Pulmonary Metastasis of Anal Squamous Cell Carcinoma Nine Years Following Treatment
Maxwell S Madani, Anushka Deogaonkar, Athanasios S Naum, Robert Gordon, Marie L Borum

TL;DR
A rare case of anal cancer spreading to the lungs nine years after treatment is reported, highlighting the long-term risks in HIV patients with poor antiretroviral therapy adherence.
Contribution
This paper presents a rare case of delayed pulmonary metastasis in anal squamous cell carcinoma, emphasizing long-term oncologic risks in HIV patients with inconsistent HAART adherence.
Findings
A 51-year-old HIV-positive man developed pulmonary metastasis nine years after curative chemoradiation for anal squamous cell carcinoma.
The metastasis was HPV-associated and confirmed via biopsy, with no local recurrence detected.
The case raises concerns about the impact of intermittent HAART adherence on long-term cancer outcomes in immunocompromised patients.
Abstract
Squamous cell carcinoma of the anus (SCCA), the predominant histologic subtype of anal cancer, is associated with human papillomavirus (HPV) infection in over 90% of cases. The risk of SCCA is markedly elevated in individuals with HIV, particularly those experiencing advanced or prolonged immunosuppression. Most local recurrences occur within three to five years of initial treatment, while distant metastases develop in 10-20% of patients following curative therapy. At diagnosis, distant metastases are identified in only 5-8% of cases. Prognosis varies significantly by stage, with a five-year overall survival of approximately 78% in localized disease and 19% in cases with distant metastasis. We report a rare case of delayed pulmonary metastasis of SCCA in a 51-year-old man with HIV and a history of inconsistent adherence to highly active antiretroviral therapy (HAART). The patient had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
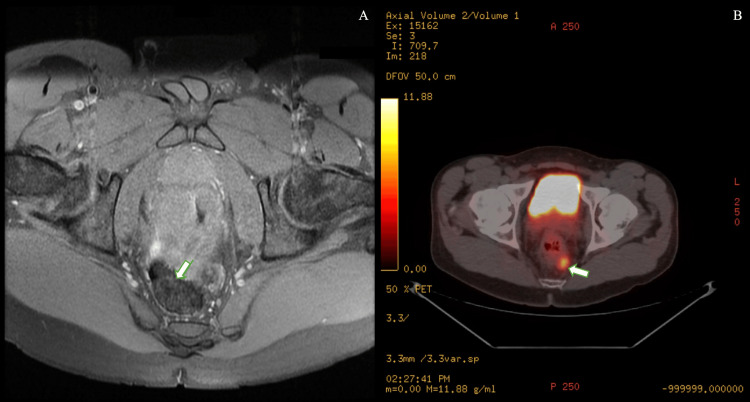 Figure 1
Figure 1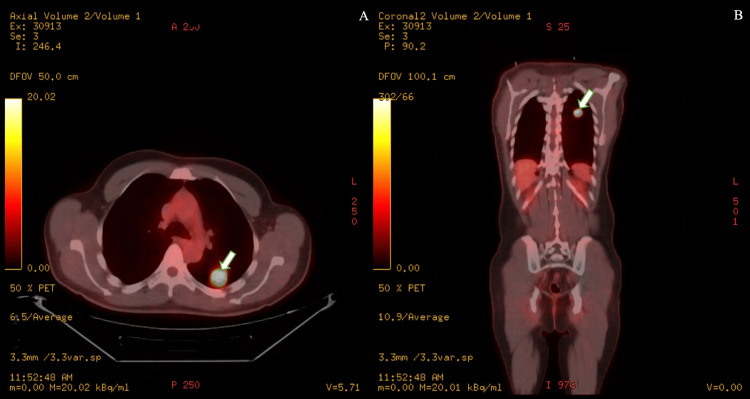 Figure 2
Figure 2| Timeline of Disease Course | |
| Year | Event |
| 2014 | Diagnosis of SCCA, HIV-positive, nonadherent to HAART |
| 2014 | Definitive chemoradiation (5-FU + mitomycin-C) |
| 2017 | PET/CT showed complete metabolic resolution |
| 2017-2023 | Regular surveillance, no recurrence |
| 2023 | Multiple interruptions in HAART due to psychosocial stress |
| 2025 | Pulmonary recurrence, 2.7 cm lung nodule |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal and Anal Carcinomas · Cervical Cancer and HPV Research · Genital Health and Disease
Introduction
Squamous cell carcinoma of the anus (SCCA), the most common histologic subtype of anal cancer, is driven by human papillomavirus (HPV) infection in over 90% of cases [1,2]. Additional risk factors include HIV infection, age, sex, ethnicity, reproductive history, healthcare access, environmental and geographic conditions, genetic predisposition, and other medical conditions that may affect immune function [3]. Individuals with HIV, particularly those with advanced immunosuppression, are at markedly increased risk of developing SCCA [4]. The incidence of SCCA has risen at approximately 2.7% annually over the past decade [5].
Most local recurrences occur within three to five years of diagnosis, and the risk of distant metastasis following curative local treatment is 10-20%. At presentation, distant metastases are observed in only 5-8% of cases [6,7]. The most common metastatic sites include the liver and lungs, followed by extra-pelvic lymph nodes, peritoneum, and bone [4]. Five-year overall survival for localized disease is ~78%, compared with 19% in patients with distant metastasis [8].
Late metastasis beyond five years is rare. A small number of published cases have described delayed pulmonary metastasis after seven to eight years [3]. To our knowledge, a nine-year disease-free interval to metastasis represents one of the longest reported intervals in the literature, highlighting the clinical significance of this case.
Case presentation
A 43-year-old man with HIV initially presented to the emergency department with progressive rectal pain and drainage of several months’ duration. He had discontinued highly active antiretroviral therapy (HAART) due to psychosocial stress but later resumed therapy (ritonavir, darunavir, dolutegravir, and tenofovir/emtricitabine).
Examination findings
A 3×2 cm friable, fixed mass was palpated in the posterior midline on digital rectal exam. No externalized mass or palpable peripheral lymphadenopathy was noted. The patient had mild weight loss at the time but no systemic symptoms. Laboratory results showed normal lactate dehydrogenase (LDH) and normal inflammatory markers (C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)).
Imaging
Pelvic MRI revealed a 1.7 cm enhancing lesion in the left supralevator space and diffuse thickening of a 7 cm distal rectal/anorectal segment (Figure 1A). Biopsy confirmed moderately differentiated invasive squamous cell carcinoma with positive margins. Staging CT and 18-F-fluorodeoxyglucose positron emission tomography/computed tomography (18-F-FDG PET/CT) demonstrated a hypermetabolic anorectal mass (standardized uptake value (SUV) 12.1) and a 1.8 cm hypermetabolic perirectal lymph node, without distant disease (Figure 1B).
A) A 1.7 cm enhancing soft tissue lesion in the left supralevator space adjacent to the rectosigmoid junction. B) A 1.8 cm hypermetabolic left perirectal lymph node (maximum SUV=7.6).SUV, standardized uptake value
The patient underwent definitive chemoradiation with 5-fluorouracil and mitomycin-C (Table 1). Follow-up PET/CT more than two years after definitive treatment showed a complete metabolic response. Proctoscopy performed every six to 12 months over the next several years showed no recurrence.
Metastasis
At age 51, nine years post-treatment, he presented with night sweats, chills, chest pain, abdominal pain, hematochezia, and unintentional weight loss. He was afebrile and hemodynamically stable. Laboratory results showed hemoglobin 10.2 g/dL, CD4 512 cells/mm^3^, and normal LDH and CRP levels.
CT angiography revealed a 2.7 cm solid nodule with spiculated borders in the left lower lobe. CT-guided biopsy confirmed squamous cell carcinoma positive for P40 and P16, consistent with HPV-associated disease. 18-F-FDG PET/CT showed intense uptake in the lesion (SUV 17.2), with no other sites of disease (Figure 2). Colonoscopy identified two benign tubular adenomas (resected) and one hyperplastic rectal polyp (resected). No evidence of local recurrence was seen. Tumor markers were unremarkable.
Hyperbolic left lower lobe lung nodule with a maximum SUV of 17.2; A) axial view, B) coronal view.SUV, standardized uptake value
Management
The multidisciplinary review considered surgery. However, surgical resection was deferred because the patient’s HIV-associated immunosuppression, prior pelvic radiation, and comorbidities made systemic therapy preferable. He was started on carboplatin (area under the curve (AUC) 5) and paclitaxel (80 mg/m² on days 1, 8, and 15 of each 28-day cycle) plus retifanlimab (anti-PD-1). Treatment was complicated by immune-mediated hepatitis, requiring discontinuation of immunotherapy. Chemotherapy was resumed after the resolution of liver enzyme abnormalities.
Discussion
Anal carcinoma most commonly presents with symptoms such as rectal bleeding, anal pain, changes in bowel habits, or the presence of a palpable mass. Accurate diagnosis and effective treatment require a thorough understanding of anal anatomy and lymphatic drainage patterns, and early detection is critical for improving prognostic outcomes. While clinical evaluation and imaging are essential components of the diagnostic workup, anoscopy with biopsy remains the gold standard for obtaining histopathologic confirmation.
Treatment typically involves a multidisciplinary approach, including surgical resection, radiation therapy, and chemotherapy [4]. Metastatic anal cancer at presentation is relatively less common and represents a therapeutic challenge, as this population has a poor prognosis, with five-year overall survival rates estimated at approximately 10% in men and 20% in women [8]. Poor prognostic factors include male sex, age over 65 years, advanced T stage, nodal involvement, and poorly differentiated tumor histology [9]. The standard first-line systemic therapy for metastatic disease remains a combination of cisplatin and 5-fluorouracil. Despite the emergence of several small, non-randomized phase II trials, there has been minimal therapeutic advancement in the management of metastatic SCCA over the past two decades [10].
This report highlights a rather interesting aberration from the usual recurrence timeline of three to five years, without any evidence of locoregional manifestations. It is essential to note that immunosuppressed patients have poor tolerance of chemotherapy and response to chemoradiation, and an increased rate of recurrence, along with unique displays of tumor recurrence [11].
Notably, this patient’s history of intermittent HAART adherence due to psychosocial stressors likely contributed to his sustained immunosuppression, as reflected by his fluctuating antiretroviral regimens and multiple hospitalizations over the years. At the time of metastasis, he had a CD4 count of 512 cells/mm³ yet exhibited symptoms and radiologic findings concerning malignancy. His diagnosis of HPV-positive pulmonary squamous cell carcinoma was confirmed on biopsy, and PET/CT demonstrated no additional sites of disease.
The patient initially opted for aggressive systemic therapy with carboplatin, paclitaxel, and the PD-1 inhibitor retifanlimab. During treatment, he developed immune-related hepatitis, characterized by elevated liver enzymes (AST and ALT >5 × upper limit of normal). Retifanlimab was temporarily discontinued while supportive care, including corticosteroids, was administered. Chemotherapy with carboplatin and paclitaxel was also paused briefly during the acute phase. Once liver function tests normalized, chemotherapy was resumed, while immunotherapy remained on hold until reassessment by the oncology team.
Diagnosis of metastatic anal SCC was confirmed by immunohistochemical staining for P40 and P16, which are instrumental in distinguishing HPV-associated anal SCC metastases from primary pulmonary squamous cell carcinoma. P40, a sensitive marker for squamous differentiation, and P16, a surrogate for oncogenic HPV infection, are typically co-expressed in metastatic anal SCC. In contrast, primary pulmonary SCC often exhibits P40 positivity without corresponding P16 expression. This differential expression pattern aids in accurately identifying the origin of lung lesions [3,12].
This case highlights several important clinical points. First, late metastasis can occur long after standard surveillance windows, particularly in immunocompromised patients. Second, intermittent HAART adherence may contribute to sustained immunosuppression and potentially influence tumor recurrence patterns. Finally, immunohistochemical markers such as P40 and P16 provide critical diagnostic guidance when evaluating pulmonary lesions in patients with a history of HPV-associated SCCA. Clinicians should maintain a high index of suspicion for metastatic disease in similar patients, and long-term surveillance strategies may need to be tailored to account for these risks.
Conclusions
The interplay between the use of immunosuppressive antiretroviral medications to prevent life-threatening complications of HIV and neoplastic recurrence in HIV-positive cancer survivors is complex and evolving. This case of unusually late metastatic recurrence underscores the need for further research on strategies to reduce relapse risk while supporting sustained HAART adherence. It also serves as a clinical reminder: when evaluating new nodules in immunocompromised patients, clinicians should maintain a high index of suspicion for metastasis, even in the absence of locoregional disease. Early consideration may accelerate diagnosis and improve long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Recent trends in squamous cell carcinoma of the anus incidence and mortality in the United States, 2001-2015 J Natl Cancer Inst Deshmukh AA Suk R Shiels MS 82983811220203174263910.1093/jnci/djz 219PMC 7825484 · doi ↗ · pubmed ↗
- 2RE: autoimmune disease and the risk of anal cancer in the US elderly population J Natl Cancer Inst Mahla RS 33833911620243780292210.1093/jnci/djad 204 · doi ↗ · pubmed ↗
- 3Stage IV anal canal squamous cell carcinoma with long-term survival: a case report Surg Case Rep Sawai K Goi T Tagai N 119820223572376510.1186/s 40792-022-01474-x PMC 9209564 · doi ↗ · pubmed ↗
- 4Therapy for squamous-cell carcinoma of the anus in HIV-positive patients ESMO Gastrointest Oncol 6 2025 Evin C Camandaroba MPG Riechelmann RP Huguet F 2025 http://ncbi.nlm.nih.gov/books/NBK 441891/
- 5Outcomes of anus squamous cell carcinoma. Management of anus squamous cell carcinoma and recurrences Dig Liver Dis Marref I Romain G Jooste V 149214985320213419336610.1016/j.dld.2021.05.028 · doi ↗ · pubmed ↗
- 6Metastatic or locally recurrent anal squamous cell carcinoma (SCAC): current clinical trial landscape and novel approaches Cancer Manag Res Rogers JE Leung M Johnson B 206520771420223576182310.2147/CMAR.S 331429 PMC 9233494 · doi ↗ · pubmed ↗
- 7Rectal squamous cell carcinoma in immunosuppressed populations: is this a distinct entity from anal cancer?AIDS Coghill AE Shiels MS Rycroft RK 1051123020162637248210.1097/QAD.0000000000000873 PMC 4703472 · doi ↗ · pubmed ↗
- 8Overview of recent trends in the management of metastatic anal cancer World J Oncol Yellu M Deeb A Olowokure O 311315620152914742310.14740/wjon 866w PMC 5649953 · doi ↗ · pubmed ↗