A Quasi-experimental Study to Assess the Effectiveness of the Neonatal Golden Hour Management Workshop on Knowledge Among Healthcare Providers in Latifa Women and Children Hospital, Dubai
Khaled El-Atawi, Merlin N Kumari, Khadija M AL Sulaimi, Udayakumari Pethaperumal, Sylvia Fernandes

TL;DR
This study shows that a workshop on neonatal care significantly improved healthcare providers' knowledge during the critical first hour of a newborn's life.
Contribution
The study demonstrates the effectiveness of a structured neonatal golden hour workshop in improving healthcare providers' knowledge.
Findings
Post-workshop knowledge scores showed significant improvement compared to pretest results.
Healthcare providers in ICU and emergency departments had higher knowledge scores after the workshop.
Older participants (35-50 years) achieved higher knowledge scores following the training.
Abstract
Background: The first hour of life, often referred to as the "golden hour," represents a critical window for initiating timely, evidence-based interventions that stabilize the newborn and reduce the risk of complications. This period demands coordinated efforts in thermoregulation, respiratory support, glucose monitoring, and early nutrition to optimize neonatal outcomes. Despite the existence of well-established clinical guidelines, knowledge and practice gaps among healthcare providers continue to pose significant challenges. These discrepancies contribute to variations in the quality of neonatal care, particularly in high-risk settings. To address this issue, structured educational programs and targeted workshops have emerged as effective strategies to enhance healthcare providers' competencies, ensuring consistent and high-quality care during this vital phase. Objective: This study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
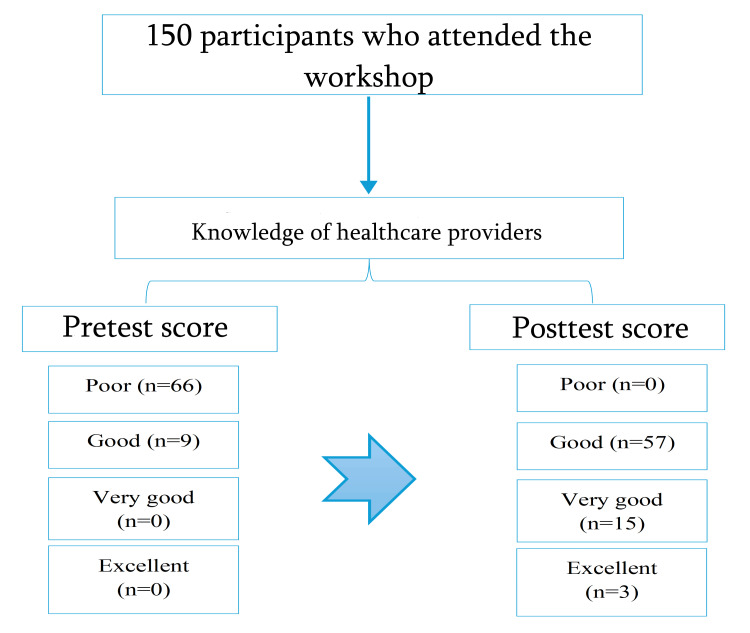 Figure 1
Figure 1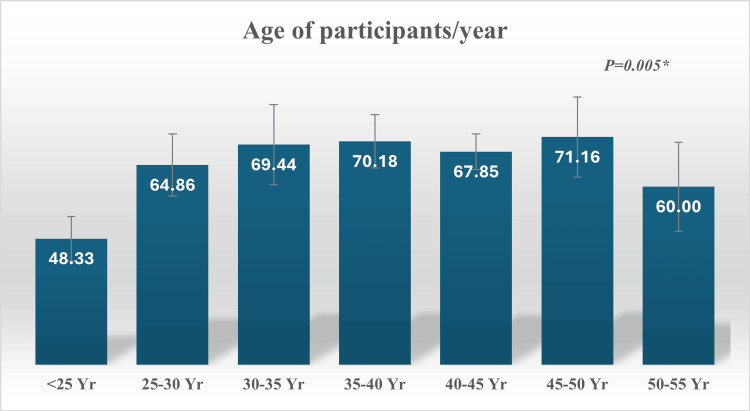 Figure 2
Figure 2| Score interpretation | Pretest score (N=75) | Posttest score (N=75) | Total (N=150) | χ2 | MC (P) |
| Poor (<70%) | 66 (88) | 0 | 66 (44) | 94.573 | <0.001* |
| Good (70-80%) | 9 (12) | 57 (76) | 66 (44) | ||
| Very good (80-90%) | 0 | 15 (20) | 15 (10) | ||
| Excellent (90-100%) | 0 | 3 (4) | 3 (2) | ||
| Total | 75 | 75 | 150 | - | - |
| Healthcare providers' knowledge scores | Mean±SD | χ2 | P | ||||
| Poor (<70%) | Good (70-80%) | Very good (80-90%) | Excellent (90-100%) | ||||
| Maternity | 24 (36.36) | 14 (21.2) | 5 (33.3) | 3 (100) | 65.97±17.18 | 1.396 | 0.926 |
| Operation theatre | 3 (4.5) | 2 (3.03) | 0 | 0 | 60.00±20.31 | ||
| Delivery suite | 12 (18.2) | 15 (22.7) | 2 (13.3) | 0 | 68.27±11.04 | ||
| NICU | 23 (34.8) | 22 (33.3) | 6 (40) | 0 | 63.82±18.01 | ||
| ICU | 2 (3.03) | 8 (12.1) | 2 (13.3) | 0 | 74.58±8.10 | ||
| Emergency | 2 (3.03) | 5 (7.6) | 0 | 0 | 70.71±8.86 | ||
| Total | 66 | 66 | 15 | 3 | 66.40±15.83 | - | - |
| Healthcare providers' knowledge scores | Mean±SD | χ2 | P | ||||
| Poor (<70%) | Good (70-80%) | Very good (80-90%) | Excellent (90-100%) | ||||
| <5 years | 5 (7.6) | 6 (9.1) | 3 (20) | 1 (33.3) | 67.33±21.62 | 14.657 | 0.014* |
| 5-10 years | 14 (21.1) | 7 (10.6) | 3 (20) | 1 (33.3) | 62.60±19.21 | ||
| 10-15 years | 23 (34.8) | 19 (28.8) | 4 (26.7) | 1 (33.3) | 65.21±15.88 | ||
| 15-20 years | 13 (19.7) | 25 (37.9) | 4 (26.7) | 0 | 70.24±11.89 | ||
| 20-25 years | 6 (9.1) | 7 (10.6) | 1 (6.7) | 0 | 67.86±11.55 | ||
| >25 years | 5 (7.6) | 2 (3) | 0 | 0 | 60.00±15.55 | ||
| Total | 66 | 66 | 15 | 3 | 66.40±15.83 | - | - |
| Healthcare providers' knowledge scores | Mean±SD | χ2 | P | ||||
| Poor (<70%) | Good (70-80%) | Very good (80-90%) | Excellent (90-100%) | ||||
| Bachelor | 63 (95.5) | 65 (98.5) | 15 (100) | 3 (100) | 66.54±15.92 | 2.107 | 0.910 |
| Diploma | 1 (1.5) | 0 | 0 | 0 | 60.00±0.000 | ||
| Master | 2 (3.03) | 1 (1.5) | 0 | 0 | 61.67±16.07 | ||
| Total | 66 | 66 | 15 | 3 | 66.40±15.83 | - | - |
| Healthcare providers' knowledge scores | Mean±SD | χ2 | P | ||||
| Poor (<70%) | Good (70-80%) | Very good (80-90%) | Excellent (90-100%) | ||||
| No | 61 (92.4) | 9 (13.6) | 0 | 0 | 53.36±12.59 | 11.85 | <0.001* |
| Yes | 5 (7.6) | 41 (62.1) | 11 (73.3) | 3 (100) | 77.58±8.00 | ||
| Golden hour workshop | 0 | 2 (3.03) | 0 | 0 | 75.00±0.00 | ||
| Neonatal nursing course | 0 | 3 (4.5) | 1 (6.7) | 0 | 78.75±4.79 | ||
| Stable | 0 | 7 (10.6) | 0 | 0 | 76.43±2.44 | ||
| Others related to the neonatal specialty | 0 | 4 (6.06) | 3 (20) | 0 | 83.00±2.74 | ||
| Total | 66 | 66 | 15 | 3 | 66.40±15.83 | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Hospital Admissions and Outcomes · Infant Development and Preterm Care
Introduction
Clinical events that occur during the physiologic transition from intrauterine to extrauterine life are especially significant for the extremely low birth weight (ELBW) infant (≤1000 g) [1]. Following birth, ELBW infants are susceptible to the rapid development of hypothermia, hypoglycemia, hypotension, and respiratory failure [2,3]. Resuscitation in the delivery room (DR) and stabilization during admission to the neonatal intensive care unit (NICU) involve a series of interdependent tasks and procedures. These interventions must be performed quickly, proficiently, and systematically to minimize the short-term sequelae of prematurity, which contribute to the risk of long-term morbidity and mortality [4].
Neonatal morbidity and death are permanently impacted by care practices during the first 60 minutes of life for extremely preterm neonates [5,6]. The phrase "golden hour" refers to the crucial hour following an initial injury during which successful stabilization increases survival. It originated from the out-of-hospital stabilization of adult trauma patients. The first hour of newborn care following delivery has recently been referred to by this phrase [7]. The golden hour refers to a potentially standardized, evidence-based approach to DR care, communication, and teamwork for very preterm infants (less than 32 weeks' gestational age (GA)), with the goal of improving outcomes. However, the precise procedures included or recommended within the neonatal golden hour are currently unclear [8]. Maintaining normothermia, targeting oxygen saturation appropriately, using non-invasive respiratory support on a regular basis, and preventing hypoglycemia are among the goals. There are no precise criteria for the timing of interventions within the first hour of life, despite the fact that international resuscitation guidelines concentrate on standardized DR stabilization [9].
Critical to the success and sustainability of any golden hour initiative is the recognition of the continuous educational process involving multidisciplinary team collaboration to ensure coordination between providers in the DR and beyond [10]. Standardization of practices in the care of extremely premature neonates during the first hour of life leads to improved outcomes. A coordinated focus on the golden hour in ELBW neonates has been shown to improve short-term and long-term outcomes [11].
Simulation-based learning (SBL) has been shown to effectively improve medical knowledge, procedural proficiency, comfort with undertaking taught tasks, inter-professional communication, teamwork, and teaching skills [12,13]. This study aimed to find the effectiveness of the neonatal golden hour management workshop on knowledge among nurses in the selected government hospital. Thus, nurses who attended the workshop will gain enough knowledge and confidence to face the real situation and act appropriately to save the patient at the earliest by implementing learned advanced interventions.
Research hypothesis
H1
There is a significant difference in pre- and posttest knowledge scores of healthcare providers who attended the golden hour management workshop.
H0
There is no significant difference in pre- and posttest knowledge scores of healthcare providers who attended the golden hour management workshop.
H1
There is a significant association between the selected demographic variables and knowledge scores of healthcare providers who attended the golden hour management workshop.
H0
There is no significant association between the selected demographic variables and knowledge scores of healthcare providers who attended the golden hour management workshop.
Materials and methods
Study design and setting
A quasi-experimental quantitative research design study was conducted at Latifa Women and Children Hospital, one of the largest maternity hospitals in Dubai, consisting of all its employees. The hospital has around 600 nurses working in various maternity units and a yearly census of 4000-5000 deliveries, and all normal vaginal deliveries are conducted by obstetric nurses or midwives. All categories of nurses working who attended the workshop from February 2024 to November 2024 were included as sample.
Sample size and selection
Sampling is the process of selecting a portion of the population to represent the entire population. Purposive sampling techniques were used to select the sample. One hundred fifty samples were included in the study.
Sample selection criteria
In the current study, we included the nurses who attended the golden hour workshop and were willing to participate. However, we excluded the nurses who attended the golden hour workshop before the study period.
Collection of data
A structured questionnaire was prepared based on the 10 components of the golden hour [14,15], namely, antenatal counseling and team pre-briefing, delayed cord clamping, support to the respiratory system, support to the cardiovascular system, prevention of hypoglycemia-initiation of breastfeeding, infection prevention/laboratory investigation/arterial blood gas (ABG) analysis, temperature control, monitoring/record-code narrator documentation, teamwork/de-briefing/communication and family counseling, and emotional support. From each component, two questions are being prepared and sent for expert validity, and data were collected by sending an online questionnaire to the study participants.
A structured questionnaire was prepared based on the components of golden hour [14,15].
Validity of the tool
To determine the content validity of the data collection tool, the prepared instrument along with the proposal was sent to five experts. The experts were requested to give their opinion on the appropriateness and relevance of standardized tools. Modifications were made according to the experts' opinion.
Ethical considerations
Ethical permission was obtained from the Dubai Scientific Research Ethics Committee (DSREC) of the Dubai Health Authority (approval number: DSREC-11/2024_37). The study was conducted after obtaining written informed consent from all the participants. Assurance was given to all the participants that confidentiality will be maintained throughout the study.
Pilot study
A pilot study is a test run of the research to confirm its feasibility and conduct the real study based on the test run changes. A pilot study was conducted among 10 samples who met the inclusion criteria.
Data collection
The purpose and significance of the study were communicated to the participants in advance, and the staff who came to the workshop were given a pretest and posttest to assess their knowledge. The study subjects were allowed to withdraw consent at any time. The researchers remained neutral in collecting the data by sending the questionnaire via Microsoft Forms (Microsoft Corp., Redmond, WA, USA) to the study participants.
Data analysis methods
Data was analyzed based on descriptive and inferential statistics. Statistical analysis was done using IBM SPSS Statistics for Windows, V. 26.0 (IBM Corp., Armonk, NY, USA). Quantitative variables were presented as mean and standard deviation (SD) and were analyzed by an unpaired Student's t-test. Qualitative variables were presented as frequency and percentage (%) and were compared by the chi-squared test. Fisher's exact test or Monte Carlo correction was used to correct for chi-square when more than 20% of the cells have expected count less than 5. The analysis of variance (ANOVA) F-test is used to compare the quantitative variables between more than two groups of normally distributed data. The paired t-test is used to test the mean difference between pairs of measurements. A p-value of <0.001 was considered statistically highly significant.
Results
A flowchart illustrates that there were 150 participants who attended the workshop and their knowledge was assessed using a pretest and posttest at Latifa Women and Children Hospital, one of the largest maternity hospitals in Dubai (Figure 1). Participants were categorized into four groups based on their pretest and posttest scores: 66 (44%) demonstrated poor knowledge, 57 (44%) had good knowledge, 15 (10%) had very good knowledge, and 3 (2%) had excellent knowledge.
Flowchart of the participants studied.
The findings of the study revealed a highly significant improvement in participants' knowledge following the golden hour management workshop, as indicated by the posttest scores (p<0.001). Post-intervention, 76% of participants achieved good knowledge, 20% demonstrated very good knowledge, and 4% reached excellent knowledge levels compared to only 12%, 0%, and 0%, respectively, in the pretest (Table 1, Figure 1).
In the current study, a significant association was observed between participants' knowledge scores and their age (p=0.005). Participants aged 40-50 years and 35-40 years demonstrated higher knowledge scores (71.16±25.16 and 70.18±9.95, respectively). Conversely, participants younger than 25 years recorded the lowest knowledge scores (48.33±21.50) (Figure 2).
Relation between healthcare providers' knowledge scores and ages.
With respect to different units, participants working in the intensive care unit (ICU) and emergency department demonstrated the highest knowledge scores (74.58±8.10 and 70.71±8.86, respectively), followed by those in the delivery suite (68.27±11.04). In contrast, participants from the operation theatre reported the lowest knowledge scores (60.00±20.31). However, no statistically significant relationship was found between knowledge scores across the various departments, including maternity, operation theatre, delivery suite, NICU, ICU, and emergency (p>0.05) (Table 2).
Similarly, no significant association was observed between participants' knowledge scores and years of experience (p>0.05) (Table 3).
Additionally, healthcare providers' knowledge scores increased among participants who had a bachelor's education (66.54±15.92); however, there was no significant relation between healthcare providers' knowledge scores and highest education (p>0.05) (Table 4).
In contrast, there was a highly significant relation between healthcare providers' knowledge scores and courses attended previously (p>0.001). The participants who previously attended neonatal nursing courses and other courses related to the neonatal specialty had higher scores (78.75±4.79 and 83.00±2.74) (Table 5).
Discussion
The neonatal period represents a highly vulnerable stage, with the first 60 minutes after birth often referred to as the "golden hour" being particularly critical for both survival and long-term health outcomes [16]. Evidence-based interventions during this period, including thermoregulation, respiratory support, vascular access, and timely administration of medications, have consistently demonstrated improvements in both short-term outcomes (such as reduced hypothermia and hypoglycemia) and long-term outcomes (including lower risks of bronchopulmonary dysplasia, intraventricular hemorrhage, and retinopathy of prematurity), especially among extremely premature and ELBW infants [11]. Hence, this study aimed to assess the effectiveness of neonatal golden hour management on the knowledge scores of healthcare providers before and after attending the workshop.
In our study, 76%, 20%, and 4% of participants demonstrated good, very good, and excellent healthcare knowledge regarding golden hour management, as measured by posttest scores. These findings are consistent with those of Moninder and Gopal [17], who assessed the effectiveness of a structured teaching program on the management of neonatal asphyxia among staff nurses in pediatric allied units in selected hospitals of Punjab. Their study revealed that, in the pretest, 22 (73.34%) staff nurses in the experimental group had average knowledge and eight (26.66%) had below-average knowledge. In the control group, 20 (66.67%) had average knowledge, eight (26.66%) had below-average knowledge, and only two (6.67%) demonstrated good knowledge, with no staff nurse in either group achieving excellent knowledge. Following the intervention, however, the experimental group showed notable improvement, with 80% of nurses attaining good knowledge, 13.33% achieving excellent knowledge, and 6.67% remaining at an average level. Conversely, the control group continued to exhibit lower outcomes, with 76.67% at average knowledge and 23.33% at below-average knowledge. The consistency between their results and the current study highlights that structured educational interventions are effective in enhancing knowledge among healthcare workers involved in neonatal care.
The comparison between their findings and this study underscores the effectiveness of structured educational interventions in enhancing knowledge among healthcare professionals involved in neonatal care. Similar results were observed by Bajracharya et al. [18] in a quasi-experimental study assessing the effect of educational interventions on neonatal resuscitation knowledge and skills among nursing students. That study reported a significant increase in median knowledge and skill scores post-intervention. Notably, while the intervention and control groups did not differ significantly before the training, a statistically significant difference emerged after the intervention, highlighting the substantial impact of structured training programs on competency development.
Our outcome reflects a high level of post-intervention knowledge compared with previous studies conducted in similar contexts. For instance, Kamath-Rayne et al. [19] reported a lower mean pretest knowledge score of 7.22 among Indian nurses prior to neonatal resuscitation training, while Kc et al. [20] found similarly low pretest scores in Nepal before participants received a three-day neonatal resuscitation course. These findings suggest that baseline knowledge among healthcare workers often remains limited before structured educational programs are introduced. Consistent with the present study, research in Ethiopia by Hoban et al. [21] demonstrated a substantial improvement in healthcare workers' neonatal resuscitation knowledge immediately after training, effectively closing the pre-existing knowledge gap. Likewise, Sendo et al. [22] on Ethiopian undergraduate midwifery students reported a significant rise in posttest knowledge scores among participants following the Helping Babies Breathe intervention, with all participants attaining adequate knowledge levels (p<0.001). The convergence of findings across these studies supports the conclusion that targeted, skill-based educational programs are highly effective in enhancing neonatal care knowledge. However, variations in knowledge levels across studies may be attributed to differences in course duration, content specificity, and participants' prior clinical exposure. Collectively, the evidence underscores the value of structured training interventions in improving healthcare providers' competency in critical neonatal care, particularly during the golden hour and resuscitation period.
Although the general trend across all three studies confirms the effectiveness of educational interventions in neonatal care, differences emerge in the degree of improvement achieved. The current study showed a complete elimination of poor knowledge levels in the posttest, while in Moninder and Gopal's research, some participants in the control group continued to have below-average knowledge even after the teaching program [17]. This may be explained by the difference in methodology, as the present study used a workshop-based training model that provided hands-on engagement, whereas Moninder and Gopal utilized a structured teaching program that may have been more theoretical [17]. Furthermore, differences in the study populations could also contribute to variations in outcomes. The present study focused on healthcare providers at Latifa Women and Children Hospital, Dubai, while Moninder and Gopal assessed staff nurses in pediatric allied units in Punjab, and Bajracharya et al. evaluated nursing students [17,18]. These groups vary in terms of clinical exposure, prior knowledge, and direct responsibility for neonatal care, which may influence how effectively they benefit from educational interventions. Despite these variations, the overall agreement among the studies strongly supports that structured teaching, workshops, and training interventions significantly enhance knowledge and skills in neonatal care, though tailoring the method to the characteristics of the target population may optimize the outcomes.
The present study showed that there was no significant relation between healthcare providers' knowledge scores and years of experience, and, similarly, no significant relation between healthcare providers' knowledge scores and highest educational level, even though most of the nurses in the study sample held a bachelor's degree. The current results stand in contrast to the earlier work of Maarouf [23]. In an assessment of nurses' performance for traumatic head injury patients during the golden hour, Maarouf found that a high proportion (nearly two-thirds) of nurses had unsatisfactory practices. Furthermore, that study identified a statistically significant relationship between practice levels and years of experience, as well as a highly significant relationship with nurse age. According to Maarouf, increasing age and years of experience contributed to performance improvements until the level of automatism was reached [23]. This view was supported by Delucia et al. [24] and Dale et al. [25], who confirmed that work experience influences nurses' performance. On the other hand, Collins [26] reported that total nurses' practice regarding nursing management of trauma patients in the emergency unit was satisfactory, while Browne and Merrill [27] clarified that most studied nurses demonstrated satisfactory practice regarding the assessment and management of severe musculoskeletal injury. Furthermore, the results of the current study are not in line with Gidam and Abdelgair [28], who found that years of experience strongly affected performance, with more than half of the respondents having less than one year of experience. Their results align with previous research indicating a positive association between healthcare providers' years of experience and their neonatal resuscitation performance [29-31]. The discrepancy between these studies and the present findings may be explained by methodological differences, as the current study measured knowledge while others primarily assessed practice. It may also be related to contextual factors. In the present study, most nurses were bachelor's degree holders working in a tertiary hospital in Dubai, while Maarouf [23] and Elsayed [32] studied nurses in Ain Shams University Hospitals, Collins [26] evaluated emergency nurses, and Gidam and Abdelgair [28] focused on nurses and midwives in Sudan. Regarding education, the present study differs from Elsayed [32] and Ahmed et al. [33] who both found that most nurses in Ain Shams University were diploma graduates. However, the current results are in partial agreement with Maarouf [23], who found that nearly half of the emergency nurses in her study held a bachelor’s degree. Additionally, Ahmed et al. [33] reported that nearly three-quarters of their sample studied had received a training course about trauma patients, with more than four-fifths of them gaining benefits, which agrees with Metwaly et al. [34], who found that more than half of the nurses in their study at Zagazig University had training courses about critically ill patients. Overall, these comparisons suggest that while structured training programs consistently improve performance and knowledge, the impact of years of experience and educational level is less uniform and may depend on the setting, the characteristics of the studied population, and whether outcomes are measured as knowledge or practice.
Participants who had previously attended neonatal nursing courses and other courses related to the neonatal specialty achieved significantly higher knowledge scores, indicating a strong correlation between prior training and knowledge levels. These results emphasize the direct impact of prior training on improving knowledge in neonatal care. Similar findings were reported by Gidam and Abdelgair [28] who found that 53.3% of respondents had received training, while 46.7% had not, despite receiving basic neonatal cardiopulmonary resuscitation, and their results indicated that training had a direct effect on performance with respect to basic neonatal cardiopulmonary resuscitation. Furthermore, they noted that post‐educational program knowledge of respondents regarding advanced newborn cardiopulmonary resuscitation reached 65.3% compared to the pre‐educational program, which reflected high motivation to acquire knowledge after training. However, contradictory evidence was found in studies from Baghdad and Nigeria, where no statistically significant association was observed between nurses' practices and their number of training sessions (Nour [35] and Khalid et al. [36]), suggesting that the effectiveness of training may also depend on its structure, quality, and follow-up mechanisms. In a similar vein, Bajracharya et al. [18] in a quasi-experimental study on the effect of educational intervention on neonatal resuscitation knowledge and skills among nursing students found that training provided essential knowledge and skills, enabling students to handle neonatal emergencies more effectively. Their study showed that while the median pretest knowledge scores of the intervention and control groups were not significantly different, the posttest scores became significantly different (p<0.001). The median knowledge score in the intervention group increased markedly from 30.0 to 49.0, while that of the control group only increased slightly from 29.0 to 31.5. A significant increase was noted in both groups, but the difference was larger in the intervention group (19.0) compared to the control group (2.5). Bajracharya et al. suggested that the increase in the control group's posttest knowledge could have been due to sensitization, as the initial pretest assessment may have motivated them to study neonatal resuscitation independently [18]. Their findings align with those of Pawase [37], Guleri [38], and Sarvan and Efe [39], who all demonstrated increased knowledge after educational interventions, but differ from Kumar and Patidar [40] who observed a significant rise in the intervention group only, with no corresponding improvement in the control group. Beyond knowledge, Bajracharya et al. [18] also demonstrated that educational interventions improved skills, without a significant difference, but median posttest scores showed a highly significant difference (p<0.001). This result is supported by Sarvan and Efe [39] who similarly reported a difference in favor of the intervention group in enhancing skills.
Similarly, the study conducted by Mohamed and Alatroshi [41] reported a substantial improvement in nurses' knowledge following an educational intervention on neonatal sepsis. Their quasi-experimental study showed that participants in the experimental group achieved markedly higher posttest scores compared to pretest results, indicating the effectiveness of targeted educational programs in improving clinical knowledge. Both studies, therefore, agree that structured and focused educational interventions play a crucial role in enhancing healthcare providers' competence in neonatal care. However, while the study by Mohamed and Alatroshi concentrated on neonatal sepsis management, the current research emphasized comprehensive golden hour management, which involves a broader scope of neonatal stabilization practices [41]. The difference in focus may explain variations in the specific domains of knowledge gained. Moreover, the consistent improvement across both studies supports the premise that continuous professional development and participation in specialized workshops are essential for maintaining and advancing clinical proficiency among neonatal healthcare providers.
Finally, taken together, the findings of the present study and previous research strongly affirm that participation in training and courses has a powerful influence on improving both knowledge and skills in neonatal care, with consistent evidence across diverse contexts including Dubai, Sudan, South Asia, and Africa. At the same time, the variability observed in some studies may be explained by differences in training design, follow-up evaluation, and participant motivation, highlighting the need for structured, interactive, and contextually adapted educational programs to optimize outcomes.
Conclusions
Results of the current study concluded that there is a highly significant improvement in healthcare knowledge regarding golden hour management when comparing the participants' posttest scores vs their pretest scores. This result highlights the crucial role of structured workshops and training courses in improving the preparedness of healthcare providers to deliver timely and effective neonatal care during the golden hour. These findings support the integration of regular, evidence-based educational interventions into hospital training policies to ensure sustained improvements in neonatal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Outcomes of a neonatal golden hour implementation project Am J Med Qual Ashmeade TL Haubner L Collins S Miladinovic B Fugate K 73803120162519400210.1177/1062860614548888 · doi ↗ · pubmed ↗
- 2Golden hour protocol for preterm infants: a quality improvement project Adv Neonatal Care Harriman TL Carter B Dail RB Stowell KE Zukowsky K 4624701820183021238910.1097/ANC.0000000000000554 · doi ↗ · pubmed ↗
- 3"Golden hour" quality improvement intervention and short-term outcome among preterm infants J Perinatol Peleg B Globus O Granot M 3873923920193034140310.1038/s 41372-018-0254-0 · doi ↗ · pubmed ↗
- 4The golden hour: a quality improvement initiative for extremely premature infants in the neonatal intensive care unit J Perinatol Croop SE Thoyre SM Aliaga S Mc Caffrey MJ Peter-Wohl S 5305394020203171265910.1038/s 41372-019-0545-0PMC 7222905 · doi ↗ · pubmed ↗
- 5Admission temperature and associated mortality and morbidity among moderately and extremely preterm infants J Pediatr Laptook AR Bell EF Shankaran S 535919220182924635810.1016/j.jpeds.2017.09.021PMC 5808888 · doi ↗ · pubmed ↗
- 6Admission temperature and hospital outcomes in extremely preterm infants J Paediatr Child Health Tay VY Bolisetty S Bajuk B Lui K Smyth J 2162235520193021846510.1111/jpc.14187 · doi ↗ · pubmed ↗
- 7The golden hour in trauma: dogma or medical folklore?Injury Rogers FB Rittenhouse KJ Gross BW 5255274620152526232910.1016/j.injury.2014.08.043 · doi ↗ · pubmed ↗
- 8Quality improvement in the golden hour for premature infants: a scoping review BMC Pediatr Sheng L Zhong G Xing R Yan X Cui H Yu Z 882420243830296010.1186/s 12887-024-04558-9PMC 10832117 · doi ↗ · pubmed ↗