A Placebo-Controlled Exploratory Trial of Sirolimus for Tocilizumab-Resistant Idiopathic Multicentric Castleman Disease: Early Termination and Long-Term Extension Results Based on Descriptive Results From Two Patients
Tomohiro Koga, Remi Sumiyoshi, Toshimasa Shimizu, Naoki Hosogaya, Chizu Fukushima, Hiroshi Yamamoto, Hajime Yoshifuji, Shinji Higa, Atsushi Kawakami

TL;DR
A small study on sirolimus for a rare disease showed promising results when patients switched from placebo, despite early termination.
Contribution
The study provides early evidence suggesting sirolimus may benefit patients with tocilizumab-resistant iMCD.
Findings
The sirolimus-treated patient maintained disease stability while the placebo patient worsened.
Switching the placebo patient to sirolimus led to significant improvement in disease scores.
Sirolimus showed a favorable safety profile over 40 weeks.
Abstract
Background Idiopathic multicentric Castleman disease (iMCD) remains challenging to treat, with a considerable number of patients showing insufficient response to tocilizumab, the current standard therapy for iMCD. Sirolimus, an mTOR inhibitor, is a potential therapeutic option for tocilizumab-resistant cases based on its mechanism of action and preliminary case reports. Methods This investigator-initiated, multicenter, exploratory, placebo-controlled study was designed to evaluate sirolimus (2 mg daily) versus placebo in patients with tocilizumab-resistant iMCD. The primary endpoint was the change in the CHAP (CRP, Hemoglobin, Albumin, Performance Status) score from baseline at week 16. The study was prematurely terminated due to recruitment challenges and the impact of the COVID-19 pandemic, enrolling only two of the planned 20 participants. Both patients completed a 40-week…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
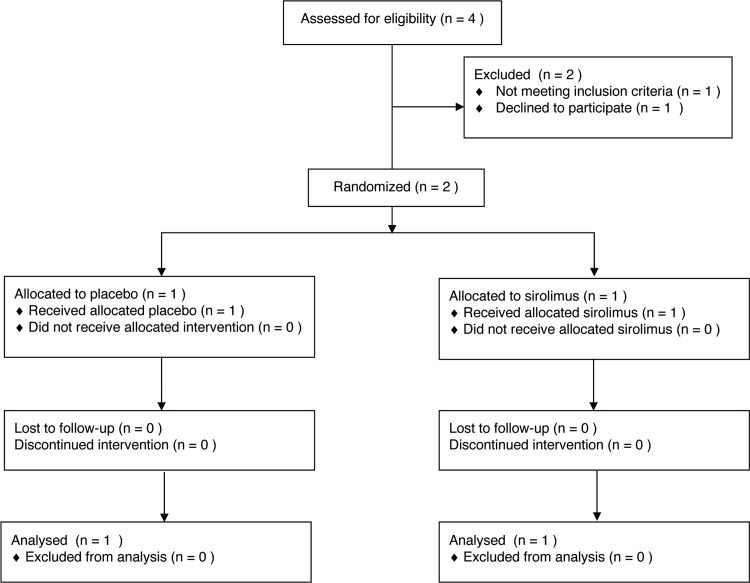 Figure 1
Figure 1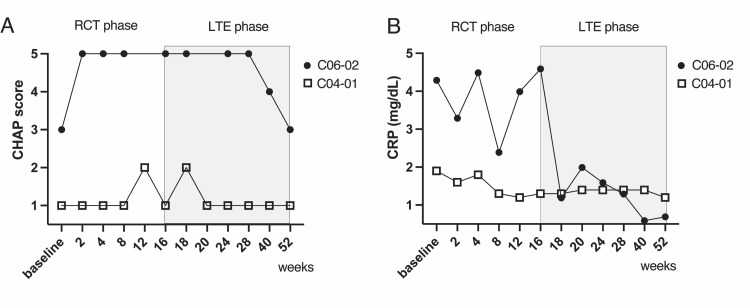 Figure 2
Figure 2| C04-01 | C06-02 | |
| Gender | female | male |
| Age | 47 | 61 |
| Race | Asian | Asian |
| Pathological findings of lymph nodes | Plasma cell type | Hyaline vascular type |
| BMI (kg/m2) | 19.6 | 32.3 |
| CRP (mg/L) | 19 | 43 |
| White blood cells (/μL) | 7900 | 9400 |
| Hemoglobin (g/dL) | 13.1 | 10.4 |
| Platelet count (×103/μL) | 312 | 200 |
| Albumin (g/dL) | 4.3 | 3.2 |
| Creatinine (mg/dL) | 0.5 | 1.5 |
| IgG (mg/dL) | 1030 | 2210 |
| ECOG PS | 0 | 1 |
| CHAP Score | 1 |
| Group | Subject Number | Visit | Sirolimus Blood Concentration (ng/mL) |
| Sirolimus | C04-01 | 1 Week | 9.2 |
| 2 Weeks | 13.5 | ||
| 4 Weeks | 12.5 | ||
| 8 Weeks | 11.6 | ||
| 12 Weeks | 23.2 | ||
| 16 Weeks | 27.8 | ||
| Placebo | C06-02 | 1 Week | 1.0 (Not detected) |
| 2 Weeks | 1.0 (Not detected) | ||
| 4 Weeks | 1.0 (Not detected) | ||
| 8 Weeks | 1.0 (Not detected) | ||
| 12 Weeks | 1.0 (Not detected) | ||
| 16 Weeks | 1.0 (Not detected) |
| CHAP Score | CRP | Hemoglobin | Albumin | ECOG PS | ||||
| Group | Subject | Visit | CHAP Score | CRP Subscore* | (mg/dL) | (g/dL) | (g/dL) | PS |
| Number | ||||||||
| Sirolimus | C04-01 | Baseline | 1 | 0 | 1.9 | 13.1 | 4.3 | 0 |
| 2 Weeks | 1 | 0 | 1.6 | 13.2 | 4.1 | 0 | ||
| 4 Weeks | 1 | 0 | 1.8 | 13.6 | 4.2 | 0 | ||
| 8 Weeks | 1 | 0 | 1.3 | 12.6 | 4.2 | 0 | ||
| 12 Weeks | 2 | 1 | 1.2 | 11.6 | 4.2 | 0 | ||
| 16 Weeks | 1 | 0 | 1.3 | 12.4 | 4.3 | 0 | ||
| Placebo | C06-02 | Baseline | 3 | 2 | 4.3 | 10.4 | 3.2 | 1 |
| 2 Weeks | 5 | 4 | 3.3 | 8.7 | 2.9 | 1 | ||
| 4 Weeks | 5 | 4 | 4.5 | 8.6 | 2.9 | 1 | ||
| 8 Weeks | 5 | 4 | 2.4 | 8.5 | 2.7 | 1 | ||
| 12 Weeks | 6 | 5 | 4 | 7.9 | 2.6 | 1 | ||
| 16 Weeks | 5 | 4 | 4.6 | 8.5 | 2.8 | 1 | ||
| Subject | Physician | Patient | ||
| Group | Number | Visit | VAS | VAS |
| Sirolimus | C04-01 | Baseline | 16 | 0 |
| 2 Weeks | 10 | 47 | ||
| 4 Weeks | 27 | 52 | ||
| 8 Weeks | 28 | 49 | ||
| 12 Weeks | 27 | 49 | ||
| 16 Weeks | 11 | 50 | ||
| Placebo | C06-02 | Baseline | 22 | 22 |
| 2 Weeks | 41 | 36 | ||
| 4 Weeks | 38 | 26 | ||
| 8 Weeks | 26 | 27 | ||
| 12 Weeks | 40 | 43 | ||
| 16Weeks | 40 | 38 |
| Subject | 1-100 Score | NB Score | ||||||||||||||||||
| Group | Number | Visit | PF | RP | BP | GH | VT | SF | RE | MH | PF | RP | BP | GH | VT | SF | RE | MH | ||
| Sirolimus | C04-01 | Baseline | 85 | 100 | 62 | 37 | 43.8 | 100 | 91.7 | 55 | 47 | 55.7 | 44.7 | 36.2 | 40.2 | 57 | 51.9 | 41.1 | ||
| 4 Weeks | 85 | 93.8 | 62 | 42 | 50 | 100 | 100 | 65 | 47 | 52.4 | 44.7 | 38.9 | 43.4 | 57 | 56.1 | 46.5 | ||||
| 8 Weeks | 85 | 93.8 | 100 | 42 | 43.8 | 100 | 100 | 75 | 47 | 52.4 | 61.7 | 38.9 | 40.2 | 57 | 56.1 | 51.8 | ||||
| 12 Weeks | 80 | 62.5 | 72 | 42 | 37.5 | 100 | 100 | 65 | 43.4 | 35.8 | 49.2 | 38.9 | 37 | 57 | 56.1 | 46.5 | ||||
| 16 Weeks | 85 | 75 | 100 | 42 | 37.5 | 100 | 100 | 75 | 47 | 42.4 | 61.7 | 38.9 | 37 | 57 | 56.1 | 51.8 | ||||
| Placebo | C06-02 | Baseline | 80 | 93.8 | 72 | 52 | 50 | 100 | 100 | 70 | 43.4 | 52.4 | 49.2 | 44.2 | 43.4 | 57 | 56.1 | 49.1 | ||
| 4 Weeks | 65 | 68.8 | 74 | 35 | 56.3 | 87.5 | 75 | 65 | 32.6 | 39.1 | 50.1 | 35.1 | 46.6 | 50.6 | 43.6 | 46.5 | ||||
| 8 Weeks | 70 | 81.3 | 62 | 35 | 50 | 75 | 75 | 65 | 36.2 | 45.8 | 44.7 | 35.1 | 43.4 | 44.1 | 43.6 | 46.5 | ||||
| 12 Weeks | 55 | 62.5 | 52 | 40 | 56.3 | 87.5 | 83.3 | 65 | 25.4 | 35.8 | 40.3 | 37.8 | 46.6 | 50.6 | 47.7 | 46.5 | ||||
| 16 Weeks | 55 | 68.8 | 52 | 40 | 43.8 | 75 | 66.7 | 60 | 25.4 | 39.1 | 40.3 | 37.8 | 40.2 | 44.1 | 39.4 | 43.8 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · PI3K/AKT/mTOR signaling in cancer · Multiple Myeloma Research and Treatments
Introduction
Idiopathic multicentric Castleman disease (iMCD) is a rare, life-threatening lymphoproliferative disorder characterized by systemic inflammation, constitutional symptoms, and dysregulated cytokine production, particularly interleukin-6 (IL-6) [1-4]. The estimated incidence ranges from 1,000 to 5,000 new cases annually in the United States, making it an orphan disease with limited treatment options [4]. The humanized anti-IL-6 receptor monoclonal antibody tocilizumab has emerged as a cornerstone therapy for iMCD, demonstrating efficacy in multiple studies and receiving regulatory approval [5]. However, clinical experience has revealed that approximately 40% of patients exhibit insufficient response to tocilizumab, creating a significant unmet medical need for alternative therapeutic approaches [5].
Recent research has identified dysregulation of the PI3K/AKT/mTOR signaling pathway in iMCD pathogenesis, particularly in IL-6 blockade-refractory cases [6]. The mammalian target of rapamycin (mTOR) is a central regulator of cell growth, metabolism, and immune function, making it an attractive therapeutic target [7]. Sirolimus (rapamycin), an FDA-approved mTOR inhibitor with an established safety profile in transplant medicine [8] and other autoimmune conditions, has shown promising results in case reports of tocilizumab-resistant iMCD [9-11].
This exploratory, placebo-controlled study was designed to provide the first randomized evidence regarding the efficacy and safety of sirolimus in patients with tocilizumab-resistant iMCD. While recruitment challenges led to early termination with a sample size smaller than planned, the study offers valuable insights into the potential role of mTOR inhibition in this difficult-to-treat population and provides important safety data for extended sirolimus use in patients with iMCD.
Materials and methods
Study design and setting
This investigator-initiated, multicenter, exploratory, placebo-controlled study with an open-label long-term extension (LTE) was conducted at eight medical centers across Japan. This study was registered in the Japan Registry of Clinical Trials (jRCT2071190029 and jRCT2051200050). The original protocol and amendments were approved by the Institutional Review Board of each participating center. The trials were conducted in accordance with the SPIRIT guidelines. The protocols for these trials (NUH03iMCD and NUH04iMCD) have been published previously [12,13].
Participants
Recruitment was conducted between October 2019 and April 2021. Two patients diagnosed with tocilizumab-resistant iMCD were enrolled in this study, although the target enrollment was 20. The inclusion criteria were a definitive diagnosis of iMCD based on the Japanese diagnostic criteria and failure to achieve complete remission with tocilizumab treatment for more than eight weeks. Patients were required to be ≥ 18 years of age and maintain a stable dose of corticosteroids prior to the start of the study. The exclusion criteria were designed to eliminate patients with a high risk of adverse outcomes due to drug or disease-related complications.
Randomization and blinding
The participants were randomly assigned in a 1:1 ratio to receive sirolimus or placebo. Randomization was implemented using a biased coin design with an imbalanced tolerance to maintain allocation concealment and treatment balance. The initial phase maintained a double-blind structure, with both the participants and investigators being unaware of the treatment assignments.
Interventions
In the controlled trial phase, the assigned medication was administered orally at a daily dose, with the sirolimus group receiving 2 mg of sirolimus once daily for 16 weeks. The extension phase involved open-label administration of sirolimus, in which both patients, regardless of their initial assignment, were administered sirolimus under the same dosing schedule.
Outcomes
The primary endpoint was the change in the CHAP (CRP, Hemoglobin, Albumin, Performance Status) score from the baseline to week 16. The CHAP score is a validated disease activity assessment tool specifically developed for iMCD by Fujimoto et al. [5]. The score integrates four key disease parameters: CRP (C-reactive protein), Hemoglobin, Albumin, and Performance Status (ECOG), each graded on a five-point scale (0-4). The total score, therefore, ranges from 0 to 16. Secondary outcomes included hemoglobin, albumin, and CRP levels; changes in lymph node size; patient and physician global assessment; and safety parameters, including adverse events. In the extension phase, these outcomes were monitored to assess the long-term efficacy and safety of the treatment. Secondary outcomes included hemoglobin, albumin, and CRP levels; changes in lymph node size; patient and physician global assessment; and safety parameters, including adverse events. In the extension phase, these outcomes were monitored to assess the long-term efficacy and safety of the treatment.
Sample size and statistical considerations
The study was originally designed to enroll 20 participants (10 per group) based on feasibility considerations, given the rarity of tocilizumab-resistant iMCD. This sample size was determined through consultation with iMCD experts and consideration of patient availability across the participating centers, rather than formal power calculations. This study was designed as a proof-of-concept trial to generate preliminary efficacy and safety data to inform future larger studies.
Early termination and modified analysis plan
The trial was terminated early after enrolling only two participants due to (1) unexpected difficulties in obtaining matching placebo supplies when the manufacturer changed the sirolimus formulation and (2) recruitment challenges exacerbated by the COVID-19 pandemic, which significantly reduced patient willingness to participate in clinical trials requiring frequent hospital visits. Given the extremely small sample size, formal statistical hypothesis testing was not conducted. Instead, descriptive analyses were conducted, and the results are presented as individual patient trajectories and summary statistics. The analysis focused on documenting safety outcomes and exploring preliminary efficacy signals to inform future trial designs.
Safety monitoring
Adverse events were monitored and recorded throughout the trial and extension phases. All events were categorized according to their severity and relationship with the study drug. Clinical examinations, laboratory assessments, and other medically important indicators were systematically documented.
Data collection and management
Clinical data were collected and managed using an electronic data capture system compliant with Japan's Good Clinical Practice guidelines. Patient confidentiality was strictly maintained throughout the study, with anonymized and securely stored data being used.
Ethical considerations
The study protocol was approved by the institutional review boards of each site, and all participants provided written informed consent prior to participation. This study was conducted in accordance with the Declaration of Helsinki and other relevant ethical guidelines.
Results
Participant enrollment and characteristics
As shown in Figure 1, in the preliminary trial (NUH03iMCD), four cases of consent were obtained and screened, of which two patients were enrolled and one was allocated to the study drug group and one to the placebo group. In addition, two patients dropped out of the study due to withdrawal of consent from the patient and failure to meet the eligibility criteria. Two patients with tocilizumab-refractory iMCD were randomized 1:1 to receive either sirolimus or a placebo. Notably, the study was prematurely terminated because of unexpected difficulties in obtaining placebo supplies. These challenges were further compounded by the COVID-19 pandemic, which significantly hindered participant recruitment and retention, preventing us from reaching the target enrollment of 20 patients.
Participant flow diagram.This figure illustrates the flow of participants through a clinical trial. Starting with the initial screening and moving through subsequent phases of the trial, including enrollment, randomization, and follow-up, the diagram details the number of participants at each stage.
In the LTE trial (NUH04iMCD), participants who had completed the 16-week double-blind phase were included in a long-term safety and efficacy study of sirolimus. The study included one participant (C04-01 from the sirolimus group) at Kyoto University Hospital and another (C06-02 from the placebo group) at Daini Osaka Police Hospital. After the initial 16-week double-blind phase, the participant (C06-02), originally in the placebo group, began receiving sirolimus. Owing to the premature termination of the trial, all participants were eventually classified as discontinued subjects. The patient demographics and baseline characteristics are shown in Table 1.
Treatment exposure and compliance
Both participants completed the full 16-week double-blind phase with excellent medication adherence (99.2% for C04-01, 100% for C06-02). Subsequently, both enrolled in the extension phase receiving open-label sirolimus for an additional 24-40 weeks, with total treatment durations of 413 days (C04-01) and 420 days (C06-02). Sirolimus blood levels confirmed adequate drug exposure throughout both study phases (Table 2).
Primary outcome in the 16-week, double-blind phase (NUH03iMCD trial)
Table 3 shows the longitudinal clinical and laboratory data of the two participants enrolled in the NUH03iMCD trial. The primary efficacy endpoint, defined as a decrease of ≥1 in the CHAP score from baseline to 16 weeks, was not observed in either participant. Specifically, the sirolimus-treated patient (C04-01) had a stable CHAP score of 1 at both the baseline and week 16, indicating no change. In contrast, the placebo-treated patient (C06-02) experienced an increase in the CHAP score from 3 at baseline to 5 at week 16, suggesting disease progression rather than improvement. These results did not meet the predefined criterion for efficacy based on the CHAP score reduction within the 16-week treatment period.
Secondary outcomes
The secondary endpoints were laboratory markers and overall well-being. At week 16, neither group showed a reduction in hemoglobin (Hb), albumin (Alb), or C-reactive protein (CRP) levels from baseline. The physician's general assessment of disease activity showed a decrease in the sirolimus-treated patients and an increase in the placebo group, indicating an improvement and worsening of perceived disease activity, respectively. However, the patient self-assessment did not show any decrease in disease activity in either group (Table 4).
Regarding the SF-36 quality of life scores, sirolimus-treated patients showed an increase in the bodily pain (BP), general health (GH), emotional role (RE), and mental health (MH) subscales, suggesting an improved quality of life. The physical functioning (PF) and social functioning (SF) subscales remained unchanged. The placebo group experienced a decrease in all SF-36 subscale scores, implying a decline in quality of life (Table 5).
Throughout the study period, including the 16-week double-blind phase and the long-term extension phase (up to 420 days), systematic clinical and radiological assessments revealed no measurable lymph node enlargement or organomegaly in either participant. Neither participant achieved a complete response (CR) or partial response (PR) at week 16 based on the Castleman Disease Collaborative Network (CDCN) treatment response criteria. The CHAP score and the CHAP score minus the CRP score did not decrease from baseline for either participant.
Figure 2 illustrates the changes in CHAP scores and CRP levels throughout the course of the study, dividing the observations into RCT and LTE phases. As shown in Figure 2A, the CHAP scores for participant C04-01 remained stable and low throughout both the phases, indicating consistent disease control. In contrast, the CHAP scores in participant C06-02, which were initially high during the RCT phase, showed a significant decrease after transitioning into the LTE phase, reflecting an improvement in disease symptoms with extended treatment. Figure 2B depicts the CRP levels, where participant C04-01 maintained low inflammatory markers throughout the study, whereas participant C06-02 exhibited fluctuating but overall decreasing CRP levels in the LTE phases, further correlating with the clinical improvement observed in the LTE phase.
Longitudinal CHAP scores and CRP levels during RCT and LTE phases for participants C04-01 and C06-02.(A) CHAP score trajectories for participants C04-01 (represented by squares) and C06-02 (represented by circles) across the randomized controlled trial (RCT) phase and long-term extension (LTE) phase of the study. (B) CRP level trajectories for the same participants over the same period, showing the inflammatory response along with treatment administration.
Safety outcomes
No serious adverse events were reported during either study phase. Mild adverse events included aphthous ulcers (considered possibly related to sirolimus), oral herpes, gastroenteritis, vaccination-related symptoms, and minor musculoskeletal complaints. All events were Grade 1-2 in severity. Laboratory monitoring revealed no clinically significant abnormalities attributable to study medication. The extended treatment duration (up to 420 days) provided valuable long-term safety data supporting the tolerability of sirolimus in this patient population.
Discussion
Recent studies have revealed that iMCD involves not only excessive IL-6 signaling but also aberrant activation of the PI3K/AKT/mTOR pathway, which regulates cell growth, metabolism, and immune responses [14]. In particular, mTORC1 and mTORC2 activation has been demonstrated in lymph nodes from patients with iMCD-TAFRO, providing a biological rationale for mTOR inhibition [15]. Sirolimus, an mTOR inhibitor, may exert therapeutic effects by suppressing abnormal lymphoproliferation and cytokine production, thereby stabilizing disease activity in refractory cases [16,17].
This exploratory study represents the first prospective evaluation of sirolimus in tocilizumab-resistant iMCD, despite premature termination with only two participants. While the extremely small sample size prevents definitive efficacy conclusions, the contrasting disease trajectories observed between treatment groups and the systematic improvement when the placebo patient switched to sirolimus provide meaningful insights into the potential therapeutic role of mTOR inhibition in this challenging patient population.
The lack of CHAP score reduction in the sirolimus-treated patient prompts a discussion on the interpretation of 'efficacy' in a complex disease like iMCD, where stabilization might be as clinically significant as reduction, particularly in a disease known for its debilitating flares and progressive deterioration [4,18]. Hence, the stable CHAP score observed might suggest a beneficial effect of sirolimus, which was not captured by the stringent criteria of the primary endpoint. Although primary efficacy based on the CHAP score was not observed, secondary outcomes provided mixed signals. Physician-assessed improvement in the sirolimus-treated patient and quality of life measures that improved or remained stable in certain domains contrasted with the worsening condition in the placebo-treated patient.
Moreover, the improvement observed in the CHAP score as well as the CRP level during open-label LTE in the patient initially assigned to the placebo group further supports the potential efficacy of sirolimus. These outcomes imply a positive trend for sirolimus in managing iMCD, suggesting a suppressive effect on disease activity over time.
The fact that sirolimus was well tolerated with no new safety concerns arising over the long-term treatment period is also encouraging. The adverse events observed were consistent with the known safety profile of sirolimus, and none led to treatment discontinuation, indicating that sirolimus could be a viable option for patients who have exhausted other treatment options.
There are several recognized types of Castleman’s disease, including the hyaline vascular type, plasma cell type [18,19], and the more recently described TAFRO syndrome, which includes thrombocytopenia, anasarca, fever, reticulin fibrosis, and organomegaly [20,21]. The current trial did not enroll patients with a severe phenotype that is often associated with TAFRO syndrome [22-24]. However, the effectiveness of sirolimus has been demonstrated not only in iMCD-TAFRO [16], but also in iMCD-NOS (not otherwise specified) [6], suggesting a broader therapeutic potential for this treatment. The results of this trial support the findings of the previous case reports.
Unfortunately, this trial was prematurely concluded after enrolling only two participants, largely because of difficulties in obtaining placebo supplies. The supplier had to change the formulation of the sirolimus tablets, making it impossible to produce matching placebo tablets. Additionally, the spread of the COVID-19 pandemic significantly contributed to the challenges faced, particularly influencing patient reluctance towards frequent hospital visits, which further complicated trial execution.
We acknowledge several important limitations: (1) the extremely small sample size precludes statistical analysis; (2) early termination may introduce selection bias; (3) baseline differences between participants limit comparative interpretation; (4) single-country recruitment may limit generalizability; and (5) the lack of formal interim analysis plan for early termination decisions.
Conclusions
In conclusion, although definitive conclusions on the long-term safety and efficacy of sirolimus in patients with tocilizumab-insufficiently responsive iMCD cannot be drawn from this trial alone, there were indications of efficacy, as evidenced by partial improvements in the CHAP scores and physicians’ global assessments. Over a period exceeding one year, the continuous administration of sirolimus did not raise any new safety concerns, suggesting a favorable safety profile for long-term use. In addition, the historical data collected in this stringent trial environment could be instrumental in guiding future research and improving patient care strategies for iMCD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Localized mediastinal lymphnode hyperplasia resembling thymoma Cancer CAB IVL MEVP 82283091956 https://pubmed.ncbi.nlm.nih.gov/13356266/1335626610.1002/1097-0142(195607/08)9:4<822::aid-cncr 2820090430>3.0.co;2-4 · doi ↗ · pubmed ↗
- 2Pathogenic significance of interleukin-6 (IL-6/BSF-2) in Castleman's disease Blood Yoshizaki K Matsuda T Nishimoto N 13601367741989 https://pubmed.ncbi.nlm.nih.gov/2788466/2788466 · pubmed ↗
- 3A benefit and the prospects of IL-6 inhibitors in idiopathic multicentric Castleman's disease Mod Rheumatol Koga T Sumiyoshi R Kawakami A Yoshizaki K 3023052920193028551610.1080/14397595.2018.1532383 · doi ↗ · pubmed ↗
- 4HHV-8-negative, idiopathic multicentric Castleman disease: novel insights into biology, pathogenesis, and therapy Blood Fajgenbaum DC van Rhee F Nabel CS 2924293312320142462232710.1182/blood-2013-12-545087 · doi ↗ · pubmed ↗
- 5Tentative diagnostic criteria and disease severity classification for Castleman disease: a report of the research group on Castleman disease in Japan Mod Rheumatol Fujimoto S Koga T Kawakami A 1611672820182888069710.1080/14397595.2017.1366093 · doi ↗ · pubmed ↗
- 6A case of tocilizumab-refractory idiopathic multicentric Castleman's disease successfully treated with sirolimus Clin Immunol Sumiyoshi R Koga T Furukawa K Umeda M Yamamoto K Mori R Kawakami A 10888723320213479824010.1016/j.clim.2021.108887 · doi ↗ · pubmed ↗
- 7m TOR signaling in growth, metabolism, and disease Cell Saxton RA Sabatini DM 96097616820172828306910.1016/j.cell.2017.02.004PMC 5394987 · doi ↗ · pubmed ↗
- 8Sirolimus for GVHD prophylaxis in allogeneic stem cell transplantation Bone Marrow Transplant Cutler C Antin JH 4714763420041527370810.1038/sj.bmt.1704604 · doi ↗ · pubmed ↗