Effects of probiotics on heart failure: a systematic review and meta-analysis
Zheqin Zhu, Aoli Chen, Min Wang, Huimin Zhang, Sisi Dai, Rongzhen Liu, Jianhe Liu

TL;DR
This study reviews and analyzes the effects of probiotics on heart failure, finding some benefits in cardiac function and inflammation but no impact on mortality or certain biomarkers.
Contribution
The paper provides a systematic review and meta-analysis of probiotics' effects on heart failure, offering new insights into their potential as an adjunct therapy.
Findings
Probiotics slightly improved cardiac function indicators like LVEF and LVESV.
They reduced inflammatory markers such as hs-CRP, IL-6, and TNF-α.
Probiotics had no effect on NT-proBNP, activity endurance, TMAO, or mortality.
Abstract
Heart failure (HF) is a serious clinical syndrome with substantial health threats. Emerging studies link intestinal flora dysbiosis to HF onset and progression. Although probiotics are thought to regulate gut microbiota, the specific impact of probiotics on HF remains unclear, highlighting the need for systematic evaluation. As of 9 September 2025, we searched eight major academic databases using a predefined protocol for data extraction and quality assessment. Subsequently, a meta-analysis was conducted using Review Manager 5.4 and Stata 18. Forest plots were used to analyse the effect size, and publication bias was evaluated through funnel plots. Ultimately, 11 of the studies met the inclusion criteria for the systematic review. The results showed that probiotics have a slight beneficial effect on cardiac function indicators (LVEF, LVESV), reduced the levels of inflammatory factors…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
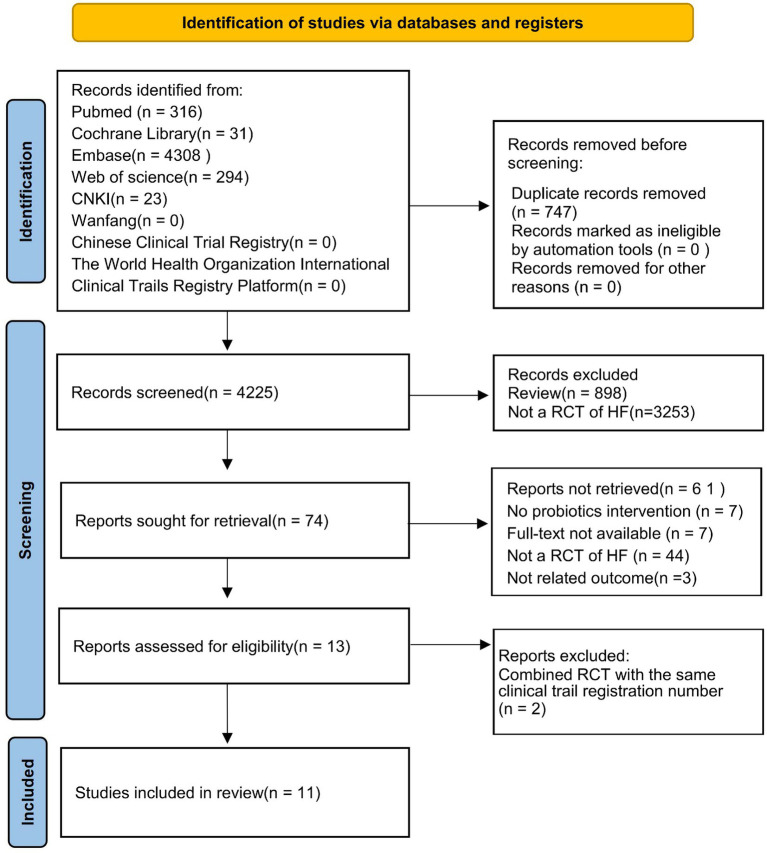 Figure 1
Figure 1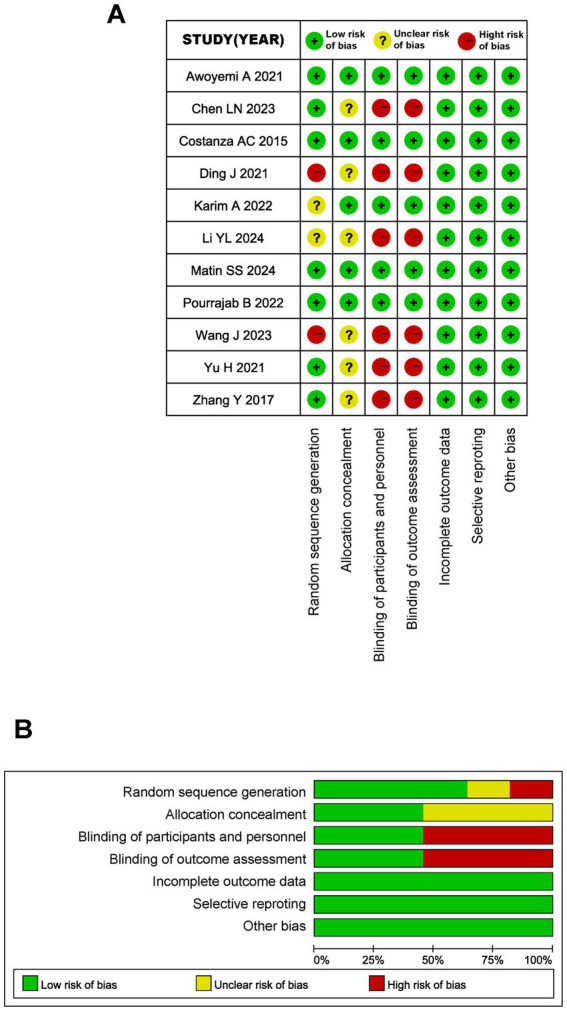 Figure 2
Figure 2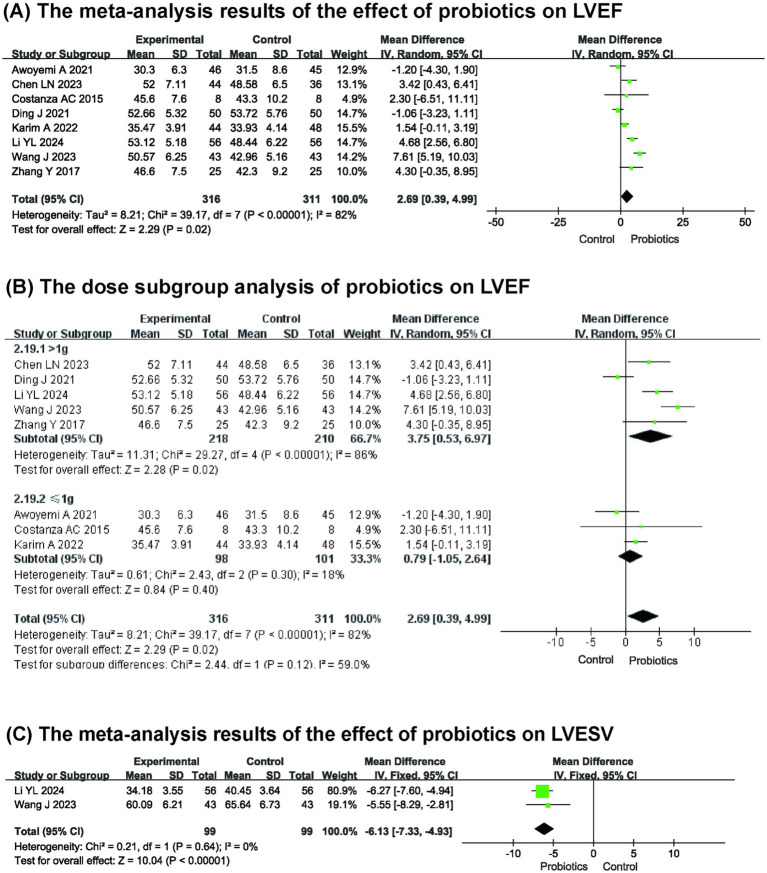 Figure 3
Figure 3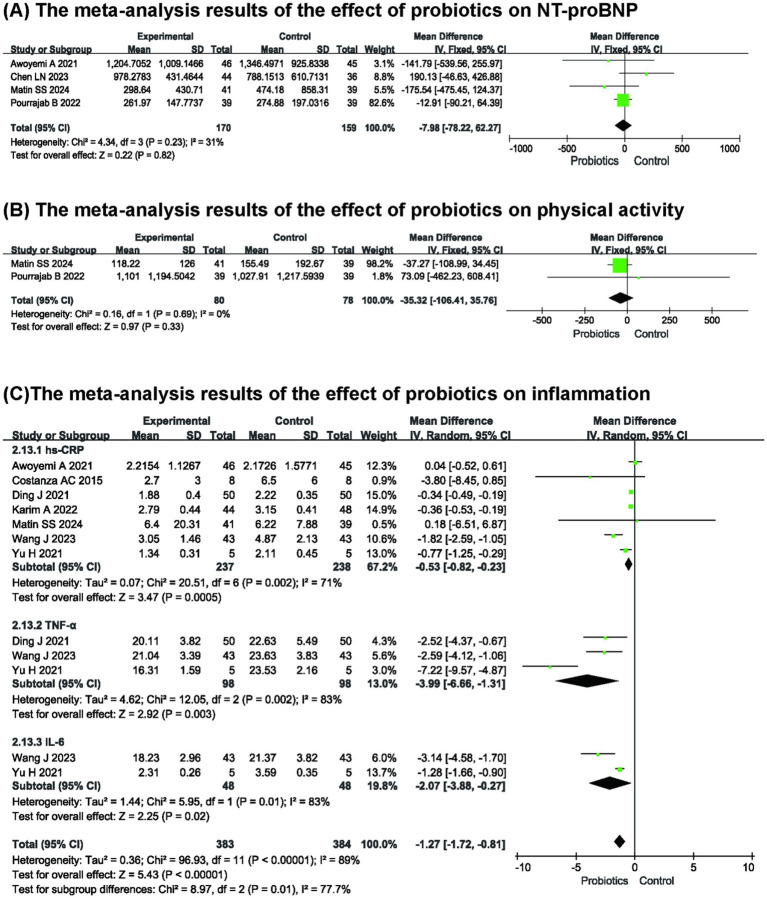 Figure 4
Figure 4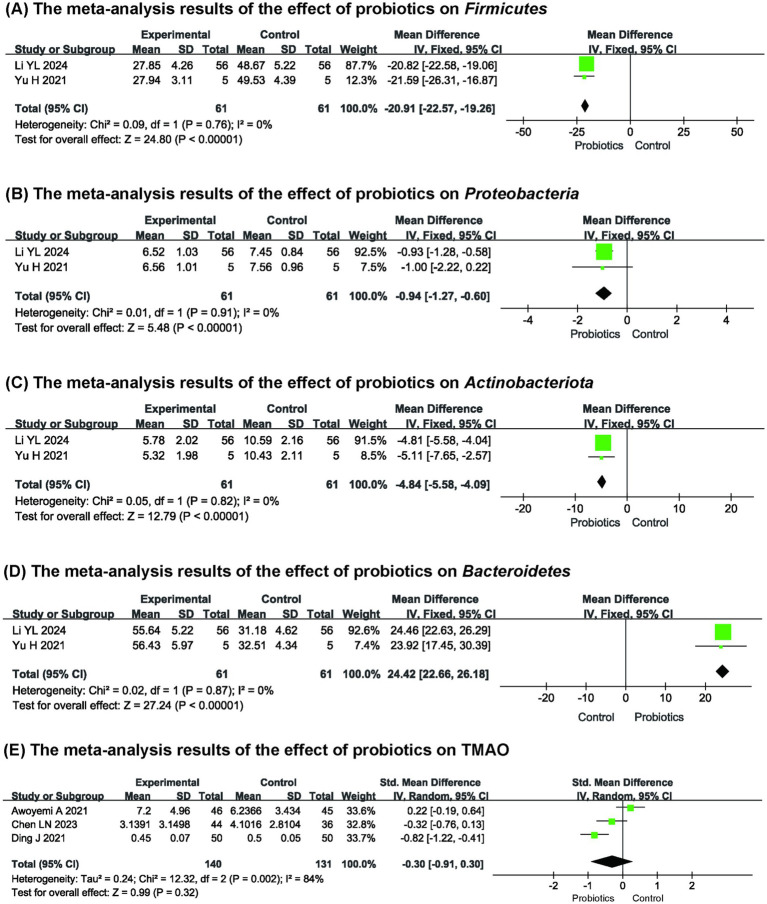 Figure 5
Figure 5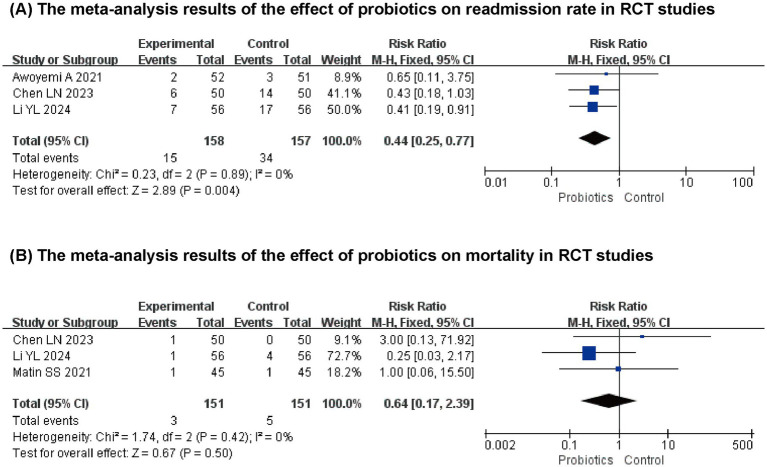 Figure 6
Figure 6| Study (year) | Country | Participants (Experimental/Control group) | Male/ | Age (mean±SD) | Types of heart failure | Experimental group | Control group | Time of treatment | Outcomes | Rehospitalization rate and mortality rate |
|---|---|---|---|---|---|---|---|---|---|---|
| Costanza AC (2015) ( | Brazil | 8/8 | NR | NR | NYHA II-III | Placebo | 12 weeks |
hsCRP LVEF | NR | |
| Yu H (2021) ( | China | 5/5 | C:3/2 | C:70.14 ± 4.71 | NR | Dietary management | 6 weeks |
hsCRP TNF-α IL-6 Abundance of intestinal flora | NR | |
| Matin SS | Iran | 41/39 | C:25/14 | C:50.1 ± 10.56 | NYHA I-III, HFrEF | Placebo | 10 weeks |
sCD163 sTWEAK physical activity NTpro-BNP hs-CRP | Experimental/Control group: | |
| Ding J (2021) ( | China | 50/50 | C:29/21 | C:65.86 ± 5.35 | NYHA II-III | Conventional treatment | 12 weeks |
LVEF TNF-α hsCRP TMAO | NR | |
| Li YL (2024) ( | China | 56/56 | C:29/27 | C:63.15 ± 4. 82 | NYHA II-III | ARB + ACEI | 16 weeks |
LVEF LVESV Abundance of intestinal flora TMAO TNF-α | Experimental/Control group: | |
| Wang J (2023) ( | China | 43/43 | C:26/17 | C:67.23 ± 7.36 | NYHA II-IV | Conventional treatment | 12 weeks |
LVEF LVESV hs-CRP TNF-α IL-6 | NR | |
| Ayodeji A (2021) ( | Norway | 52/51 | C:38/13 | C:60 ± 10 | NYHA II-III, HFrEF | Conventional treatment | 12 weeks |
LVEF NTpro-BNP CRP TMAO | Experimental/Control group: | |
| Pourrajab B (2020,2022) ( | Iran | 39/39 | C:26/13 | C:53.87 ± 7.25 | NYHA I-III,HFrEF | Ordinary yogurt | 10 weeks |
NTpro-BNP physical activity sCD163 sTWEAK | NR | |
| Karim A (2022) ( | United Arab Emirates | 44/48 | C:48/0 | C:65.2 ± 5.6 | HFrEF | Placebo | 12 weeks |
LVEF CRP | NR | |
| Chen LN (2023) ( | China | 50/50 | C:26/24 | C:70.60 ± 6.24 | NYHA II-III | Conventional treatment | 12 weeks |
LVEF NTpro-BNP TMAO | Experimental/Control group: | |
| Zhang Y (2017) ( | China | 25/25 | C:23/2 | C:86.2 ± 4.6 | NYHA II-III | Conventional treatment | 12 weeks |
LVEF | NR |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProbiotics and Fermented Foods · Gut microbiota and health · Cardiac Fibrosis and Remodeling
Introduction
1
Heart failure (HF) is a complex clinical syndrome that represents the advanced stage of various heart conditions. Statistics indicate that the prevalence and mortality of HF are rising annually, affecting more than 64 million individuals globally and causing approximately 1.73 million deaths each year (1). This makes HF a significant public health concern worldwide. The pathogenesis of HF is highly complex, involving disruptions in neuro-humoral regulation, myocardial remodeling, inflammation, and oxidative stress, among other contributing factors. While substantial advancements have been made in drug therapies and device therapies in recent years, the quality of life and long-term prognosis for patients remain inadequate. Consequently, investigating the pathophysiological mechanisms underlying HF and identifying new intervention targets have become prominent research areas.
In recent years, the rapid advancements of microbiome research have gradually illuminated the link between gut microbiota (GM) and various diseases, including HF. The GM is often referred to as the “second genome” of the human body, playing a crucial role in regulating metabolism, immunity, and intestinal barrier function (2). The “Heart Failure Gut Hypothesis” posits that during HF, reduced cardiac output and systemic congestion result in insufficient intestinal perfusion, leading to intestinal ischemia, compromised barrier function, microbiota imbalance, bacterial translocation, and endotoxemia. These changes activate systemic inflammation, creating a vicious cycle that exacerbates myocardial damage and worsens cardiac function (3). This hypothesis not only offers a novel perspective on the pathogenesis of HF but also suggests that regulating the GM could emerge as a potential target for HF treatment.
Probiotics have been shown to be an effective strategy for regulating intestinal flora and enhancing the functionality of the intestinal barrier. Previous studies have demonstrated that probiotics can reduce risk factors associated with cardiovascular disease, such as blood lipid levels (4). Subsequent research further revealed the anti-inflammatory, antioxidant, and intestinal microbiota-regulating effects of probiotics under conditions of cardiac remodeling after myocardial infarction (5). This underscores the significant potential of probiotics in improving cardiac health. Numerous animal and clinical studies have investigated the effects of probiotics on HF and their underlying mechanisms, including the regulation of intestinal flora composition, reduction of harmful metabolites (such as trimethylamine-N-oxide, TMAO), promotion of beneficial metabolites (like short-chain fatty acids, SCFAs), inhibition of inflammatory signaling pathways, and alleviation of myocardial fibrosis (6–8).
While previous studies have investigated the benefits of probiotics for HF from various perspectives, the inconsistency in certain outcome measures complicates the clear definition of the role and position of probiotics in HF treatment. Therefore, we conducted a systematic review and meta-analysis of a randomized controlled trial (RCT) on the effects of probiotic supplements on patients with HF to comprehensively evaluate the role of probiotics in the management of HF.
Methods
2
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines and the recommendations of the Cochrane Collaboration. Details of the protocol for this systematic review were registered on PROSPERO (CRD420251083960).
Search strategy
2.1
Computerized searches were conducted across eight major databases: PubMed, Embase, Cochrane, Web of Science, CNKI, Wanfang Database, the United States Clinical Trial Registry, and the Chinese Clinical Trial Registry. Search the published literature from the establishment of the database until September 9, 2025. The search did not limit the publication language of the literature. The search strategy incorporated subject terms and free-text keywords, developed through iterative pre-searches. Additionally, manual searching was employed as a supplementary method. Detailed information regarding the search strategy can be found in the Supplementary File 1.
Eligibility criteria
2.2
Inclusion criteria: (1) Participants: Patients diagnosed with HF. (2) Intervention: Trials where the treatment group received probiotic intervention (including single-strain or multi-strain preparations), with probiotics administered as monotherapy or adjuvant therapy, and the control group received a placebo. (3) Outcome Indicators: Studies must include at least one primary or secondary outcome indicator. Primary outcome indicators include cardiac function and N-terminal pro-B-type natriuretic peptide (NT-proBNP). Secondary indicators encompass factors related to inflammation, intestinal flora abundance, activity endurance, readmission rate, and mortality. (4) Study Design: RCT.
Exclusion criteria: (1) Not an RCT; (2) The intervention measure is not probiotics; (3) Duplicated literature; (4) Reviews, comments, conference papers, dissertations; (5) Full text not available; (6) No available outcome indicators.
Study screening and data extraction
2.3
Two researchers independently screened the literature using NoteExpress (version 4.2.0.10156) software based on the inclusion and exclusion criteria. Translation tools were used to assist in determining eligibility for inclusion and reducing single-language comprehension biases. In instances of disagreement between the two researchers, they consulted a third researcher to reach a consensus. The extracted data included authors’ names, publication year, country or region, the sample sizes of the experimental and control groups, age, sex ratio, specific intervention measures, intervention duration, and outcome indicators. When results were only available in graphical format, the GetData2.26 software extracted numerical values from the graphs. This software has been effectively utilized in other meta-analyses and is recognized as a reliable method for extracting data from studies (9).
Risk of bias
2.4
The Cochrane Collaboration risk of bias tool was used to evaluate the quality of the literature in seven aspects: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Each aspect was categorized as “low risk” “unclear risk” or “high risk.” Two researchers conducted independent evaluations, and in instances of disagreement, they consulted with a third researcher to achieve consensus.
Statistical analyses
2.5
Meta-analysis was conducted utilizing Review Manager 5.4 and Stata 18. The results for binary variables were expressed as relative risk (RR) along with a 95% confidence interval (95% CI), while continuous variables were presented as either mean difference (MD) or standardized mean difference (SMD). The heterogeneity among the studies was assessed using I^2^ statistics and p-values from the chi-square test. When I^2^ < 50% and p > 0.1, it indicated no heterogeneity among the studies, and a fixed-effect model was used; otherwise, a random-effect model was adopted. Sensitivity analysis or subgroup analysis was performed on outcomes with high heterogeneity to identify the sources of heterogeneity, and the stability and reliability of the overall results were evaluated simultaneously. Funnel plots were generated using Stata 18 to test and assess publication bias. Additionally, the Kappa value was calculated using SPSS 25.0 software to assess the degree of consistency between the two researchers’ literature screening and quality evaluation results. The results are presented in Supplementary File 1.
Result
3
Results of study search and selection
3.1
The preliminary search yielded 4,972 articles that met the established criteria. After eliminating 747 duplicate articles using NoteExpress and screening for relevant research content by reviewing titles and abstracts, 74 articles were obtained. After excluding articles where the RCTs were not related to HF, those with intervention measures other than probiotics, those without full-text access, and those without available outcome indicators, 13 articles were selected for further review. After merging the literature with the same clinical trial registration number, a total of 11 studies were ultimately included in meta-analysis. The detailed literature screening process is shown in Figure 1.
Flow chart of the process of study selection.
Characteristics of included studies
3.2
Table 1 shows the main characteristics of the included clinical studies. A total of 11 RCTs were included (8, 10–21), involving 827 participants. Six of the studies were conducted in China (8, 11, 13, 14, 19, 21), two in Iran (12, 16, 17, 20), and one each in Brazil (10), Norway (15), and the United Arab Emirates (18). Among the included studies, 10 studies (8, 10, 12–16, 19, 21) specified the New York Heart Association’s cardiac function classification for the participants, and four studies included patients with heart failure with reduced ejection fraction (HFrEF) (12, 15, 16, 18). The average treatment duration was 11.5 weeks. The most commonly used probiotic genera were Lactobacillus and Bifidobacterium.
Study quality
3.3
Figure 2 shows the assessment of study quality and risk of bias, using the Cochrane Collaboration risk of bias tool. The studies by Awoyemi A (15), Costanza AC (10), Matin SS (12), and Pourrajab B (16) indicated a lower risk of bias. The studies by Ding J (8), Li YL (13), and Wang J (14) indicated a higher risk of bias. In general, the blinding of participants, researchers, and outcome assessors, the generation of random sequences, and the allocation concealment process are aspects with a higher risk of bias.
Quality assessment of RCTs. (A) Risk of bias summary of RCTs. (B) Risk of bias graph of RCTs.
Meta-analysis results
3.4
Effects of probiotics on cardiac function
3.4.1
Eight studies (8, 10, 13–15, 18, 19, 21) reported left ventricular ejection fraction (LVEF). Figure 3A shows the meta-analysis results: compared with the control group, probiotics increased LVEF (n = 627, MD: 2.69, 95% CI (0.39, 4.99), p = 0.02, I^2^ = 82%). Due to the significant heterogeneity observed among the included studies, a sensitivity analysis was performed. Although we sequentially excluded each study, the source of the heterogeneity remained unclear. Nevertheless, the sensitivity analysis indicated that the results were stable.
(A) The meta-analysis results of the effect of probiotics on LVEF (B) The dose subgroup analysis of probiotics on LVEF (C) The meta-analysis results of the effect of probiotics on LVESV.
We further explored the source of heterogeneity by dividing the subjects into two subgroups based on probiotic dose (> 1 g and ≤ 1 g) for subgroup analysis. The results are shown in Figure 3B. When the probiotic dose was ≤ 1 g, probiotics had no significant effect on LVEF compared to the control group (MD: 0.79, 95% CI (−1.05, 2.64), p = 0.40), and the heterogeneity was low (p = 0.30, I^2^ = 18%). When the probiotic dose was > 1 g, a significant improvement in LVEF was noted (MD: 3.75, 95% CI (0.53, 6.97), p = 0.02), although this subgroup exhibited high heterogeneity (p < 0.00001, I^2^ = 86%). This indicates that the difference in probiotic dose may be the source of heterogeneity, and it is a relevant factor affecting the improvement effect of LVEF.
Furthermore, two studies (13, 14) reported on left ventricular end systolic volume (LVESV) (Figure 3C), revealing that probiotics significantly decreased LVESV compared to the control group (n = 198, MD: −6.13, 95% CI: (−7.33, −4.93), p < 0.00001, I^2^ = 0%).
Effect of probiotics on NT-proBNP
3.4.2
Four studies (15–17, 19) reported the effect of probiotics on serum NT-proBNP. The results indicated that probiotics did not reduce NT-proBNP compared with the control group (n = 329, MD: −7.98, 95% CI (−78.22, 62.27), p = 0.82, I^2^ = 31%) (Figure 4A).
The meta-analysis results of the effect of probiotics on (A) NT-proBNP (B) physical activity (C) inflammation.
Effect of probiotics on physical activity
3.4.3
Two studies (17, 20) reported the effects of probiotics on physical activity. The meta-analysis results indicated that probiotics did not improve the activity endurance of patients with HF (n = 158, MD: −35.32, 95% CI (−106.41, 35.76), p = 0.33, I^2^ = 0%) (Figure 4B).
Effect of probiotics on inflammation
3.4.4
A total of seven studies (8, 10, 11, 14, 15, 17, 18) examined the effects of probiotics on inflammation. The meta-analysis of hypersensitive C-reactive protein (hs-CRP), interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) indicated a significant overall effect, indicating that probiotics can inhibit the systemic inflammation in patients with HF (n = 475, MD: −1.27, 95% CI (−1.72, −0.81), p < 0.00001, I^2^ = 89%) (Figure 4C). Regarding sensitivity analysis, the results showed no significant change in the overall effect compared with that of the subgroups.
Effect of probiotics on the intestinal flora and its products
3.4.5
Two studies (n = 122) (11, 13) reported the effects of probiotics on the GM abundance. Among them, the Firmicutes and the Bacteroidetes were the dominant bacterial groups in the intestines of patients with HF. The results revealed that compared with the control group, probiotics could reduce the proportions of Firmicutes (MD: −20.91, 95% CI (−22.57, −19.26), p < 0.00001, I^2^ = 0%), Proteobacteria (MD: −0.94, 95% CI (−1.27, −0.60), p < 0.00001, I^2^ = 0%), and Actinobacteriota (MD: −4.84, 95% CI (−5.58, −4.09), p < 0.00001, I^2^ = 0%) in the intestines, and increase the proportion of Bacteroidetes (MD: 24.42, 95% CI (22.66, 26.18), p < 0.00001, I^2^ = 0%) (Figures 5A–D), thereby contributing to the regulation of GM.
The meta-analysis results of the effect of probiotics on (A) Firmicutes (B) Proteobacteria (C) Actinobacteriota (D) Bacteroidetes (E) TMAO.
Three studies (8, 15, 19) indicated that TMAO was not significantly influenced by probiotics when compared to the control group (MD: −0.30, 95% CI (−0.91, 0.30), p = 0.32, I^2^ = 84%) (Figure 5E). This finding also suggested considerable heterogeneity among the studies. In an effort to identify the source of this heterogeneity, we systematically removed each study one by one; however, the underlying cause remained elusive. Nevertheless, the sensitivity analysis demonstrated that the results were stable.
Effect of probiotics on the readmission rate and mortality
3.4.6
Three studies (13, 15, 19) reported the impact of probiotics on readmission rates. The results from the meta-analysis indicated that probiotics significantly reduced the readmission rates of patients with HF compared to the control group (n = 315, RR: 0.44, 95% CI (0.25,0.77), p = 0.004, I^2^ = 0%). However, a meta-analysis of the three clinical studies that evaluated mortality (13, 17, 19) revealed no significant effect of probiotics on mortality (n = 302, RR: 0.64, 95% CI (0.17, 2.39), p = 0.50, I^2^ = 0%) (Figure 6).
The meta-analysis results of the effect of probiotics on (A) readmission rate (B) mortality.
Publication bias
3.5
We used funnel plots to assess publication bias in the meta-analysis results with a total of ≥ 5 included studies. The funnel plots were all approximately symmetrical (Supplementary Figure S1).
Discussion
4
Our study included 11 RCTs involving 827 participants, aiming to review and analyse the effects of probiotic supplements on the cardiac function, overall condition, and prognosis of patients with HF, to reveal their potential benefits as supplementary treatments for HF. Previous similar studies showed that probiotics had no improvement effect on the LVEF of patients with HF (22). After including new studies, we found that probiotics could increase LVEF by 2.69%, and this improvement was manifested when the daily dose was > 1 g. However, from a clinical perspective, a 2.69% increase was within the range of routine measurement errors for LVEF. Additionally, the results indicated that probiotics had no beneficial effects on NT-proBNP or activity endurance. Nevertheless, probiotics significantly reduced the LVESV in HF patients. This suggests that probiotics have a slight improvement effect on cardiac remodeling at the microscopic level, but the efficacy is negligible for the overall complex physiological and pathological state of patients with HF.
The excessive proliferation of cardiac fibroblasts and the accumulation of extracellular matrix lead to cardiac remodeling, an important pathological precursor of HF. The cross-linked carboxyl terminal telopeptide (ICTP) is a crucial biomarker for monitoring extracellular matrix metabolism in the myocardium (23). Elevated levels of ICTP are strongly correlated with the development of HF (24). The research by Li et al. demonstrated that probiotics enhanced the inhibitory effect of the angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on the renin-angiotensin system, reduced ICTP in patients with HF, alleviated myocardial fibrosis, and thereby reversed ventricular remodeling (13). The mechanism by which probiotics inhibit myocardial fibrosis and alleviate ventricular remodeling may be related to the inhibition of inflammation, regulation of the intestinal flora, and improvement of cardiac energy metabolism.
Activation of the transforming growth factor-β (TGF-β) pathway is crucial for myofibroblast formation and induction, and TGF-β antibodies alleviate cardiac fibrosis and diastolic dysfunction (25). SCFAs like acetate and butyrate are metabolic products of the GM that help prevent systemic inflammation and maintain intestinal barrier integrity. An imbalance in GM can disrupt SCFA production and weaken the gastrointestinal epithelium, allowing luminal toxins to enter, triggering inflammation in the cardiovascular system and contributing to cardiac fibrosis (26). Studies indicate that HF is associated with decreased bacterial richness and a loss of butyric acid-producing bacteria (27). Wang et al. induced myocardial fibrosis in mice and found that butyric acid supplementation reduced Collagen I and TGF-β expression, preventing fibrosis progression. Additionally, Bifidobacterium pseudolongum enhanced butyric acid production by Lactobacillus butyricum, and their combined use showed a stronger anti-myocardial fibrosis effect (6). In HF, increased fatty acid oxidation inhibits glucose utilization, disrupts the glucose-fatty acid cycle in the heart, creates energy imbalance, and promotes cell damage and fibrosis activation (28). Tuerhongjiang G et al. discovered a negative correlation between intestinal Clostridium and circulating saturated fatty acids (SFA) in both HF patients and animal models. Administration of Clostridium sporogenes reduced SFA, regulated cardiac energy metabolism, and inhibited myocardial fibrosis, thereby improving cardiac function in HF mice (29).
Growing evidence shows that inflammation-related GM imbalance is linked to HF. The “intestinal leak” hypothesis suggests that GM imbalance disrupts tight junctions in intestinal cells, allowing toxins to enter the bloodstream and leading to systemic inflammation that impacts the cardiovascular system (30). Common mechanisms of intestinal damage in HF patients include reduced cardiac output, excessive activation of the sympathetic system, ischemic swelling of the intestinal mucosa, and deterioration of intestinal wall barrier function (31). Under such pathological conditions, inflammatory factors such as hs-CRP, IL-6, and TNF-α are produced.
Hs-CRP is a classic inflammatory marker for HF assessment and can exacerbate the disease by increasing oxidative stress and disrupting energy metabolism (32). IL-6 plays a crucial regulatory role in the inflammation associated with HF. In this context, cardiomyocytes and macrophages increase IL-6 secretion, activating NF-κB and other pathways, which recruit more inflammatory factors and amplify systemic inflammation (33, 34). Furthermore, IL-6 can promote myocardial fibrosis by activating the TGF-β1 pathway or interfering with myocardial metabolism, worsening the overall condition of HF patients through multiple mechanisms (35, 36). TNF-α is an important pro-inflammatory factor in the development of HF. Besides amplifying the inflammation and stimulating myocardial fibrosis, TNF-α can directly inhibit myocardial contraction by reducing sarcoplasmic reticulum proteins and impairing the efficiency of calcium uptake and release in cardiomyocytes (37). Studies have indicated that alterations in the dominant microbial population and intestinal epithelial damage in HF patients may induce the secretion of inflammatory mediators, including hs-CRP, IL-6, and TNF-α (32, 38). Our findings demonstrate that probiotic administration reduced levels of hs-CRP (8, 10, 11, 14, 15, 17, 18), IL-6 (11, 14), and TNF-α (8, 11, 14) in HF patients, with a significant overall effect. Additionally, Wang et al. conducted animal experiments that demonstrated probiotics inhibit the maturation and secretion of TNF-α and IL-6, mediated by the NOD-like receptor thermal protein domain-associated protein 3, thus regulating inflammation in HF (39).
The predominant bacterial species in the human intestinal microbiota mainly include Firmicutes, Bacteroidetes, Proteobacteria, and Actinobacteria (40). Recent studies show decreased diversity or imbalanced composition of GM in HF patients (41). Many bacterial species in the Firmicutes ferment dietary fibers to produce SCFAs, which can inhibit inflammation by activating G protein-coupled receptors and reducing pro-inflammatory factors (42). Studies have shown a significant increase in Firmicutes levels in the intestines of HF animals (43, 44). Our results show that the intervention of probiotics can reduce the proportion of the Firmicutes in HF patients (11, 13). This phenomenon may be caused by intestinal microcirculation disorders and abnormal permeability during HF, which trigger cytokine production and create a favorable environment for Firmicutes proliferation, leading to increased abundance of this phylum. Probiotics use inhibits inflammation and promotes intestinal mucosal repair, thereby alleviating the stimuli that drive Firmicutes proliferation. Bacteroidetes also contribute to SCFA production, helping maintain intestinal integrity, regulate immune function, and alleviate cardiac hypertrophy and myocardial fibrosis (45). Proteobacteria are a marker of GM imbalance. All members of this phylum are Gram-negative bacteria, with their outer membrane primarily composed of lipopolysaccharides (LPS). When LPS enters the bloodstream, it activates the NF-κB pathway, increasing TNF-α, IL-6, and IL-1β levels, which worsen systemic inflammation and HF progression (46). A meta-analysis found that in HF patients, Bacteroidetes decreased and Proteobacteria increased compared to non-HF patients (47). In light of this shift in bacterial community proportions, our findings indicated that administering probiotics increased Bacteroidetes and decreased Proteobacteria (11, 13). Bifidobacteria are essential members of the Actinobacteria, helping to reduce ammonia in feces and lower intestinal pH, creating an optimal gut environment. They also inhibit harmful bacteria and inflammatory factors (48–50). Studies indicate that Actinobacteria, particularly Bifidobacteria, increase in the intestines of HF patients, potentially due to compensatory adaptations to the intestinal environment (47, 51). The studies by Yu (11) and Li (13) demonstrated that probiotics can reduce the level of the Actinobacteria in the intestines of patients with HF, but the mechanisms need further investigation.
TMAO is a harmful metabolite created by gut bacteria from choline and carnitine, leading to oxidative stress and inflammation. This can result in endothelial and mitochondrial dysfunction, contributing to myocardial hypertrophy, fibrosis, and impaired cardiac function. Elevated TMAO levels are closely associated with late diastolic dysfunction of the left ventricle and affect the prognosis of patients with HF (52). Nevertheless, our meta-analysis did not find any evidence that probiotics reduce TMAO levels in patients with HF (8, 15, 19). This is related to the specificity of TMAO metabolism by the microbiota, and the probiotics we included in the study were not effective strains for reducing TMAO levels (53).
Regarding safety and prognosis, previous studies evaluated the effect of probiotics on renal function in patients with HF, and the results showed no difference compared to the control group. Our study focused on mortality and readmission rates, and the results revealed that probiotics could not reduce the mortality rate of patients with HF, but could lower the readmission rate of HF patients. This result provides a new option for improving patient prognosis and reducing medical costs while supporting the clinical application of the “gut-heart axis” theory.
Overall, probiotics act as an auxiliary regulator rather than a core treatment in HF management. They have a certain delaying effect on the structural progression of HF and have potential value in maintaining long-term cardiac function. Moreover, the anti-inflammatory and GM-regulating effects of probiotics are more targeted for patients with infections, diarrhea, and constipation, and can serve as an auxiliary measure to reduce medical expenses and improve quality of life. This conclusion encourages clinicians to apply probiotics more rationally, integrating them into the “multi-target comprehensive management strategy” for HF rather than as an independent treatment option.
Limitations
5
Our research has certain limitations. Firstly, the quality of the included studies was relatively low, some studies neglected the importance of randomization, blinding, and allocation concealment.
The limited number of included studies and small sample size led to three main issues. Firstly, this resulted in an overestimation of the effect size; while probiotics showed a cardioprotective effect on HF, the actual therapeutic effect was small. Combined with the insufficient sample size, this further reduced the statistical persuasiveness of the results. Secondly, the limited sample restricted deeper analysis of heterogeneity; despite conducting subgroup and sensitivity analyses, it remained challenging to clarify the real impact of potential moderating factors on the intervention effect. Lastly, Egger’s test for publication bias could not be used, making the assessment of bias rely on subjective judgment from the funnel plot, which further increased the uncertainty in assessing publication bias. Therefore, future high-quality, multicenter, and large-sample studies are needed.
Current evidence on probiotics for HF has two main shortcomings: First, there is limited exploration of underlying mechanisms; most studies focus on therapeutic indicators without identifying specific cardioprotective targets. Second, the specificity of strains is often unclear, as many studies use multi-strain combinations rather than single strains, making it difficult to assess their independent effects. Future research should examine the efficacy and dose-effect relationships of individual strains to provide clearer evidence for clinical applications.
Conclusion
6
In conclusion, the systematic review and meta-analysis indicate that probiotics have a protective effect on the heart and can reduce readmission rates. A daily dose of > 1 g is recommended. However, probiotics have no benefits for NT-proBNP, exercise endurance, or mortality. They can be used as an adjunctive treatment in the management of HF. Based on the evidence from RCTs, the most commonly used probiotic species are Lactobacillus and Bifidobacterium. The mechanism by which probiotics exert their effects may be related to anti-myocardial fibrosis, anti-inflammation, regulation of the GM, and improvement of myocardial energy metabolism. However, the heterogeneity of the meta-analysis results and the varying quality of some studies have diminished the credibility of the findings. Therefore, further high-quality research is needed to validate these results in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Savarese G Becher PM Lund LH Seferovic P Rosano GMC Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. (2023) 118:3272–87. doi: 10.1093/cvr/cvac 013, 35150240 · doi ↗ · pubmed ↗
- 2Zhao L. Genomics: the tale of our other genome. Nature. (2010) 465:879–80. doi: 10.1038/465879 a, 20559375 · doi ↗ · pubmed ↗
- 3Matacchione G Piacenza F Pimpini L Rosati Y Marcozzi S. The role of the gut microbiota in the onset and progression of heart failure: insights into epigenetic mechanisms and aging. Clin Epigenetics. (2024) 16:175. doi: 10.1186/s 13148-024-01786-9, 39614396 PMC 11607950 · doi ↗ · pubmed ↗
- 4Sun J Buys N. Effects of probiotics consumption on lowering lipids and CVD risk factors: a systematic review and meta-analysis of randomized controlled trials. Ann Med. (2015) 47:430–40. doi: 10.3109/07853890.2015.1071872, 26340330 · doi ↗ · pubmed ↗
- 5Taslim NA Yusuf M Ambari AM del Rosario Puling IM Ibrahim FZ Hardinsyah H . Anti-inflammatory, antioxidant, metabolic and gut microbiota modulation activities of probiotic in cardiac remodeling condition: evidence from systematic study and Meta-analysis of randomized controlled trials. Probiotics Antimicrob Proteins. (2023) 15:1049–61. doi: 10.1007/s 12602-023-10105-2, 37349622 PMC 10393865 · doi ↗ · pubmed ↗
- 6Wang J Chen J Li L Zhang H Pang D Ouyang H . Clostridium butyricum and Bifidobacterium pseudolongum attenuate the development of cardiac fibrosis in mice. Microbiol Spectr. (2022) 10:e 0252422. doi: 10.1128/spectrum.02524-22, 36318049 PMC 9769846 · doi ↗ · pubmed ↗
- 7Hesari Z Kafshdoozan K Barati M Kokhaei P Andalib S Talebi Kiassari F . Lactobacillus paracasei impact on myocardial hypertrophy in rats with heart failure. J Chem Health Risks. (2020) 10:67–74. doi: 10.22034/jchr.2020.1888659.1080 · doi ↗
- 8Ding J Jing HZ Wang ZL Yang Q. A study on the impact of probiotics on patients with chronic heart failure based on the analysis of the intestinal flora. J Hainan Med Univ. (2021) 27:260–4. doi: 10.13210/j.cnki.jhmu.20200902.003 · doi ↗