Eosinophilic Granulomatosis With Polyangiitis Presenting as Mononeuritis Multiplex in a Diabetic Patient: Diagnostic and Therapeutic Challenges
Waqas Ahmed, Muhammad Zeeshan Khan, Rameen Saeed, Kamran Nazir, Muhammad Farooq

TL;DR
A diabetic patient presented with EGPA as mononeuritis multiplex, highlighting the diagnostic and therapeutic challenges in distinguishing it from diabetic neuropathy.
Contribution
This case emphasizes the importance of early EGPA recognition in diabetic patients with atypical neuropathies.
Findings
The patient showed marked eosinophilia and positive MPO-ANCA, supporting EGPA diagnosis.
Multidisciplinary evaluation confirmed vasculitic neuropathy, not diabetic neuropathy.
Treatment with corticosteroids and immunosuppressants led to significant clinical improvement.
Abstract
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare antineutrophil cytoplasmic antibody (ANCA)-associated small-vessel vasculitis that may present with asthma, eosinophilia, pulmonary involvement, and peripheral neuropathy. Distinguishing EGPA-related vasculitic neuropathy from diabetic neuropathy can be particularly challenging in patients with long-standing diabetes mellitus. We present a case of a 64-year-old man with type 2 diabetes, chronic kidney disease, and asthma, who developed systemic symptoms, mononeuritis multiplex, and pulmonary haemorrhage. Laboratory tests revealed marked eosinophilia and strongly positive myeloperoxidase (MPO)-ANCA, while electrophysiological studies demonstrated asymmetric axonal neuropathy. A multidisciplinary assessment by neurology and rheumatology confirmed the diagnosis of EGPA with vasculitic neuropathy, following which treatment with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1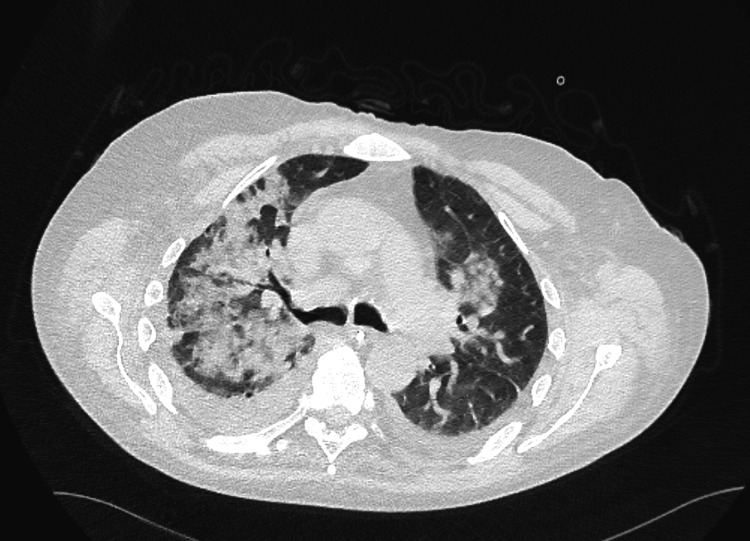 Figure 2
Figure 2| Laboratory tests | Results | Interpretation |
| White blood cell (WBC) count | 32 * 10^9/L | Leukocytosis |
| Neutrophils | Increased | Neutrophilia |
| Eosinophils | 2.08 * 10^9/L | Eosinophilia |
| C-reactive protein (CRP) | 149 mg/L | Elevated |
| MPO-ANCA | >134 U/mL | Strongly positive (supporting the diagnosis of EGPA) |
| Sputum test for tuberculosis | Negative | No TB detected |
| Interferon-gamma release assay (IGRA) | Negative | No latent TB infection |
| Sensory nerve conduction | |||||
| Nerve/sites | Onset Lat ms | Peak Lat ms | P-P Lat ms | Dist. mm | Vel m/s |
| R Median - Ulnar Hand Sensory | |||||
| Digit 2 - Wrist | 3.6 | 4.3 | 6.1 | 140 | 38.4 |
| Digit 3 - Wrist | 3.9 | 4.5 | 6.5 | 135 | 34.7 |
| Digit 5 - Wrist | NR | NR | NR | ||
| L Median - Ulnar Hand Sensory | |||||
| Digit 2 - Wrist | 2.8 | 3.4 | 6.3 | 137 | 48.7 |
| Digit 3 - Wrist | 3 | 3.4 | 4.9 | 140 | 47.3 |
| Digit 5 - Wrist | 2.3 | 2.9 | 2.5 | 112 | 48 |
| R Radial - Rec 1st Web Space, Stim Forearm | |||||
| Forearm | 2.1 | 2.7 | 17.6 | 115 | 54.1 |
| L Radial - Rec 1st Web Space, Stim Forearm | |||||
| Forearm | 2.3 | 2.7 | 29.1 | 110 | 48.9 |
| R Lateral Antebrachial Cutaneous - Rec Forearm Stim Elbow | |||||
| Elbow | 1.3 | 1.9 | 8.5 | 90 | 69.7 |
| L Lateral Antebrachial Cutaneous - Rec Forearm Stim Elbow | |||||
| Elbow | 1.5 | 2 | 15.2 | 93 | 62 |
| R Mixed Ulnar - Rec Elbow Stim Wrist | |||||
| Wrist | NR | NR | NR | ||
| L Mixed Ulnar - Rec Elbow Stim Wrist | |||||
| Wrist | NR | NR | NR | ||
| R Sural - Rec Ankle, Stim Lower Leg | |||||
| Lower Leg | NR | NR | NR | ||
| L Sural - Rec Ankle, Stim Lower Leg | |||||
| Lower Leg | NR | NR | NR | ||
| Motor nerve conduction | ||||||
| Nerve/sites | Onset ms | P-P Amp mV | Segments | Lat Diff. ms | Dist. mm | Vel m/s |
| R Median - Rec APB Stim Wrist, Elbow, Axilla | ||||||
| Wrist | NR | NR | Wrist - Elbow | NR | ||
| R Median - Rec APB Stim Wrist, Elbow, Axilla | ||||||
| Wrist | 4.5 | 4.3 | Wrist - Elbow | -6 | 275 | 45.8 |
| Elbow | 10.5 | 3.1 | Elbow - Axilla | |||
| R Ulnar - Rec ADM Stim Wrist, Elbow, Axilla | ||||||
| Wrist | 3 | 6.1 | Wrist - Below Elbow | -5.5 | 230 | 42.1 |
| Below Elbow | 8.4 | 4.3 | Below Elbow - Above Elbow | -2.1 | 116 | 54.6 |
| Above Elbow | 10.6 | 4.2 | Above Elbow - Axilla | |||
| L Median - Rec APB Stim Wrist, Elbow, Axilla | ||||||
| Wrist | 3.3 | 9.4 | Wrist - Elbow | -5.5 | 270 | 48.9 |
| Elbow | 8.8 | 8.3 | Elbow - Axilla | |||
| L Ulnar - Rec ADM Stim Wrist, Elbow, Axilla | ||||||
| Wrist | 2.8 | 7.2 | Wrist - Below Elbow | -4.6 | 230 | 50.4 |
| Below Elbow | 7.3 | 6.5 | Below Elbow - Above Elbow | -1.6 | 90 | 55.4 |
| Above Elbow | 9 | 6.2 | Above Elbow - Axilla | |||
| R Peroneal - Rec EDB, Stim Ankle, Fibula, Pop Fossa | ||||||
| Ankle | NR | NR | Ankle - Neck of Fibula | NR | ||
| L Peroneal - Rec EDB, Stim Ankle, Fibula, Pop Fossa | ||||||
| Ankle | NR | NR | Ankle - Neck of Fibula | NR | ||
| R Tibial - Rec AH, Stim Ankle, Knee | ||||||
| Ankle | NR | NR | Ankle - Knee | NR | ||
| L Tibial - Rec AH, Stim Ankle, Knee | ||||||
| Ankle | NR | NR | Ankle - Knee | NR | ||
| F-wave studies | ||
| Nerve | M Lat ms | F Lat ms |
| L Median - APB | 3.4 | 32.6 |
| L Ulnar - ADM | 2.9 | 31.8 |
| Electromyography summary | ||||||||||
| Ins. Activity | Spont. Activity | Volitional MUAPs | Maz. Volitional Act. | |||||||
| Muscle | Insertional | Fib | + Wave | Fasc | Dur. | Amp | Poly | Recruit | Pattern | Effort |
| R. Tibialis Anterior | Myotonia | 1+ | 1+ | None | Normal | Low | None | Reduced | Single Unit | Max |
| L. Tibialis Anterior | Myotonia | 1+ | 2+ | None | None | Max | ||||
| R. Gastrocnemius (Medial Head) | Myotonia | 1+ | 2+ | None | Normal | Normal | None | Reduced | Discrete | Max |
| L. Gastrocnemius (Medial Head) | Myotonia | 1+ | 1+ | None | Normal | Normal | None | Normal | Discrete | Max |
| R. Vastus Medialis | Normal | None | None | None | Long | High | None | Reduced | Discrete | Max |
| L. Vastus Medialis | Normal | None | None | None | Long | High | None | Reduced | Discrete | Max |
| R. Deltoid | Normal | None | None | None | Normal | Normal | Many | Normal | Moderate | Max |
| R. Extensor Digitorum Communis | Normal | None | None | None | Normal | Normal | None | Normal | Full | Max |
| R. First Dorsal Interosseous | Normal | None | None | None | Long | Normal | None | Reduced | Discrete | Max |
| L. First Dorsal Interosseous | Normal | None | None | None | Normal | Normal | Many | Reduced | Moderate/Discrete | Max |
| R. Iliopsoas | Normal | None | None | None | Normal | Normal | None | Normal | Full | Max |
| R. T10 Paraspinal | Normal | None | None | None | ||||||
| R. T8 Paraspinal | Increased | 1+ | 1+ | None | ||||||
| L. T8 Paraspinal | Increased | None | None | None | ||||||
| R. T7 Paraspinal | Increased | 1+ | 1+ | None | Normal | Normal | None | Normal | Full | Max |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Eosinophilic Disorders and Syndromes · Systemic Sclerosis and Related Diseases
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA), formerly Churg-Strauss syndrome, is a rare antineutrophil cytoplasmic antibody (ANCA)-associated small-vessel vasculitis that causes eosinophilic tissue infiltration and extravascular granulomas and can affect multiple organ systems, most commonly the lungs and peripheral nerves and, less frequently, the kidneys and heart [1,2]. EGPA typically progresses through three overlapping phases: a prodromal phase with asthma and allergic rhinitis, an eosinophilic phase characterized by tissue infiltration, and a vasculitic phase involving systemic small vessels [3]. Peripheral neuropathy occurs in up to 75% of patients, most commonly manifesting as painful, asymmetric mononeuritis multiplex [4]. Diagnosing EGPA in patients with diabetes mellitus presents a particular challenge. Diabetic neuropathy typically presents as a distal symmetric polyneuropathy, whereas vasculitic neuropathy is asymmetric, patchy, and may be accompanied by systemic features [5-7]. Electrophysiological studies, serologic testing (myeloperoxidase (MPO)-ANCA/perinuclear antineutrophil cytoplasmic antibodies (p-ANCA)) [6], and careful clinical evaluation are critical for accurate differentiation. Early recognition is essential to initiate immunosuppressive therapy like rituximab and prevent irreversible organ damage [8].
Case presentation
A 64-year-old man with type 2 diabetes mellitus, stage 3 chronic kidney disease, and asthma initially presented to his general practitioner with persistent fever, myalgia, and lethargy following a recent travel to South Asia. He was started on empirical antibiotics for a presumed bacterial infection, but his symptoms did not improve. Shortly afterwards, he was admitted with chest pain and treated for acute coronary syndrome. During this hospitalization, his clinical condition evolved in a way that became increasingly dominated by neurological symptoms.
While in the hospital, the patient began to develop subtle distal sensory symptoms, initially described as intermittent numbness in his left hand and foot. These symptoms rapidly progressed over days to include marked paraesthesia and weakness, particularly in the ulnar distribution of the left hand and the tibial distribution of the left lower limb. The asymmetry and rapid progression of these deficits were unusual for diabetic neuropathy, prompting further evaluation. Alongside the neurological decline, he experienced worsening fatigue, dysphagia, and unintentional weight loss. A gastroscopy was performed to evaluate for eosinophilic oesophagitis in the context of marked eosinophilia, but the findings were unremarkable.
His systemic symptoms worsened with the onset of acute dyspnoea and haemoptysis, necessitating high-flow oxygen support. Imaging studies, including chest radiography (Figure 1) and subsequent computed tomography (Figure 2), revealed bilateral pulmonary haemorrhages, predominantly affecting the right lung, suggestive of an underlying vasculitic process. Differential diagnoses, including tuberculosis, were considered but subsequently excluded based on negative sputum analysis and interferon-gamma release assay (IGRA) results.
Chest radiograph demonstrating bilateral pulmonary opacities consistent with pulmonary haemorrhage, more pronounced in the right side.This image shows diffuse patchy opacities, greatest in the right mid-to-lower zones, consistent with vasculitic pulmonary involvement in eosinophilic granulomatosis with polyangiitis.
Computed tomography of the chest showing bilateral pulmonary haemorrhages, more pronounced in the right lung.Bilateral high-attenuation ground-glass and patchy consolidation, more pronounced on the right, suggest acute alveolar haemorrhage from a vasculitic process.
Laboratory investigations, as summarized in Table 1, revealed marked leukocytosis (WBC = 32 × 10⁹/L) with neutrophilia and eosinophilia (2.08 × 10⁹/L), along with an elevated C-reactive protein level (149 mg/L). MPO-ANCA was strongly positive (>134 U/mL), supporting the diagnosis of EGPA.
As described above, the patient’s evolving neurological deficits, including asymmetric numbness and weakness, prompted further evaluation with electrophysiological studies. Nerve conduction studies (Tables 2-4) and electromyography (Table 5) were performed to characterize the pattern and extent of neuropathy. These investigations revealed asymmetric sensory and motor involvement consistent with mononeuritis multiplex. Specifically, there was impaired motor and sensory conduction in the right median and ulnar nerves, absent sural sensory responses bilaterally, and markedly reduced ulnar sensory responses with relative preservation of radial and lateral antebrachial cutaneous nerves. Motor studies demonstrated reduced compound muscle action potentials in intrinsic hand and foot muscles and slowed conduction in the right ulnar nerve.
Electromyography (EMG) demonstrated fibrillation potentials and positive sharp waves in the tibialis anterior, medial gastrocnemius, and thoracic paraspinal muscles, chronic reinnervation changes in the vastus medialis and first dorsal interosseous muscles, and fibrosis in the medial gastrocnemius. Overall, the findings indicate an asymmetric, predominantly axonal, inflammatory neuropathy with both chronic and active denervation, consistent with mononeuritis multiplex.
A multidisciplinary discussion between neurology and rheumatology teams confirmed vasculitic mononeuritis multiplex secondary to EGPA. The patient was treated with high-dose intravenous corticosteroids, pulsed methylprednisolone, and cyclophosphamide. He later developed sepsis, requiring intensive care support, including plasmapheresis, intravenous immunoglobulin, and mechanical ventilation.
Following stabilization, rituximab therapy was initiated. Over the following weeks, the patient showed marked improvement in systemic symptoms and neurological function, with gradual recovery of motor and sensory deficits.
Discussion
This case underscores the diagnostic and therapeutic complexity of EGPA in a patient with pre-existing diabetes mellitus. While neuropathy is a common complication of diabetes, the presence of asymmetric or patchy deficits, particularly when accompanied by systemic inflammation, eosinophilia, or pulmonary involvement, should prompt consideration of a vasculitic aetiology such as EGPA [5-7]. Unlike diabetic polyneuropathy, which typically presents as a symmetric, distal sensorimotor neuropathy without systemic manifestations, vasculitic neuropathy often demonstrates asymmetry, rapid progression, and nerve-specific involvement, as observed in this patient [5].
Electrophysiological studies and serological testing, particularly MPO-ANCA, were pivotal in distinguishing EGPA-associated neuropathy from diabetic neuropathy [3,4,6]. In this patient, nerve conduction studies revealed asymmetric axonal involvement, with selective impairment of the ulnar, median, and tibial nerves, while other sensory nerves, such as the radial and lateral antebrachial cutaneous nerves, were relatively preserved. This pattern, coupled with EMG evidence of fibrillation potentials, positive sharp waves, and chronic reinnervation, indicated ongoing inflammatory damage and differentiated the neuropathy from the diffuse, length-dependent axonal loss typically seen in diabetes [4]. The strongly positive MPO-ANCA and marked eosinophilia further supported a systemic vasculitic process rather than metabolic neuropathy alone.
The patient’s clinical course also highlights the potential severity of EGPA, exemplified by pulmonary haemorrhage and sepsis requiring intensive care management [9]. The favourable response to immunosuppressive therapy, including corticosteroids, cyclophosphamide, and rituximab, demonstrates the critical importance of early recognition and aggressive intervention to prevent permanent neurological deficits and multi-organ complications [8,9].
Overall, this report contributes to the literature by reinforcing the need for vigilance in diabetic patients presenting with atypical, asymmetric neuropathies, especially when accompanied by systemic or inflammatory features [5,10]. The synthesis of electrophysiological findings with serological and clinical data illustrates how careful interpretation beyond descriptive reporting can guide early, targeted therapy, ultimately reducing morbidity and preventing irreversible organ damage [9].
Conclusions
EGPA should be actively considered in diabetic patients who develop unexplained systemic symptoms and asymmetric neuropathy. Differentiating vasculitic neuropathy from diabetic neuropathy requires thorough clinical evaluation, electrophysiological studies, and serological testing for ANCA and eosinophil counts.
Prompt recognition and initiation of immunosuppressive therapy, supported by a multidisciplinary care approach, are crucial to prevent permanent neurological deficits and organ damage. This case highlights the importance of maintaining a high index of suspicion for EGPA in complex diabetic presentations to ensure timely diagnosis and improved patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eosinophilic granulomatosis with polyangiitis - advances in pathogenesis, diagnosis, and treatment Front Med (Lausanne) Fijolek J Radzikowska E 11452571020233721572010.3389/fmed.2023.1145257 PMC 10193253 · doi ↗ · pubmed ↗
- 2Eosinophilic granulomatosis with polyangiitis: an overview Front Immunol Gioffredi A Maritati F Oliva E Buzio C 549520142540493010.3389/fimmu.2014.00549 PMC 4217511 · doi ↗ · pubmed ↗
- 3Eosinophilic granulomatosis with polyangiitis: understanding the disease and its management Rheumatology (Oxford) Trivioli G Terrier B Vaglio A 09459202010.1093/rheumatology/kez 57032348510 · doi ↗ · pubmed ↗
- 4Clinical characteristics and treatment response of peripheral neuropathy in the presence of eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome): experience at a single tertiary center J Clin Neurol Cho HJ Yune S Seok JM 77831320172807931610.3988/jcn.2017.13.1.77PMC 5242145 · doi ↗ · pubmed ↗
- 5Eosinophilic granulomatosis with polyangiitis (EGPA)- a presentation of rapid progressive demyelinating polyneuropathy Open J Clin Med Case Rep Kheng QK 135032017 https://jclinmedcasereports.com/articles/OJCMCR-1350.pdf
- 6Severe mononeuritis multiplex in a patient with eosinophilic granulomatosis with polyangiitis Reumatologia Kalinova D Kukushev G Kolarov Z Rashkov R 2882915720193184434210.5114/reum.2019.89522 PMC 6911252 · doi ↗ · pubmed ↗
- 7Unique case of mononeuritis multiplex in a patient of Eosinophilic granulomatosis with polyangiitis J Family Med Prim Care Shah T Patel P Patel M 301330151420254081451310.4103/jfmpc.jfmpc_1870_24PMC 12349800 · doi ↗ · pubmed ↗
- 8Rituximab for eosinophilic granulomatosis with polyangiitis with severe vasculitic neuropathy: case report and review of current clinical evidence Semin Arthritis Rheum Fanouriakis A Kougkas N Vassilopoulos D Fragouli E Repa A Sidiropoulos P 60664520152590817910.1016/j.semarthrit.2015.03.004 · doi ↗ · pubmed ↗