers independently evaluated a random sample of 25 articles, assessing titles and abstracts according to the eligibility criteria. Afterwards, they met to discuss and resolve discrepancies and make the necessary adjustments to the criteria and definitions. Data extraction began only when 75% or more similarity was achieved between reviewers, ensuring methodological consistency and reliability.
2.5. Stage 5 – Analysis of the results
The mapped studies were analyzed descriptively, using the information described on the form used to extract the data and other characteristics considered relevant to the findings. The results of the studies were categorized into three analysis groups: a) topics covered; b) methodologies used; c) work process and/or health outcome indicators used to measure impact.
2.5. Stage 6 – Presentation of results
The results of the research are presented in a flowchart (Fig 1) and tables (Tables 1 and 2). The results were presented to experts in the field and analyzed in the light of the relevant literature in order to qualify the preliminary findings.
Table 1: Characterization of the studies included in the scoping review.
Table 2: Thematic areas, methodological strategies, and indicators of work process and health outcomes identified in the included studies.
3. Results
The initial database search yielded 804 records while an additional 101 records were identified through other methods, including 100 from the gray literature and 1 through citation searching.
A total of 192 duplicate records were removed from the study. Subsequently, a screening process was carried out, considering all records retrieved from both databases and other sources. During this stage, eight studies were excluded because their full texts were not available. Among the remaining exclusions, 112 publications did not meet the PCC criteria, and 12 were literature reviews. It should be noted that one article [25], related to the aim of this review, was included from the references of a study [26] selected in the searches. In total, 16 documents were included in the final sample, comprising 15 scientific articles and 1 doctoral thesis [27]. The search results and the study selection process are summarized in Fig 1.
The characterization of the studies included in the scoping review, according to author, year, title, objective, type of study, approach, study population, as well as the main results of the studies are shown in Table 1.
The mapping of the sources that make up the results of this study showed that of the total of 16 documents, 56% (9) were publications from the period 2007–2019 [25, 27, 29, 31 - 33, 36 - 38] and 44% (7) were publications from the last 5 years (2020–2024) [26, 28, 30, 34, 35, 39, 40].
Although the highest percentage of evidence was obtained before the last five years, interest in studying the impact of health professionals’ CHE actions in PHC has increased, especially in recent years.
We identified three intervention-type studies [29, 32, 33, 34], three analytical studies [38–40], one case study [27], one cross-sectional study [28], one exploratory-descriptive study [30], two quasi-experimental studies [31,35], two ecological studies [25, 26], one prospective study [37] and one action research study [36]. As for the methodological approach used, eleven studies were quantitative [25, 26, 28, 29, 31, 33, 35, 37 - 40], four were qualitative [27, 32, 34, 36], and one was mixed [30].
With regard to the population of the studies, it was possible to identify in the findings the participation of various categories of health professionals working in PHC [25,26,34,36-40], such as Biomedical, Dental Surgeon, Nurse, Pharmacist, Physiotherapist, Physician, and Nutritionist. Other studies were aimed more at university-educated professionals who make up the minimum team of the Family Health Strategy (eSF), namely doctors, nurses, and dentists [27-30,35]. The studies by Lazarini and Barbosa [31] and Amaral et al [33] also included technical (nursing technicians) and medium-level (community health workers) professionals.
With regard to the CHE actions described in the selected studies, the mapping of published information was categorized according to the thematic areas covered, the methodological strategies used, and the work process and health outcome indicators used to measure the impact of the training strategy, as described in Table 2.
Based on the publications analyzed, the thematic areas covered in continuing education actions for health professionals in PHC include: family health [25 - 27, 32], oral mucosa lesions [28, 35], care for adults with disabilities [29], medicinal plants and herbal medicines [30], syphilis and/or other STIs [31, 40], cervical cancer [33], child development [34, 37], health education for the elderly [36], and suicide prevention [38]. The study by Ricardo et al [39] covers various subject areas in courses offered in a virtual learning environment.
Among the studies selected in this review, the majority (n = 9) deal with educational actions implemented through face-to-face modality [27, 28, 30, 31, 33, 34, 36-38], using methodological strategies such as: oral presentations, workshops, and presentation of clinical cases. In addition, distance learning actions were identified in six studies [25, 26, 35, 39, 40]. The study by Balogt and colleagues [29] presented an intervention with a hybrid approach, combining a technology-mediated course and two face-to-face workshops as methodological strategies. Mattos, Dahmer, and Magalhães [32] carried out a study based on a face-to-face educational process and a technology-mediated one.
To measure the impact of CHE actions, the studies analyzed adopted different measures. Eleven studies used exclusively work process indicators [27, 29 30,32 - 39], while three studies focused on health outcome indicators [25, 26, 40]. Two studies used work process and health outcome indicators, seeking a more comprehensive assessment of the impact of Continuing Education on health services [28, 31]. Among the analyzed studies, process indicators were predominant, reflecting changes in professional practice and organization of work. In contrast, health outcome indicators, such as those related to maternal and child health or disease prevention, were less commonly evaluated.
4. Discussion
This review presents us with a comprehensive mapping of CHE actions aimed at PHC professionals in Brazil. The study highlights the various thematic areas, methodological strategies and impact indicators used, which provides a broad view of how CHE is being implemented and evaluated in the context of PHC. In addition, the review identifies emerging trends, such as the growing use of technology-mediated teaching, and highlights gaps and opportunities for future research, especially in relation to direct impacts on the population’s health outcomes.
The analysis revealed that Continuing Education in Health has an impact on work processes in Primary Health Care, mainly in terms of qualification and updating knowledge, demonstrated by the predominance of studies that evaluated the effects and impacts on work processes and found positive results [27, 29, 30, 32–39]. It was observed that these processes were evaluated on the basis of changes in professional practice following continuing education.
Most of these studies followed this approach, and carried out measurements before and after educational actions to identify changes in performance or professional practices, such as the study by Cardoso et al [35], which applied a pre-test and post-test for dental surgeons after a 3-month online course on the diagnosis and management of oral lesions in Primary Health Care. The study showed that the classification of the nature of the lesions, diagnostic hypotheses, sensitivity, and specificity improved by 13.4%, 10.0%, 13.4%, and 6.6%, respectively [35].
The perception of professionals was also used as a parameter to measure the impact of continuing education processes. In the research carried out by Mattos; Dahmer and Magalhães [32], according to the perception of doctors, dentists and nurses, after the training process focused on Family Health, there was a reorganization of the team’s work process, implementation of collective activities and reception of spontaneous demand, as well as a greater understanding of the work process.
It is important to note that the literature emphasizes how health professionals are not always trained to approach the health-disease process with a comprehensive and integrated perspective. This limitation often results in fragmented and low-resolution practices, which can reduce the effectiveness of outcomes in Primary Health Care [41].
From the studies reviewed, it was observed that the measurement of health outcomes as an evaluation of Continuing Health Education processes is still incipient, and is an area that needs greater attention in future research [42,43]. This contrasts with the predominance of work process indicators found in most studies, which assess immediate changes in professional practice and service organization. Such distinction helps to contextualize how CHE has been measured in Brazil, emphasizing the gap in evaluating long-term health results.
According to the literature, the evaluation processes of Continuing Education in Health are still poorly implemented in Brazil [44]. In general, these initiatives are isolated and occasional, although they play an important role in health policy by enabling the measurement of an intervention’s degree of implementation, its effects, and impacts [45]. In this sense, monitoring and evaluating continuing education actions is both a major shortcoming and a major necessity for strengthening the National Policy for Continuing Education in Health and, consequently, for consolidating the SUS [46].
The use of health indicators is one of the main evaluation measures in public health, qualifying services and allowing for the analysis of the population’s life process. It is essential, among other factors, for demonstrating the impact of interventions on the population’s health, as well as evaluating subjective concepts such as care and access [47]. In this context, the incorporation of results indicators in the evaluation of CHE practices not only makes it possible to measure the improvement of work processes but also provides robust data for decision-making and the allocation of resources in health management.
The relationship between CHE and the monitoring of health indicators is an indispensable complementary strategy for boosting the impact of actions in PHC, as we can see in the studies that measured impact based on health outcomes. Nascimento and collaborators [26] investigated whether taking a specialization course in Family Health, in the online modality, was associated with an improvement in care and maternal and child health indicators. They used parameters such as the monitoring of pregnant women, children breastfed for up to 4 months, preventive examinations for cancer and cervical cancer, as well as the diagnosis of new cases of the disease. The results show that the training had a visible impact on the CHE process, with better indicators related to maternal and child health [26].
The study by Santos and collaborators [25], In 2019, analyzed the impact of a specialization course in Family Health, focusing on the insertion of qualified professionals and its relationship with hospitalization rates for primary care-sensitive conditions, in addition to the monitoring of chronic conditions in a municipality. The results indicated a reduction in the overall and specific rates of hospitalizations for primary care-sensitive conditions (including asthma, gastroenteritis, and heart failure) over the period studied, especially in areas with a high or intermediate proportion of professionals who had completed specialization. Similarly, there was an improvement in monitoring indicators for chronic conditions such as diabetes and hypertension, with greater registration, follow-up, and group care for these patients [25].
The study by Caitano et al [40], published In 2022, analyzed the impact of a training course on syphilis and other sexually transmitted infections. The study focused on evaluating the results of this training process in the management and prevention of these diseases based on epidemiological data and the number of tests. It was found that, as the number of children enrolled increased from 2018 onwards, vertical transmission of syphilis began to fall. This positive impact on vertical transmission rates indicates resilience and responsiveness due to changes in the work processes of the Brazilian National Health System (SUS) [14].
The thematic areas covered by the Continuing Health Education (CHE) actions are diverse, ranging from general aspects of Family Health to more specific topics, such as oral mucosal lesions, care for people with disabilities, suicide prevention, and health education for the elderly. This variety of topics highlights the flexibility of continuing education, which adjusts to local needs and the demand for specialized training within Primary Health Care, considered a dynamic and complex health scenario [48]. According to Ferreira (2019) [49], CHE has the work process as the object of transformation in the practice scenario, based on the professionals’ critical reflection on what is happening in the daily routine of the services and seeking solutions to the problems encountered together with the team.
The studies analyzed showed that the methodological strategies used are predominantly face-to-face. However, the use of technology-mediated teaching has intensified in recent years, which reflects the need for more flexible strategies that show promise for expanding the reach and effectiveness of training processes [50, 51]. The study by Ricardo Valentim and collaborators (2022) [39] evaluated the impact of online educational offers on health services and the professional practice of course participants. The results indicated that 76.2% of the study participants recommended the courses, and 81.3% of these recommendations were motivated by the quality of the course. In addition, 75.6% of respondents indicated that the content of the courses contributed to improving health services in the health establishments where they work.
The adoption of hybrid approaches, combining face-to-face teaching with technology-mediated teaching, also proved to be a viable alternative. It was observed that face-to-face activities, with workshops preceded by online activities in virtual environments, was the main association adopted in a training process, which had a positive impact, promoting changes in professionals’ perceptions and practices about child development in primary care settings [29].
The growing use of technology-mediated education and digital tools in Continuing Health Education is in line with the evolution of digital health [52], which seeks to integrate technologies to improve the quality and efficiency of health services. The use of digital platforms allows health professionals to access educational content more flexibly, overcoming geographical and time barriers [51, 53].
Regarding health professionals, the findings of this review also show that Continuing Health Education in PHC has a significant reach, as it involves professionals from different categories [54, 55]. In addition, the inclusion of nursing technicians and Community Health Agents (CHAs) in educational actions highlights an advance in valuing these professionals, who play a crucial role in promoting health and monitoring the population, particularly in Brazil, where there is an appreciation of the participation of these two professionals in PHC.
This diversity reflects the need for interdisciplinary training that favours integration between professionals and improves teamwork, an essential factor in guaranteeing quality care in PHC [56, 57]. Continuing Health Education strategies that promote collaboration between different areas of knowledge increase the problem-solving capacity of services and strengthen user-centred care [58].
Mendes [12] already confirmed these findings in 2012 by demonstrating the positive impact of multiprofessional teamwork on various dimensions of PHC practice: on user experiences; on the professional development of health team members; on the quality of care and health outcomes; on the utilization of health resources; and on provider satisfaction. In this context, considering that professionals do not arrive fully prepared from their training institutions and require continuous in-service education, it becomes essential to implement a culture of collaborative and humanized practice in PHC.
When reflecting on the findings of this review, it is evident that Continuing Health Education appears to contribute to transforming work processes and may favor improvements in health outcomes, in alignment with the principles promoted by the Sustainable Development Goals (SDGs) — particularly SDG 3 (Good Health and Well-being), SDG 4 (Quality Education), SDG 8 (Decent Work and Economic Growth), and SDG 10 (Reduced Inequalities) [59,60].
The findings reinforce the relevance of expanding training opportunities, especially through technological mediation and hybrid approaches, which seem to facilitate broader access to education for professionals in different regions and contexts [59–61]. Such strategies support the strengthening of Primary Health Care and the promotion of equity in the professional qualification process, contributing indirectly to the advancement of the 2030 Agenda.
Therefore, investing in Continuing Health Education may be considered a structuring component in the qualification of the health workforce, contributing to improved performance of health services and to the sustainability of health systems, particularly within the Brazilian context.
Although the findings of this review provide relevant insights into Continuing Education in PHC, some limitations should be considered. The selection of studies was restricted to the selected sources, which may have excluded relevant publications outside these sources. In addition, most of the studies analyzed focused on work process indicators, without a more in-depth assessment of health outcomes, which limits the understanding of the real impact of Continuing Education in Health in primary health care.
This review advances current knowledge by providing an updated and comparative synthesis of Brazilian evidence on the impacts of Continuing Health Education. It highlights persistent gaps in measuring health outcomes and in the methodological approaches used in national studies.
5. Implications for practice, policy, and future research
His scoping review offers relevant contributions by synthesizing national evidence on the impacts of Continuing Health Education (CHE) in Primary Health Care (PHC) in Brazil. The findings demonstrate that CHE initiatives predominantly influence work process indicators, such as changes in professional practices, organization of services, and adherence to protocols, while the evaluation of health outcome indicators remains limited.
From a practical and managerial perspective, these results highlight the importance of structuring continuing education programs that are closely aligned with daily work processes in PHC, fostering reflective practice and team-based organization. For policymakers, the findings reinforce the need to strengthen evaluation strategies within the National Policy for Continuing Health Education, incorporating health outcome indicators to better assess the effectiveness and sustainability of educational interventions.
Regarding future research, this review underscores the need for studies that adopt more robust and longitudinal designs, capable of linking continuing education initiatives to measurable health outcomes. Advancing this agenda may contribute to more evidence-informed decision-making and to the development of more effective continuing education strategies in Primary Health Care.
6. Conclusion
Continuing Health Education in Primary Health Care in Brazil has addressed several thematic areas, and its effects have been observed especially in changes in work processes. The findings of this scoping review indicate that most studies focus on process indicators, such as adherence to protocols and changes in professional practices, revealing a persistent gap in the assessment of impacts on health outcomes. Only a limited number of studies evaluated clinical outcomes, such as reductions in syphilis reporting or hospitalizations for primary care-sensitive conditions
Another relevant aspect identified was the predominance of in-person methodological strategies, although the growing adoption of technology-mediated and hybrid approaches in recent years signals an important transformation in continuing education practices. This movement reflects broader advances in digital health and highlights new possibilities for expanding access to professional training.
Overall, this review reinforces the relevance of Continuing Health Education as a strategic component for strengthening Primary Health Care in Brazil, while also emphasizing the need for more robust and comprehensive evaluation approaches. Future studies should prioritize the integration of process and outcome indicators in order to better capture the long-term effects of continuing education initiatives on health systems and population health.
Supporting information
S1 AppendixPRISMA.(PDF)
S2 FileFull Search Strategy for Databases and Gray Literature.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brasil. Política Nacional de Educação Permanente em Saúde: o que se tem produzido para o seu fortalecimento?. 2018. http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_educacao_permanente_saude_fortalecimento.pdf
- 2Fonseca EN Rd, Cunha SM Rd AS, Carneiro MTD, Barbosa KK da S, Batista M da C, Ferreira FCR, et al. Educação permanente em saúde: desafios e potencialidades para o processo de trabalho. REAS. 2023;23(7):e 13480.
- 3Brasil. Ministério da Saúde (MS). Portaria GM/MS nº 1.996, de 20 de agosto de 2007. Dispõe sobre as diretrizes para a implementação da Política Nacional de Educação Permanente em Saúde. Diário Oficial da União. 2007. https://bvsms.saude.gov.br/bvs/saudelegis/gm/2007/prt 1996_20_08_2007.html
- 4Ferreira L, Barbosa JS de A, Esposti CDD, Cruz M Mda. Educação Permanente em Saúde na atenção primária: uma revisão integrativa da literatura. Saúde debate. 2019;43(120):223–39. doi: 10.1590/0103-1104201912017 · doi ↗
- 5Ceccim RB, Feuerwerker LCM. O quadrilátero da formação para a área da saúde: ensino, gestão, atenção e controle social. Physis. 2004;14(1):41–65. doi: 10.1590/s 0103-73312004000100004 · doi ↗
- 6Ceccim RB. Educação Permanente em Saúde: desafio ambicioso e necessário. Interface (Botucatu). 2005;9(16):161–8. doi: 10.1590/s 1414-32832005000100013 · doi ↗
- 7Campos KFC, Sena R Rde, Silva KL. Permanent professional education in healthcare services. Esc Anna Nery. 2017;21(4). doi: 10.1590/2177-9465-ean-2016-0317 · doi ↗
- 8Gonçalves CB, Pinto IC de M, França T, Teixeira CF. A retomada do processo de implementação da Política Nacional de Educação Permanente em Saúde no Brasil. Saúde debate. 2019;43(spe 1):12–23. doi: 10.1590/0103-11042019 s 101 · doi ↗