Right-to-Left Shunt via a Patent Foramen Ovale Triggered by Constrictive Pericarditis With Right Heart Compression: A Case Report
Takeshi Yamashita, Hanako Yoshihara Kurihara, Tamami Watanabe, Kenichi Sugisaki, Takahiko Fukuchi

TL;DR
A rare case shows how constrictive pericarditis can cause a heart defect to allow blood clots to bypass the lungs, leading to a stroke.
Contribution
This case report identifies constrictive pericarditis as a novel trigger for right-to-left shunting through a patent foramen ovale.
Findings
Constrictive pericarditis elevated right atrial pressure, unmasking a silent patent foramen ovale.
Surgical removal of the pericardial hematoma resolved the shunt and hypoxemia.
The patient experienced no recurrence of paradoxical embolism after treatment.
Abstract
We report a rare case of a right-to-left shunt through a patent foramen ovale (PFO) triggered by constrictive pericarditis secondary to an organized pericardial hematoma. A 72-year-old woman presented with thoracic back pain and subsequently developed persistent hypoxemia following idiopathic pericarditis. Despite appropriate anti-inflammatory and antimicrobial therapy, she experienced a cerebral embolism involving the right middle cerebral artery territory on hospital day 50. Imaging studies revealed a pericardial effusion compressing the right heart. Intraoperative transesophageal echocardiography confirmed a right-to-left shunt through a PFO. Surgical evacuation of the organized pericardial hematoma relieved right heart compression, normalized intracardiac pressures, and resolved the shunt. The pericardium was markedly thickened and adherent to the right ventricle with a fibrotic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
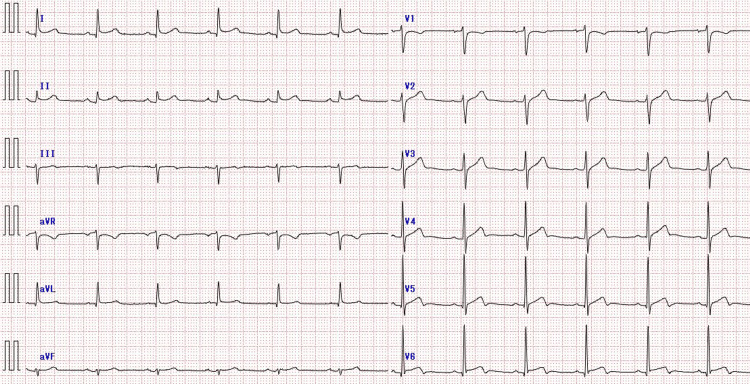 Figure 1
Figure 1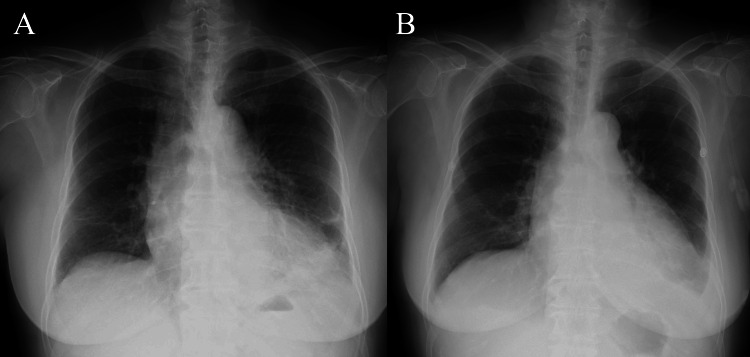 Figure 2
Figure 2 Figure 3
Figure 3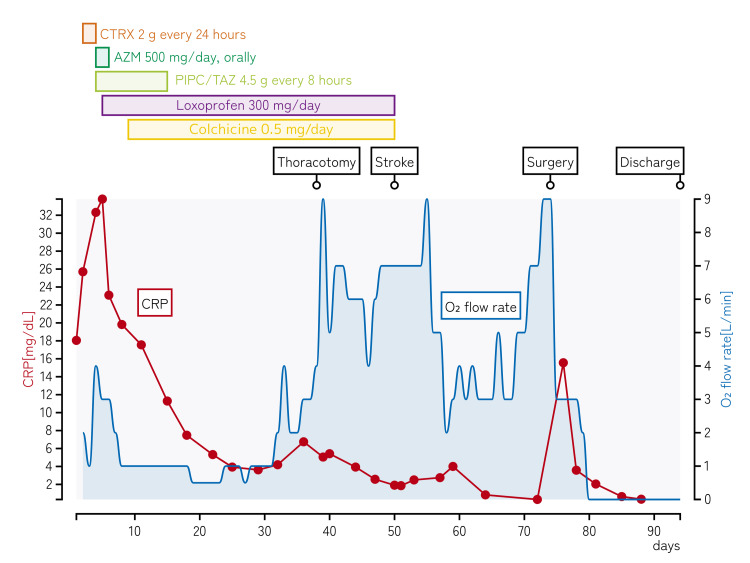 Figure 4
Figure 4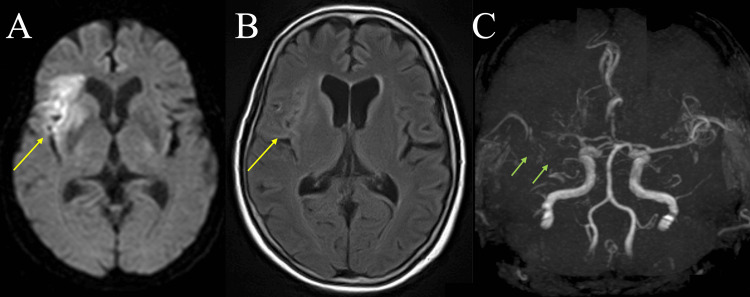 Figure 5
Figure 5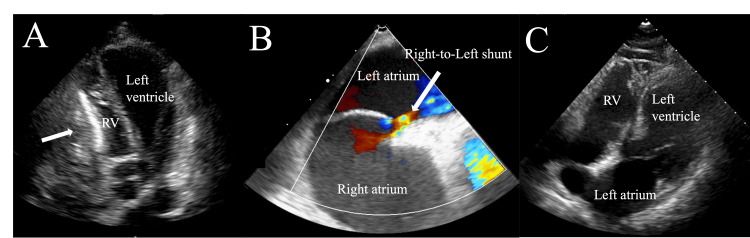 Figure 6
Figure 6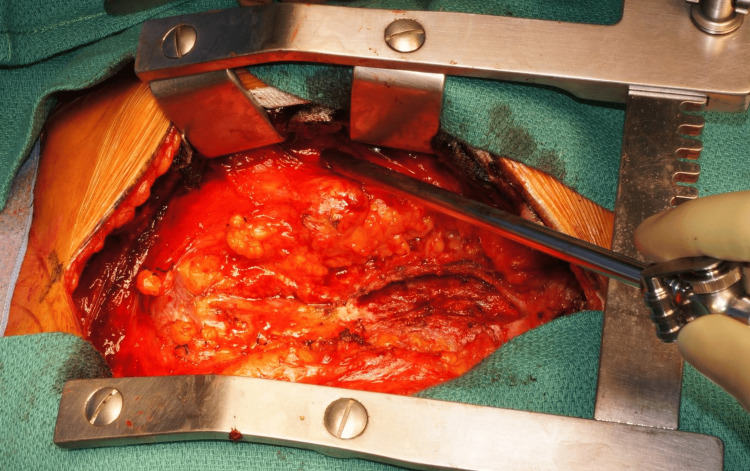 Figure 7
Figure 7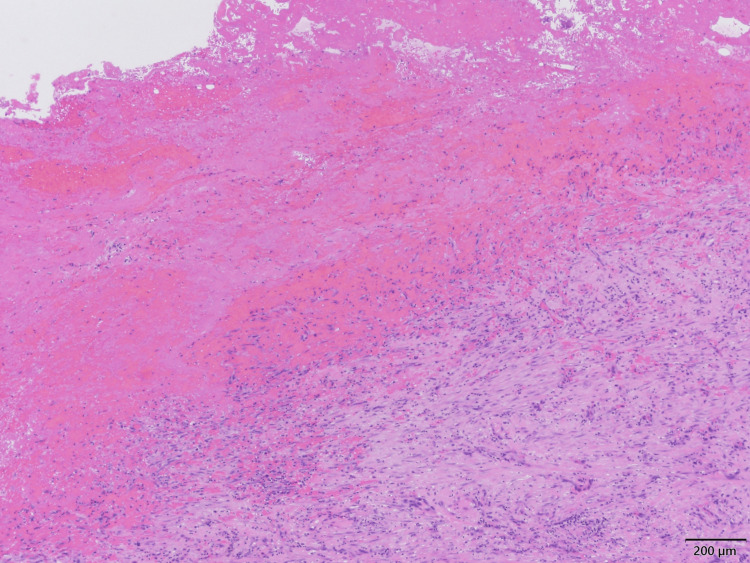 Figure 8
Figure 8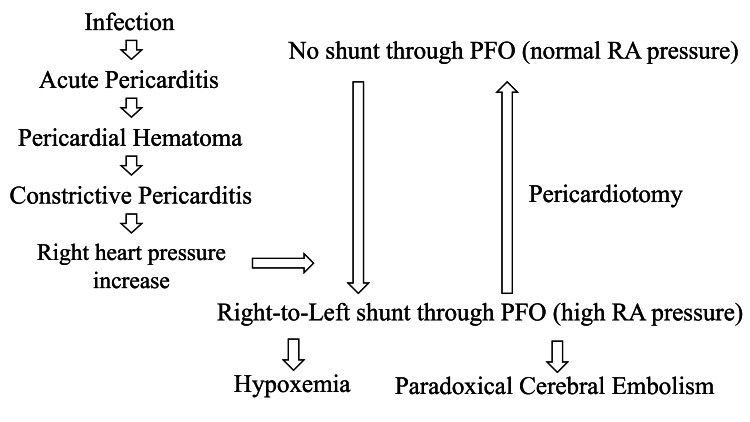 Figure 9
Figure 9| Parameter | Admission | Reference range |
| Complete blood count | ||
| White blood cell | 25.8×103/µL | 3.5-9.1×103/µL |
| Neutrophils | 88% | 40-74% |
| Lymphocytes | 5% | 19-48% |
| Monocytes | 7% | 3.4-9% |
| Eosinophils | 0% | 0-7% |
| Red blood cell | 343×104/µL | 376-500×104/µL |
| Hemoglobin | 10.7 g/dL | 11.3-15.2 g/dL |
| Hematocrit | 31.5% | 33.4-44.9% |
| Mean corpuscular volume | 91.8 fL | 79-100 fL |
| Platelet | 34×104/µL | 13-36.9×104/µL |
| Biochemistry | ||
| Total protein | 6.2 g/dL | 6.6-8.1 g/dL |
| Albumin | 2.6 g/dL | 4.1-5.1 g/dL |
| Total bilirubin | 0.68 mg/dL | 0.4-1.5 mg/dL |
| Direct bilirubin | 0.36 mg/dL | 0.05-0.23 mg/dL |
| AST | 33 U/L | 13-30 U/L |
| ALT | 47 U/L | 7-23 U/L |
| LD | 194 U/L | 124-222 U/L |
| Creatine kinase | 18 U/L | 41-153 U/L |
| Creatine kinase-MB fraction | 1 U/L | 0-25 U/L |
| ALP | 219 U/L | 106-322 U/L |
| γ-GT | 49 U/L | 9-32 U/L |
| C-reactive protein | 25.7 mg/dL | 0-0.14 mg/dL |
| Urea nitrogen | 21 mg/dL | 8-20 mg/dL |
| Creatinine | 1.03 mg/dL | 0.46-0.79 mg/dL |
| Sodium | 141 mmol/L | 138-145 mmol/L |
| Potassium | 4.4 mmol/L | 3.6-4.8 mmol/L |
| Chloride | 105 mmol/L | 100-110 mmol/L |
| Corrected calcium | 9.7 mg/dL | 8.4-10.1 mg/dL |
| Inorganic phosphorus | 5.2 mg/dL | 2.7-4.6 mg/dL |
| Magnesium | 1.9 mg/dL | 1.7-2.5 mg/dL |
| Plasma glucose | 113 mg/dL | 70-109 mg/dL |
| Troponin I | 62.9 pg/mL | <6 pg/mL |
| Brain natriuretic peptide | 58.6 pg/mL | 0-18.4 pg/mL |
| Antinuclear antibody | <40 times | <40 times |
| Coagulation tests | ||
| PT-INR | 1.16 | 0.9-1.2 |
| APTT | 38.4 seconds | 28.5-40.9 seconds |
| D-dimer | 2.9 µg/mL | 0-1 µg/mL |
| Urinalysis and sediments | ||
| Gravity | 1.056 | 1.005-1.025 |
| pH | 5.0 | 5.0-7.5 |
| Protein | 1+ | Negative |
| Glucose | - | Negative |
| Red blood cells | 5-9/HPF | 0-2/HPF |
| White blood cells | 1-4/HPF | Negative |
| Blood culture | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Pericarditis and Cardiac Tamponade · Infective Endocarditis Diagnosis and Management
Introduction
Patent foramen ovale (PFO) is a common congenital interatrial communication present in approximately 15-35% of the adult population [1]. Although often asymptomatic, a PFO can serve as a conduit for paradoxical embolism, particularly when right atrial pressure is elevated, such as in the setting of pulmonary embolism or right heart failure or during the Valsalva maneuver [1,2]. Paradoxical embolism through a PFO can lead to ischemic stroke, systemic embolization, or unexplained hypoxemia [3-6].
PFO results from the incomplete fusion of the septum primum and secundum [7]. Although it typically remains closed in function due to higher left atrial pressure [8], any condition that reverses this gradient can cause right-to-left shunting. The degree of shunting is influenced by defect size and pressure differential [7,9].
Constrictive pericarditis, a chronic inflammatory disorder characterized by the fibrotic thickening of the pericardium and impaired diastolic filling, can lead to elevated right-sided cardiac pressures [10]. Recent expert consensus from the American College of Cardiology has also emphasized early recognition and multimodal imaging for the diagnosis and management of pericardial diseases [11]. Asymmetric pericardial thickening or hematoma formation, especially in postsurgical settings, can selectively compress specific cardiac chambers, most notably the right atrium, further increasing right atrial pressure [12]. The hemodynamic sequelae of constrictive pericarditis include impaired venous return and elevated systemic venous pressure [13]. Right heart compression results in a disproportionate elevation of right atrial pressure while maintaining a relatively normal left atrial pressure, thereby creating the pressure gradient necessary for right-to-left shunting across the PFO [14]. However, the development of paradoxical embolism and hypoxemia due to this mechanism has rarely been reported. Imazio et al. noted that although constrictive pericarditis impairs cardiac filling and increases right-sided pressure, direct evidence of PFO-mediated shunting remains limited [15]. Similarly, Maloku et al. emphasized the diagnostic challenge, as pericardial diseases are infrequently considered precipitating factors for paradoxical embolisms [16].
This case report describes a rare instance of constrictive pericarditis secondary to an organized pericardial hematoma that developed after idiopathic pericarditis, resulting in a right-to-left shunt through a PFO and paradoxical cerebral embolism. To our knowledge, this is the first reported case demonstrating this sequential pathophysiological mechanism.
Case presentation
A 72-year-old Japanese woman presented with a six-day history of persistent thoracic back pain that worsened upon deep inspiration. At that time, she was afebrile. She visited a local clinic, where the electrocardiogram (ECG) showed ST-segment elevation. The patient was subsequently transported to our hospital by an ambulance.
Her medical history included hypertension and dyslipidemia, for which she was being treated with telmisartan and rosuvastatin. She was a non-smoker and reported drinking approximately 350 mL of beer twice a week.
On admission, her height was 163 cm, her weight was 56.9 kg, and her body mass index was 21.4 kg/m². The patient was alert and well-oriented. Her vital signs were as follows: temperature, 38.5℃; blood pressure, 96/50 mmHg; heart rate, 93 bpm with a regular rhythm; and respiratory rate, 22 breaths/min. Oxygen saturation was 98% on room air. Cardiac murmurs or pulmonary crackles were not observed.
Laboratory findings (Table 1) revealed marked leukocytosis with a white blood cell (WBC) count of 25,800/μL (88% neutrophils), elevated inflammatory markers with a C-reactive protein (CRP) level of 25.7 mg/dL, and a mildly elevated troponin I level (62.9 pg/mL).
The ECG showed ST-segment elevation in leads I, II, aVL, and V2-V6, without PR-segment depression (Figure 1).
ECG on admissionThe ECG showing ST-segment elevation in leads I, II, aVL, and V2-V6, without PR-segment depression.ECG: electrocardiogram
Chest X-ray demonstrated cardiomegaly and decreased transparency in the bilateral lower lung fields (Figure 2A).
Chest X-rays on admission and on day 17(A) Chest X-ray on admission showing cardiomegaly and decreased transparency in the bilateral lower lung fields. (B) Chest X-ray on day 17 showing slightly improved transparency in the bilateral lower lung fields compared with admission.
Contrast-enhanced computed tomography (CT) subsequently showed localized pericardial effusion compressing the right heart, multiple pulmonary nodular infiltrates in the left lung, and left pleural effusion (Figure 3A-3B).
Serial chest CT images demonstrating the evolution of pericardial hematoma(A) Chest CT showing multiple pulmonary nodular infiltrates in the left lung and left pleural effusion. (B) Initial contrast-enhanced CT image on admission showing circumferential pericardial effusion (yellow arrow). (C) Follow-up CT on hospital day 33 demonstrating an encapsulated pericardial collection adjacent to the right atrium (yellow arrow), with an attenuation of approximately 40 HU, suggestive of a hematoma. The dark structure anterior to the right ventricle represents pericardial fat. Left-sided pleural effusion is also present. (D) CT on hospital day 72 demonstrating a persistent encapsulated pericardial collection (yellow arrow) with dense contents adjacent to the right heart, compressing the cardiac chambers and contributing to elevated right atrial pressure. The attenuation measured approximately 50 HU, compatible with a chronic hematoma. The dark structure anterior to the right ventricle represents pericardial fat, and left-sided pleural effusion is also present.CT: computed tomography
The following day, coronary angiography revealed no significant stenosis. That same day, she developed a fever of 38°C, and based on the imaging findings, community-acquired pneumonia was diagnosed. Ceftriaxone (2 g every 24 hours) was initiated as empirical therapy.
By hospital day 4, laboratory tests showed no improvement in inflammation (WBC 25,000/μL and CRP 32.3 mg/dL), and oxygenation had not improved. Therefore, the antibiotic regimen was changed to azithromycin (500 mg/day, orally) and piperacillin/tazobactam (4.5 g every eight hours) to cover atypical pathogens and organisms not susceptible to ceftriaxone. Sputum culture later yielded Streptococcus pneumoniae and Haemophilus influenzae. Despite receiving 4 L/min supplemental oxygen, her SpO₂ decreased to 94%. Cardiac insufficiency secondary to pericarditis was suspected, and intravenous furosemide was initiated. The clinical course of the patient is shown in Figure 4.
Clinical course of the patientTimeline showing the clinical course during the 94-day hospitalization. The red line with dots represents CRP levels (left y-axis, mg/dL), and the blue line shows oxygen flow rate requirements (right y-axis, L/min). Horizontal bars indicate the duration of antimicrobial and anti-inflammatory therapies. Three major events are marked: thoracotomy (day 39), stroke (day 50), and surgery for pericardial hematoma evacuation (day 74). Note the persistent oxygen requirement despite improvement in CRP levels, which resolved only after surgical intervention.CRP: C-reactive protein; CTRX: ceftriaxone; AZM: azithromycin; PIPC/TAZ: piperacillin/tazobactam; NSAIDs: nonsteroidal anti-inflammatory drugs
On hospital day 5, loxoprofen (300 mg/day) was initiated for pericarditis-related chest pain, and on day 9, colchicine (0.5 mg/day) was added to treat the presumed idiopathic pericarditis.
By day 17, the levels of inflammatory markers had improved, and chest X-ray showed slightly improved transparency in the bilateral lower lung fields (Figure 2B). Piperacillin/tazobactam was discontinued after two weeks, following the treatment duration typically used for bacteremia. However, despite these improvements, significant hypoxemia persisted, requiring 4 L/min of oxygen. On day 29, follow-up transthoracic echocardiogram (TTE) revealed right-sided dominant pericardial effusion measuring approximately 22-26 mm in thickness anterior to the right ventricle with fibrinous strands, compressing the right heart. The inferior vena cava (IVC) was dilated with poor inspiratory collapse, and the right atrium was not collapsed, suggesting that cardiac tamponade had not yet developed. Contrast-enhanced CT scan on day 33 ruled out pulmonary embolism and deep vein thrombosis but showed that the pericardial effusion had become localized and encapsulated around the right heart (Figure 3C). These conditions were considered as possible causes of right heart pressure elevation, but their exclusion supported constrictive pericarditis as the underlying mechanism. Pericardiocentesis was not performed as no safe access sites were identified on echocardiography. On day 39, a left thoracotomy was performed through the fifth intercostal space to drain the pericardial effusion. The pericardium was incised, releasing a small amount of hemorrhagic effusion with dense adhesions in the cavity. The pericardial space was irrigated using a catheter, but the organized hematoma could not be drained. Pericardial biopsy showed pleural thickening with hemorrhage and inflammation, consistent with chronic pericarditis. The findings were not compatible with tuberculous pericarditis, and immunohistochemistry revealed no malignancy. Pericardial fluid cultures were negative.
On day 50 of hospitalization, the patient developed acute left-sided weakness. The National Institutes of Health Stroke Scale (NIHSS) score was 6 (facial palsy 2, left arm weakness 1, left leg weakness 2, dysarthria 1), and the modified Rankin Scale (mRS) score was 3. Brain magnetic resonance imaging (MRI) revealed multiple acute infarctions in the right middle cerebral artery (MCA) territory (Figure 5A-5C), consistent with cardioembolic stroke. Owing to the risk of bleeding, anticoagulation therapy was withheld, and only edaravone was administered.
Brain MRI and MRA findings demonstrating multiple embolic strokes(A-C) Brain MRI on hospital day 50. (A) Diffusion-weighted imaging showing a hyper signal intense lesion in the right basal ganglia (yellow arrow). (B) Fluid-attenuated inversion recovery image showing a lesion in the same region. (C) MRA showing the occlusion of the right middle cerebral artery (green arrow).MRI: magnetic resonance imaging; MRA: magnetic resonance angiography
On day 64, follow-up TTE showed persistent right-sided pericardial effusion and increased echogenicity of the pericardium, which was compressing the right ventricle. The IVC remained dilated with poor inspiratory collapse, and the right atrium was not collapsed, indicating that cardiac tamponade had still not developed (Figure 6A).
Echocardiographic evidence of right heart compression and intracardiac shunting(A) TTE, apical four-chamber view, showing the compression of the RV due to a pericardial hematoma (white arrow). (B) Intraoperative transesophageal echocardiogram with color Doppler showing right-to-left shunting through the patent foramen ovale with turbulent flow and a mosaic color pattern (white arrow). (C) Follow-up TTE apical four-chamber view on hospital day 82 showing the resolution of right-sided heart compression after the surgical removal of the hematoma.TTE: transthoracic echocardiogram; RV: right ventricle
The following day, her hemiparesis improved. The NIHSS score was 2 (facial palsy 1, dysarthria 1), and the mRS score was 1. Follow-up MRI showed decreased signal intensity on diffusion-weighted imaging with improved flow in the right MCA.
Given the persistent hypoxemia despite the resolution of systemic inflammation, presence of right heart compression on echocardiography, and occurrence of embolic strokes with no identifiable source, a right-to-left shunt was suspected. Although right heart catheterization was considered, it was anticipated that advancing the catheter into the pulmonary artery would be unsuccessful due to the significant compression of the right heart chambers. Because this compression was already evident on imaging and surgical intervention was considered inevitable, the decision was made to proceed directly with the surgery. On hospital day 68, a lung ventilation-perfusion scan showed no significant mismatch, effectively ruling out pulmonary embolism. Follow-up CT on day 72 confirmed a persistent hematoma that had become organized and caused significant compression of the right heart (Figure 3D).
On hospital day 74, the patient underwent pericardiotomy under general anesthesia. Intraoperative transesophageal echocardiography (TEE) confirmed a right-to-left shunt through the PFO (Figure 6B). The surgery was performed via a median sternotomy. The pericardium was markedly thickened and adherent to the right ventricle, and a fibrotic thrombus was firmly attached to the epicardial surface. The hematoma was completely removed except for the area near the inferior vena cava, where strong adhesion made further dissection hazardous due to the risk of venous injury. After decompression, right heart filling improved, although the right-to-left shunt through the PFO persisted immediately after surgery. The pericardium was left open, and the chest was closed in the usual manner (Figure 7).
Intraoperative photographIntraoperative photograph showing the operative field after the removal of the organized pericardial hematoma.
Histopathological examination revealed fibrotically thickened pericardial tissue with lymphocytic, plasma cell, and foamy cell infiltration. An attached hematoma showed organization and hemosiderin deposition, indicating a subacute to chronic process (Figure 8).
Histopathological findings of the pericardium Histopathological findings of the pericardium showing fibrotic thickening with inflammatory cell infiltration and an attached hematoma exhibiting organization and hemosiderin deposition (H&E stain, ×40).H&E: hematoxylin and eosin
On day 82, follow-up TTE confirmed the resolution of the right heart compression and showed no evidence of a right-to-left shunt (Figure 6C).
On hospital day 88, right heart catheterization showed pressures in the right atrium (mean 6 mmHg), right ventricle (end-diastolic pressure 9 mmHg), and pulmonary artery (mean 12 mmHg), with a pulmonary capillary wedge pressure of 5 mmHg. The right atrial and pulmonary capillary wedge pressures were nearly equal, no oxygen step-ups were observed, and there was no evidence of pulmonary hypertension or residual right-to-left shunt.
The patient was discharged home on hospital day 94. Her respiratory condition remained stable during follow-up, and no further paradoxical cerebral embolism occurred.
Discussion
This case illustrates a rare but clinically important scenario in which constrictive pericarditis leads to a right-to-left intracardiac shunt via a previously asymptomatic PFO, resulting in both paradoxical cerebral embolism and hypoxemia. The proposed mechanism, illustrated in Figure 9, likely involves elevated right atrial pressure due to impaired right ventricular filling caused by pericardial fibrosis. This elevated pressure gradient facilitates right-to-left shunting through the PFO [2,10].
Proposed mechanism of right-to-left shunting through a PFO induced by constrictive pericarditisThe schematic illustrates how fibrotic transformation of the pericardial hematoma led to compression of the right heart, resulting in elevated RA pressure. When left atrial pressure remained normal, the altered interatrial pressure gradient enabled right-to-left shunting across a previously silent PFO. This mechanism may result in paradoxical embolism, causing cryptogenic stroke, and allow venous blood to bypass the pulmonary circulation, leading to systemic hypoxemia.RA: right atrial; PFO: patent foramen ovale
Previous reports have linked acute pericarditis to hemorrhagic pericardial effusion and, when organization occurs, to constrictive physiology [15]. The risk is increased in patients receiving oral anticoagulants or with renal failure/uremic pericarditis [17]. Inflammation-related angiogenesis may also cause bleeding even without antithrombotic exposure. In our patient, although antithrombotic therapy was withheld, an organized hematoma developed and compressed the right heart, unmasking a previously silent PFO and resulting in right-to-left shunting, consistent with prior case reports [18]. These findings underscore the importance of cautious anticoagulant use and close echocardiographic follow-up in patients with pericarditis-associated effusion.
Typically, TEE with a bubble study is the gold standard for demonstrating a right-to-left shunt via the PFO [8]. This procedure was not performed preoperatively in our patient because the clinical evidence was highly suggestive of an intracardiac shunt. This evidence included findings of cardioembolic stroke, hypoxemia, and significant right heart compression on imaging [5]. Given the marked pericardial thickening and compression of the right ventricle, we suspected that constrictive pericarditis involving the right heart was contributing to the patient's hemodynamic compromise. Therefore, we decided to proceed with surgical intervention without additional invasive testing. Ultimately, a definitive diagnosis was established intraoperatively with TEE, which enabled the real-time imaging of the right-to-left shunt through the PFO [9].
Right-to-left shunting through a PFO typically occurs during transient elevations in right atrial pressure, such as those seen in pulmonary embolism or chronic obstructive pulmonary disease or during the Valsalva maneuver [5,16]. In contrast, chronic right heart compression, as seen in constrictive pericarditis, is a less common but plausible cause, as demonstrated in our case [16].
Paradoxical embolism is a potentially serious complication of PFO, especially in the presence of prothrombotic conditions [3,4]. In our patient, the delayed recognition of a PFO-mediated shunt underscores the importance of considering intracardiac shunting in cases of cryptogenic stroke when no other embolic source has been identified [5,6]. The absence of atrial fibrillation, intracardiac thrombi, and carotid artery disease further supported the diagnosis of paradoxical embolism via a PFO, which was confirmed by TEE, demonstrating a right-to-left shunt. Notably, postsurgical right heart catheterization revealed normalized intracardiac pressure and no residual shunting, confirming that the shunt was dynamic and reversible. These findings support the concept that pericardial compression can transiently elevate right atrial pressure and unmask previously silent PFO [10,16].
This case emphasizes the need to consider PFO-related right-to-left shunting in patients with unexplained hypoxemia or embolic stroke, particularly those with pericardial disease. Timely recognition and appropriate intervention, such as surgical decompression in cases similar to ours, may prevent recurrent embolic events and improve outcomes.
Conclusions
This case demonstrates that localized constrictive pericarditis can serve as a direct trigger for paradoxical embolism via a PFO. Proactive evaluation of intracardiac shunts is recommended for patients with unexplained hypoxemia or cryptogenic stroke, particularly when pericardial disease is suspected. Timely diagnosis and surgical intervention are essential for preventing recurrence and improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of patent foramen ovale in general population and in stroke patients: a narrative review Front Neurol Koutroulou I Tsivgoulis G Tsalikakis D Karacostas D Grigoriadis N Karapanayiotides T 2811120203241107410.3389/fneur.2020.00281 PMC 7198765 · doi ↗ · pubmed ↗
- 2Patent foramen ovale: a comprehensive review Curr Probl Cardiol Teshome MK Najib K Nwagbara CC Akinseye OA Ibebuogu UN 1003924520203032713110.1016/j.cpcardiol.2018.08.004 · doi ↗ · pubmed ↗
- 3Risk of paradoxical embolism (Ro PE)-estimated attributable fraction correlates with the benefit of patent foramen ovale closure: an analysis of 3 trials Stroke Kent DM Saver JL Ruthazer R 311931235120203292126210.1161/STROKEAHA.120.029350 PMC 7831886 · doi ↗ · pubmed ↗
- 4Closure of patent foramen ovale versus medical therapy in patients with cryptogenic stroke or transient ischemic attack: updated systematic review and meta-analysis Stroke Ntaios G Papavasileiou V Sagris D Makaritsis K Vemmos K Steiner T Michel P 4124184920182933533510.1161/STROKEAHA.117.020030 · doi ↗ · pubmed ↗
- 5An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke Neurology Kent DM Ruthazer R Weimar C 6196258120132386431010.1212/WNL.0b 013e 3182 a 08d 59PMC 3775694 · doi ↗ · pubmed ↗
- 6Prevalence of patent foramen ovale in the Japanese population - autopsy study Circ J Kuramoto J Kawamura A Dembo T Kimura T Fukuda K Okada Y 203820427920152608437910.1253/circj.CJ-15-0197 · doi ↗ · pubmed ↗
- 7Ridges and pouches: a case series of anomalous atrial septal fusion CASE (Phila) Zisa D Faletra FF Wessler BS Halin NJ Reddy P Patel AR Pandian NG 717420203209993710.1016/j.case.2019.10.009PMC 7026535 · doi ↗ · pubmed ↗
- 8Patent foramen ovale: the known and the to be known J Am Coll Cardiol Kutty S Sengupta PP Khandheria BK 166516715920122255459610.1016/j.jacc.2011.09.085 · doi ↗ · pubmed ↗