Telephone Administration of the Human Activity Profile Questionnaire in Patients With Cardiovascular Disease: Methodological Study
Tamara Costabile Sant´Anna, Júlia Isaac Bernardes, Adriana Marques Alcici Moreira, Janaine Cunha Polese, Maria Da Glória Rodrigues-Machado

TL;DR
This study shows that the HAP questionnaire can be reliably administered by phone to assess cardiovascular patients' functional capacity.
Contribution
Validates telephone administration of the HAP questionnaire for cardiovascular disease patients, a novel remote assessment method.
Findings
Telephone-administered HAP showed high reliability and strong agreement with face-to-face administration.
Internal consistency was excellent (Cronbach α=0.919) and test-retest reliability was high for both MAS and AAS.
Abstract
The Human Activity Profile (HAP) questionnaire is widely used to assess functional capacity in patients with chronic diseases. However, its remote administration via telephone has not been validated in individuals with cardiovascular disease (CVD), despite the increasing need for accessible assessment methods, particularly in contexts involving mobility limitations or reduced access to in-person care. We aimed to validate administration of the HAP questionnaire via telephone in patients with CVD who were participating in a cardiovascular rehabilitation program. This methodological study included 56 patients with CVD (36/56, 64% men; mean age 75.14, SD 10.28 years). Participants completed the HAP twice, once face-to-face and once by telephone, with a 3- to 14-day interval. Maximum activity score (MAS) and adjusted activity score (AAS) were analyzed. Internal consistency was assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
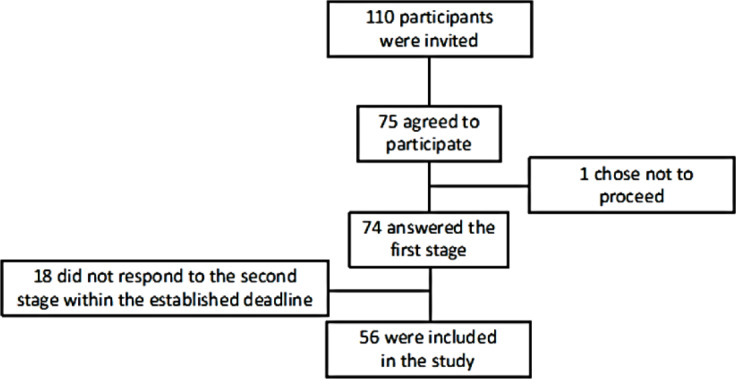 Figure 1
Figure 1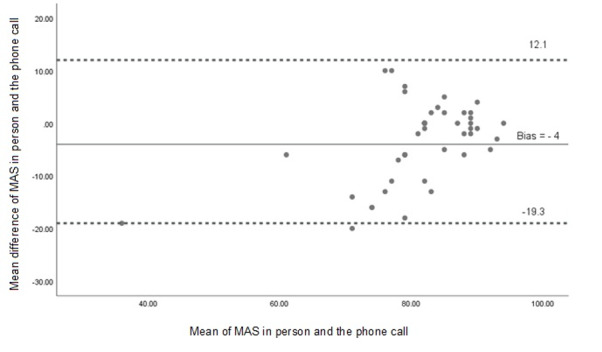 Figure 2
Figure 2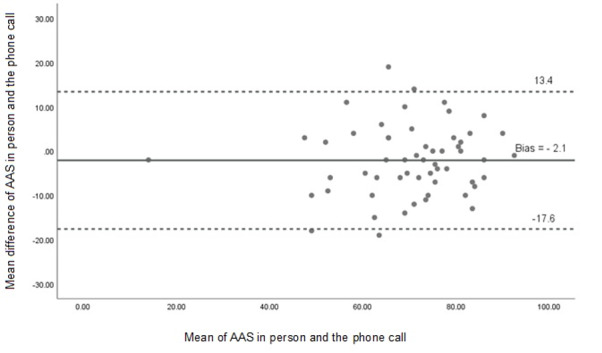 Figure 3
Figure 3| Variables | Sample |
|---|---|
| Sex (male), n (%) | 36 (64) |
| Age (years), mean (SD) | 75.14 (10.28) |
| Weight (kg), mean (SD) | 73.02 (13.64) |
| Height (cm), mean (SD) | 165.29 (10.11) |
| BMI (kg/m²), mean (SD) | 26.65 (3.97) |
| Medication use, n (%) | |
| Antihypertensives | 48 (86) |
| Statins | 44 (79) |
| Beta blockers | 26 (47) |
| Anticoagulants | 22 (39) |
| Antiglycemic agents | 12 (22) |
| Cardiovascular diagnosis, n (%) | |
| Coronary artery disease | 31 (55) |
| Arrhythmia | 15 (27) |
| Acute myocardial infarction | 7 (13) |
| Valvulopathy | 3 (5) |
| Congestive heart failure | 2 (4) |
| Comorbidities, n (%) | |
| Dyslipidemia | 55 (98) |
| Systemic arterial hypertension | 54 (96) |
| Obesity | 13 (23) |
| Diabetes mellitus | 11 (19) |
| Chronic kidney disease | 2 (4) |
| Stroke | 1 (2) |
| Procedure or surgery performed, n (%) | |
| Stent placement | 15 (27) |
| Coronary artery bypass grafting | 1 (2) |
| Score | ICC | 95% CI for ICC | Cronbach α | 95% CI for Cronbach α |
|---|---|---|---|---|
| MAS | 0.794 | 0.649‐0.879 | 0.919 | 0.879‐0.948 |
| AAS | 0.910 | 0.847‐0.947 | — | — |
| Score | Face-to-face, mean (SD) | Telephone, mean (SD) | Mean difference | |
|---|---|---|---|---|
| MAS | 79.11 (11.48) | 82.71 (7.48) | –3.61 | .10 |
| AAS | 69.11 (14.18) | 71.21 (13.43) | –2.11 | .05 |
| Category | Face-to-face | Telephone | ||
|---|---|---|---|---|
| Frequency, n (%) | Mean AAS (SD) | Frequency, n (%) | Mean AAS (SD) | |
| Inactive | 7 (12.5) | 42.42 (6.33) | 4 (7.1) | 40.75 (10.05) |
| Moderately active | 24 (42.9) | 64.68 (5.89) | 24 (42.9) | 64.87 6.42) |
| Active | 25 (44.6) | 80.33 (4.72) | 28 (50.0) | 81.00 (5.22) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Cardiac Health and Mental Health · Cardiovascular and exercise physiology
Introduction
Despite a sustained decline in cardiovascular disease (CVD) morbidity and mortality over the past 4 decades, CVD remains a leading cause of disease burden worldwide [1-3]. Nearly 80% of CVDs occur in low- and middle-income countries, where aging and urbanization trends have accelerated the increase in the burden of CVD [4].
Functional capacity assessment is an important part of clinical evaluation, especially in patients with chronic conditions such as heart failure, lung disease, neuromuscular disease, and other conditions that may affect functionality [35-8undefinedundefinedundefined]. Maximal exercise tests are widely used in functional capacity assessment, but the high cost may limit their use. Thus, a possible alternative is the application of scales and questionnaires that constitute relatively simple and economical tools, do not require sophisticated equipment or specialized environments to be administered, and are more accessible to a greater number of patients [8].
The Human Activity Profile (HAP) is a simple questionnaire designed to assess functional capacity in relation to daily activities and physical fitness and can offer a more accessible, convenient, and cost-effective approach to assessment [9]. The HAP questionnaire quantifies functional capacity individually, providing relevant information about physical well-being and supporting strategies to promote active lifestyles and monitor disease progression [1011].
The HAP questionnaire has demonstrated validity in cardiovascular populations and has been used alongside reference measures such as cardiopulmonary exercise testing that is considered the gold standard for assessing functional capacity, as well as with the 6-Minute Walk Test, which is widely applied in clinical settings, showing good correlation with functional capacity [1011]. In populations with Chagas cardiomyopathy and heart failure, the HAP questionnaire has been associated with measures such as functional class and systolic function, reinforcing its clinical relevance in characterizing functional limitations in CVD [12]. Additionally, its application has proven reliable across diverse clinical settings, including hospitalized and community-dwelling older adults [91314].
In recent years, the application of questionnaires by telephone has gained prominence as a viable method of data collection, especially during periods requiring social distancing, such as the COVID-19 pandemic. Studies have successfully validated the use of telephone-based tools, including functional assessments such as the Duke Activity Status Index, in individuals with CVD and stroke [15-17]. Such methods facilitate rapid and remote evaluations, reducing barriers for patients with mobility limitations or restricted access to in-person care.
Therefore, applying the HAP questionnaire via telephone may represent a practical alternative for remote assessment of functional capacity in individuals with CVD.
The objective of this study is to validate the telephone administration of the HAP questionnaire in patients with CVD who were participating in a cardiovascular rehabilitation program.
Methods
Study Design
This is a methodological study designed to assess the reliability and validity of the HAP questionnaire when administered via telephone to patients with CVD. The study followed the Consensus-Based Standards for the Selection of Health Measurement Instruments guidelines [18], which recommend a minimum of 50 participants for studies assessing measurement properties such as reliability and construct validity. This sample size is considered adequate to detect moderate to high intraclass correlation coefficients (ICCs; ICC >0.70) with sufficient statistical power in validation studies.
Ethical Considerations
The study was approved by the institutional research ethics committee (number 5.456.711) and was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki. All participants provided written informed consent before inclusion in the study.
Participants
Participants were recruited from a cardiovascular rehabilitation program, and the sample was composed of patients diagnosed with CVD. A convenience sampling method was used on the basis of availability and eligibility of patients enrolled in the program during the study period.
The inclusion criteria were individuals of both sexes who were aged between 50 and 90 years and with a confirmed diagnosis of CVD. The exclusion criteria included patients with auditory or cognitive impairments that could interfere with communication during the telephone interview and those who failed to complete the second part of the questionnaire within the maximum interval of 14 days between assessments.
A total of 56 participants met the eligibility criteria and completed both the face-to-face and telephone assessments. Demographic, clinical, and pharmacological characteristics of the sample are presented in Table 1.
HAP Questionnaire
The HAP questionnaire is composed of 94 items that assess an individual’s level of physical function across domains such as self-care, work, social engagement, and physical activity. The items are ordered by increasing metabolic demand, with higher item numbers representing activities that require greater energy expenditure [911].
Participants were asked to classify each activity as one they are “still doing,” have “stopped doing,” or have “never done.” The HAP questionnaire can be applied to individuals with a wide range of functional capacities—from very low (eg, getting in and out of bed without assistance) to very high (eg, running 4.8 kilometers) [911].
The questionnaire generates 2 primary scores:
Maximum activity score (MAS): the number of the most strenuous activity the participant is still performingAdjusted activity score (AAS): calculated by subtracting the number of activities the participant has “stopped doing” from the MAS, up to and including the activity with the highest score still performed
The AAS is considered a more stable estimate of the individual’s typical functional level compared to the MAS, as it adjusts for discontinued activities. According to established cutoffs, AAS values categorize individuals as: inactive (AAS<53), moderately active (AAS=53‐74), and active (AAS>74) [914].
Procedure
The HAP questionnaire was administered to each participant on 2 separate occasions: once in person and once via telephone. The interval between the two assessments ranged from 3 to 14 days (mean 8, SD 4.5 d), which was deemed appropriate to minimize recall bias while avoiding significant changes in clinical status [19].
Each participant completed both modes of administration only once, and both applications were conducted by the same trained physiotherapist who followed a standardized protocol to ensure consistency in tone, pacing, and instructions across both modalities.
The order of administration was not randomized, with all participants first completing the face-to-face assessment followed by the telephone interview. This fixed order was chosen to maximize adherence and reduce the risk of dropout, particularly among older participants, based on preliminary feasibility observations during pilot testing.
Statistical Analysis
Categorical variables were reported as absolute frequencies and percentages, whereas continuous variables were expressed as means and SDs. To evaluate convergent validity, the mean differences (MDs) between face-to-face and telephone assessments were calculated along with 95% CIs.
Cronbach α was used to assess internal consistency, with values greater than 0.70 considered acceptable. The ICC was applied to determine test-retest reliability and temporal stability of the HAP questionnaire across administration modes. The magnitude of ICC was classified as follows: very high (>0.90), high (0.70‐0.89), moderate (0.50‐0.69), low (0.26‐0.49), and very low (<0.25) [19].
To assess agreement between the two methods, the Bland-Altman method was used, comparing the mean values and the differences between in-person and telephone assessments for MAS and AAS. The upper and lower limits of agreement were calculated as MD −1.96 to +1.96 times the SD of the differences, and plotted to visualize the dispersion and potential bias.
All statistical analyses were performed using R software (version 1.0), and a significance level of 5% (P<.05) was adopted.
Results
Participants were recruited between October 10, 2022, and July 31, 2023. A total of 110 individuals were eligible, of whom 75 signed the informed consent form, and 1 participant withdrew before data collection. In total, 74 individuals completed the first phase of the study. However, 18 participants did not complete both assessments—either failing to respond to the phone call or to attend the face-to-face assessment within the required 14-day interval. Thus, 56 participants completed both modes of questionnaire administration and were included in the final analysis (Figure 1).
Flowchart of participant recruitment and inclusion in the study. The figure illustrates the recruitment process, including the number of eligible individuals, those who consented to participate, those who completed the first assessment, and those who were ultimately included in the final sample after completing both face-to-face and telephone evaluations. Reasons for exclusion—such as dropout or failure to complete the second assessment within 14 days—are also indicated.
The final sample included both men and women, with a mean age of 75.14 (SD 10.8) years. The most prevalent cardiovascular risk factors were dyslipidemia (55/56, 98.2%) and systemic arterial hypertension (54/56, 96.4%), as shown in Table 1. These characteristics reflect a clinically representative population for validation of functional assessment tools in individuals with CVD [18].
Internal consistency and temporal stability of the HAP were assessed using Cronbach α and ICC, respectively. The results demonstrated excellent internal consistency for both MAS and AAS, with Cronbach α=0.919 (95% CI 0.879‐0.948). Test-retest reliability was classified as high for MAS (ICC=0.794; 95% CI 0.649‐0.879) and very high for AAS (ICC=0.910; 95% CI 0.847‐0.947), as shown in Table 2.
There were no statistically significant differences between face-to-face and telephone applications for either MAS (P=.10) or AAS (P=.05), as shown in Table 3. This supports the equivalence of the 2 administration methods.
Agreement between modalities was further examined using Bland-Altman analysis. For MAS, the mean bias was –4.0 (95% CI –19.3 to 12.1) and –2.1 for AAS (95% CI –17.6 to 13.4), indicating acceptable agreement without systematic error, as shown in Figures23. Linear regression analysis showed nonsignificant slopes for both MAS and AAS (P>.05), confirming the absence of proportional bias.
Bland-Altman plot showing agreement between maximum activity scores (MASs) obtained through face-to-face and telephone administration of the Human Activity Profile questionnaire. The plot illustrates the mean difference between MASs obtained from face-to-face and telephone assessments, along with the 95% limits of agreement (mean difference –1.96 to +1.96 SDs), represented by dotted lines. No systematic bias was observed, and most data points lie within the limits of agreement, indicating acceptable agreement between modes.
Bland-Altman plot showing agreement between adjusted activity scores (AASs) obtained through face-to-face and telephone administration of the Human Activity Profile questionnaire. The plot displays the mean difference between AASs obtained via face-to-face and telephone assessments, along with the 95% limits of agreement (mean difference –1.96 to +1.96 SDs), indicated by dotted lines. The distribution of data points within the limits suggests acceptable agreement and no evidence of systematic bias between the 2 modes of administration.
Table 4 presents the distribution of participants across functional capacity categories (inactive, moderately active, and active) based on AASs. Results were consistent across both assessment modes, reinforcing the reproducibility of classification.
No participants scored the minimum or maximum possible values for MASs (0 or 94) or AASs (1 or 94). Therefore, no floor or ceiling effects were observed, indicating that the HAP questionnaire demonstrated adequate responsiveness in this sample.
Discussion
Principal Findings
This study demonstrated that the HAP questionnaire administered by telephone yields results highly consistent with those obtained through face-to-face application in patients with CVD. Both MASs and AASs showed no notable differences between modalities, and the instrument exhibited excellent internal consistency (Cronbach α=0.919), strong test-retest reliability (ICC=0.794 for MAS; ICC=0.910 for AAS), and acceptable agreement on Bland-Altman analysis with no systematic bias. These findings indicate that telephone administration is a valid, reliable, and practical alternative for assessing functional capacity in this population, supporting the feasibility of remote functional evaluation [10111314].
Building upon these findings, the HAP questionnaire offers additional advantages that reinforce its applicability in clinical and research settings. The questionnaire allows for quick and meaningful measurements of activity level changes, comparisons with healthy populations, and identification of activity patterns associated with medical conditions [11]. It has shown correlations with objective measures of cardiorespiratory fitness [20] and has been validated for use in various populations, such as individuals with chronic pain and knee osteoarthritis [21].
In this study, the questionnaire demonstrated good internal consistency, with a Cronbach α of 0.919, and strong reproducibility and temporal stability measured by the ICC, with MAS ICC=0.794 and AAS ICC=0.910. These findings align with previous validation studies. For example, a systematic review reported high consistency for MAS (0.76‐0.97) and AAS (0.79‐0.97), reinforcing the questionnaire’s measurement reliability [13].
The Cronbach α of 0.919 in this study is considered excellent and indicative of near-perfect reliability [22]. Similar values have been observed in previous research; one study reported a Cronbach α of 0.91 when applying the HAP questionnaire via interview in a community-dwelling older adult population [9], and another study found a Cronbach α of 0.93 in hospitalized patients [14], reinforcing the questionnaire’s internal consistency across diverse populations.
The internal consistency and temporal stability did not substantially differ between face-to-face and telephone administrations, suggesting that both methods are equally reliable. Our in-person results are consistent with previous studies; one investigation reported MAS and AAS of 71.6 and 63.6, respectively, in patients undergoing coronary artery bypass grafting [11], whereas another study observed an MAS of 79.76 and an AAS of 65.81 in patients with heart failure [10]. Importantly, this study is, to our knowledge, the first to evaluate both the internal consistency and the agreement of HAP questionnaire scores when administered in person versus by telephone.
The Bland-Altman analysis confirmed good agreement between administration methods. For MAS, the limits of agreement (95% CI) ranged from −19.3 to 12.1, and from −17.6 to 13.4 for AAS. These findings suggest that the differences between the modes are within acceptable limits, with no significant measurement bias introduced by the telephone modality. No previous studies have reported such agreement data for the HAP questionnaire using this method of comparison.
Several previous studies have successfully used telephone-based instruments in patients with CVD [1516] and in poststroke populations [1723]. For instance, one study assessed pharmacist-led telephone-based education and self-management support during the COVID-19 pandemic lockdown [1523]. Another investigation examined angina prevalence among stable outpatients with CVD using remote methods [16], and a separate validation study confirmed the reliability of the Duke Activity Status Index administration by telephone in stroke survivors [17]. Telephone administration allows for faster, more direct data collection and extends access to individuals who may be unable to attend face-to-face assessments. To our knowledge, this is the first study to validate the use of the HAP questionnaire via telephone in patients with CVD.
Strength and Limitations of the Study
The assessment of physical activity levels is a key component of both in-person and home-based exercise programs. Validating a tool like the HAP questionnaire for telephone administration broadens access to functional capacity assessment, particularly for individuals living in rural or remote areas, those with limited mobility, or patients who are unable to attend in-person sessions. This approach also facilitates multicenter research by enabling efficient and cost-effective data collection across geographically diverse populations. Additionally, traditional functional tests often require specialized equipment or trained professionals, representing a high financial burden and logistical barrier, particularly for underserved populations [24-27].
However, this study has some limitations. Certain patients may face challenges related to hearing loss, language comprehension, or cognitive deficits, which can interfere with telephone-based assessment. Moreover, the lower technological literacy commonly observed among older adults, combined with socioeconomic and ethnic disparities, may further limit the widespread applicability of telephone-based tools [28].
Conclusions
The results of this study demonstrated that the HAP questionnaire, when administered by telephone, shows adequate reliability, agreement, and internal consistency, supporting its use as a valid alternative for assessing physical activity levels in patients with CVD. These findings suggest that telephone-based administration of the HAP questionnaire may be a practical, accessible, and cost-effective tool for functional assessment in clinical and research contexts, especially when in-person evaluations are not feasible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Diseases and Injuries Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Oct 1720203961025812041222 doi 10.1016/S 0140-6736(20)30925-9Medline 33069326 PMC 7567026 · doi ↗ · pubmed ↗
- 2Ruivo J Moholdt T Abreu A Overview of Cardiac Rehabilitation following post-acute myocardial infarction in European Society of Cardiology member countries Eur J Prev Cardiol 07122023309758768 doi 10.1093/eurjpc/zwad 024Medline 36722203 · doi ↗ · pubmed ↗
- 3Writing Committee Members Virani SS Newby LK et al 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol Aug 292023829833955 doi 10.1016/j.jacc.2023.04.003Medline 37480922 · doi ↗ · pubmed ↗
- 4Li Y Cao GY Jing WZ Liu J Liu M Global trends and regional differences in incidence and mortality of cardiovascular disease, 1990-2019: findings from 2019 global burden of disease study Eur J Prev Cardiol Feb 142023303276286 doi 10.1093/eurjpc/zwac 285Medline 36458973 · doi ↗ · pubmed ↗
- 5Anderson L Sharp GA Norton RJ et al Home-based versus centre-based cardiac rehabilitation Cochrane Database Syst Rev Jun 30201766 CD 007130 doi 10.1002/14651858.CD 007130.pub 4Medline 28665511 PMC 6481471 · doi ↗ · pubmed ↗
- 6Rostagno C Gensini GF Six minute walk test: a simple and useful test to evaluate functional capacity in patients with heart failure Intern Emerg Med Sep 200833205212 doi 10.1007/s 11739-008-0130-6Medline 18299800 · doi ↗ · pubmed ↗
- 7Wijeysundera DN Pearse RM Shulman MA et al Assessment of functional capacity before major non-cardiac surgery: an international, prospective cohort study Lancet Jun 3020183911014026312640 doi 10.1016/S 0140-6736(18)31131-0Medline 30070222 · doi ↗ · pubmed ↗
- 8Ferguson M Shulman M Cardiopulmonary exercise testing and other tests of functional capacity Curr Anesthesiol Rep 20221212633 doi 10.1007/s 40140-021-00499-6Medline 34840532 PMC 8605465 · doi ↗ · pubmed ↗