When the Eyes Deceive: Uncommon Ophthalmic Presentation of Giant Cell Arteritis
Tony Yap, Leena Yalakki-Jagadeesh, Alison Penwarden, Khushbakht Subhani

TL;DR
A rare case of giant cell arteritis presented with unusual eye symptoms and was managed with steroids.
Contribution
This case highlights the importance of early steroid treatment and careful tapering in managing GCA.
Findings
A patient with GCA presented with isolated cranial nerve IV palsy and hypertension.
Steroids resolved symptoms quickly, emphasizing the need for prompt treatment.
Stopping steroids led to symptom recurrence, underscoring the need for gradual tapering.
Abstract
Giant cell arteritis (GCA) is a systemic granulomatous large vessel vasculitis that predominantly affects older adults. We present a rare case of a patient in her 60s who presented with hypertension and isolated cranial nerve (CN) IV palsy. Initial imaging and temporal artery biopsy performed were negative. Her symptoms then resurfaced again after her prednisolone was stopped. Re-commencement of steroids led to a quick resolution of her visual symptoms and headaches within a matter of days. This case highlights the importance of clinical judgement and prompt initiation of steroids without delay. A gradual and prolonged steroid tapering regime is also essential to avoid visual loss, the most feared complication in GCA.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
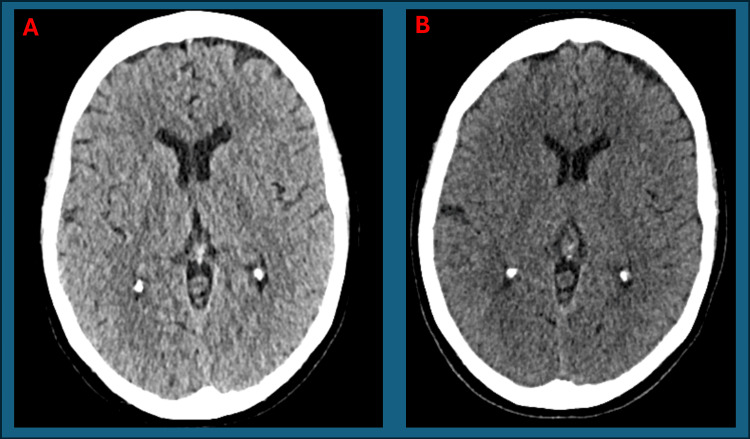 Figure 1
Figure 1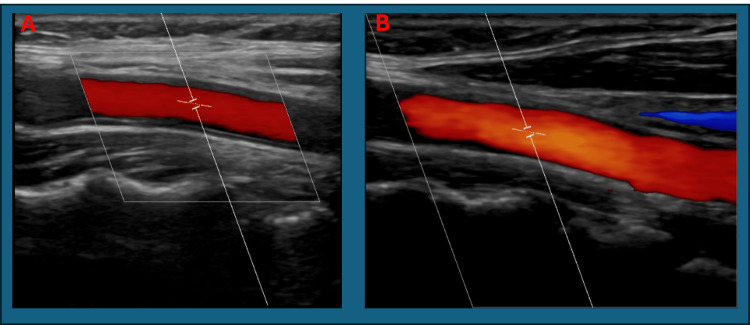 Figure 2
Figure 2 Figure 3
Figure 3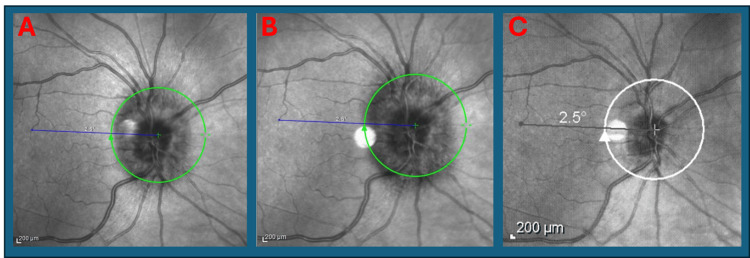 Figure 4
Figure 4 Figure 5
Figure 5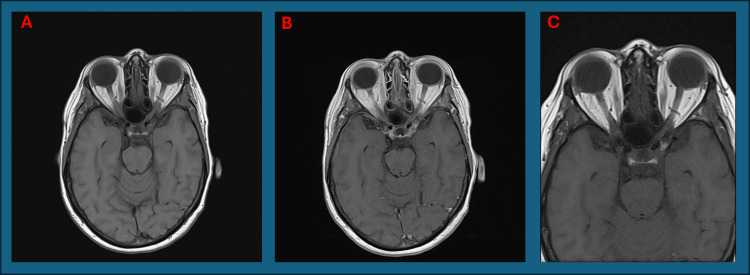 Figure 6
Figure 6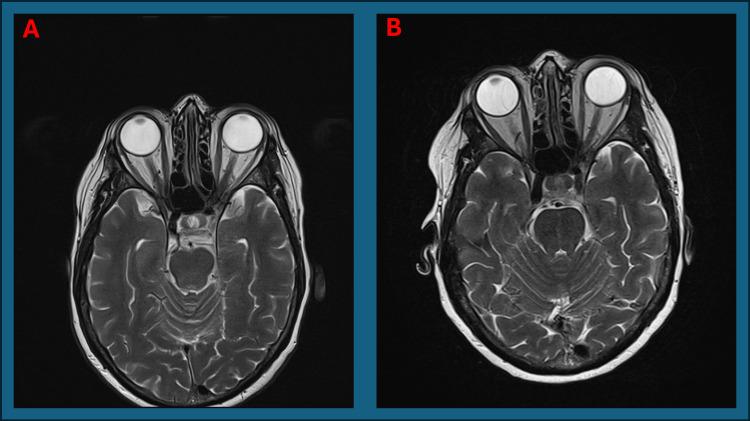 Figure 7
Figure 7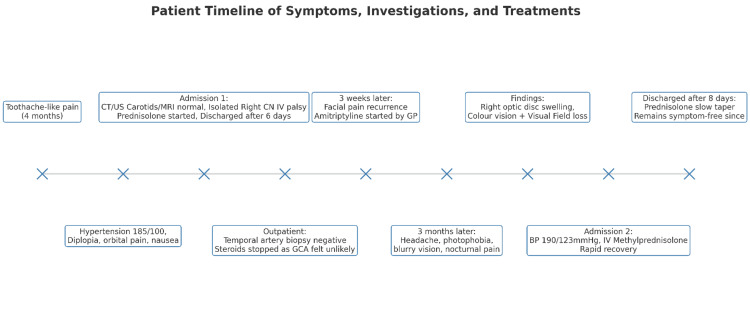 Figure 8
Figure 8| Investigation | Result | Reference Range |
| C-Reactive Protein | 8 mg/L | 0-5 mg/L |
| Erythrocyte Sedimentation Rate | 26 mm/h | 0-20mm/h |
| White Cell Count | 6.4x109/L | 4-11x109/L |
| Electrophoresis Immunoglobulin G (IgG) | 11.5 g/L | 7-16 g/L |
| Investigation | Result | Reference Ranges |
| C-Reactive protein | 11 mg/L | 0-5 mg/L |
| Erythrocyte sedimentation rate | 22 mm/h | 0-20 mm/h |
| White cell count | 6.1x109/L | 4-11x109/L |
| Ferritin | 179 µg/L | 30-400 µg/L |
| Connective tissue disease screen | Negative | Screened for Ro, La, Sm, RNP, Jo-1, Scl-70, dsDNA, Centromere, Mi-2, Ku, Th/To, RNA Polymerase III, PM-Scl, PCNA, Ribosomal P protein |
| Anti-myeloperoxidase abs | <3.2 CU | 0-19 CU |
| Anti-proteinase 3 abs | <2.3 | 0-19 CU |
| Immunoglobulin (IgG) electrophoresis | 13.0 g/L | 7-16 g/L |
| Prednisolone tapering regime | |
| Dose of Prednisolone | Duration |
| 60 mg daily | 1 week |
| 50 mg daily | 1 week |
| 40 mg daily | 2 weeks |
| 35 mg daily | 2 weeks |
| 30 mg daily | 2 weeks |
| 25 mg daily | 2 weeks |
| 20 mg daily | 2 weeks |
| Thereafter, weaning of 2.5mg every 4 weeks until 10mg | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · IgG4-Related and Inflammatory Diseases · Otitis Media and Relapsing Polychondritis
Introduction
Giant cell arteritis (GCA) is a systemic granulomatous vasculitis that predominantly affects older adults [1]. It primarily involves large and medium-sized arteries, particularly the branches of the external carotid artery, such as the temporal artery. Its classical symptoms include headaches, reduced or loss of visual acuity and jaw claudication, corresponding to the supplying arteries that are affected. Whilst diplopia is a specific indicator for GCA with cranial nerve (CN) III involvement, CN IV involvement is rarely described [1]. Visual loss, the most feared complication, usually results from arteritic anterior ischaemic optic neuropathy (AAION), occurring in up to 20% of untreated patients [2].
Systemic symptoms may not always present in GCA, at times only with visual signs and symptoms as described as occult GCA [3]. CN involvement in GCA is rare and typically affects CN III or VI [4,5]. Isolated CN IV palsy has been reported only once in the literature [6]. Temporal artery biopsy remains the gold standard for diagnosis but is subject to false-negatives due to skip lesions [7]. Early diagnosis and treatment are essential, as delayed therapy can result in permanent visual impairment [1,7].
We present a rare case of GCA initially manifesting as isolated CN IV palsy and delayed recurrence manifesting as AAION.
Case presentation
We present a 67-year-old lady with a background of right knee meniscal tear, shingles, and psoriasis. She is fully independent and physically active, with no personal or family history of autoimmune or early cardiovascular disease. She is a non-smoker.
First presentation
She initially presented with a hypertension of 185/100 mmHg and a one-day history of sudden-onset binocular vertical diplopia, accompanied by right retro-orbital pain and nausea worsened by eye movement. She had to patch her right eye to manage her diplopia. She also described intermittent, dull right orbital and jaw pain, occurring twice weekly for approximately 20 minutes. Similar, milder episodes had occurred four months earlier and had self-resolved. The pain improved with paracetamol, and nausea was exacerbated when looking down.
She denied headache, scalp tenderness, jaw claudication, vision loss, shoulder or hip girdle symptoms, fever, weight loss, or night sweats. There were no signs of dental issues, morning stiffness, photosensitivity, Raynaud’s phenomenon, cough, or alopecia. Joint and systemic examinations were unremarkable. Her investigations are as detailed in Table 1.
Ocular exam revealed a full range of extraocular movement with no ophthalmoplegia. Stroke was the top differential diagnosis then, and she was loaded on 300 mg aspirin.
Her CT brain was normal (Figure 1). A carotid Doppler ultrasound was performed and was normal (Figure 2). MRI brain was unremarkable (Figure 3). GCA was still felt to be unlikely then.
A: Normal axial CT brain from first presentation. B: Normal axial CT brain from second presentation
A: Normal ultrasound carotid Doppler of right common carotid artery (peak systolic velocity: 112.2 cm/s, end-diastolic velocity: 22.4 cm/s). B: Normal ultrasound carotid Doppler of left common carotid artery (peak systolic velocity: 129.0 cm/s, end-diastolic velocity: 19.5 cm/s)
Normal axial T2 MRI head sequence from first presentation
Ophthalmology identified a positive Parks-Bielchowsky test, suggestive of isolated right CN IV palsy. Fundoscopic exam showed a healthy optic nerve and fundi and no relative afferent pupillary defect (RAPD) was seen. Pupils were equally reactive. The best corrected visual acuity was 0.08 (right) and 0.06 (left).
Rheumatology assessment on day four of her admission noted non-thickened and pulsatile temporal arteries. She had no proximal weakness. Her GCA probability score was 12 given cranial nerve involvement, headache, duration of symptoms and demographics. This placed her in the intermediate risk category [8]. She was started on 60 mg of prednisolone with a tapering plan and discharged after six days of admission.
On outpatient review, her right CN IV palsy had resolved with no superior oblique muscle weakness and she returned to driving. Right temporal artery biopsy revealed only thickening of the internal elastic lamina, consistent with age-related changes. Steroids were discontinued due to low suspicion of GCA.
Three weeks after stopping steroids, her right-sided facial pain returned. Her general physician (GP) suspected trigeminal neuralgia and started Amitriptyline, which provided partial relief.
Second presentation
However, three months later, she presented with worsening headache described as a tight band, photophobia, blurred right vision, and nocturnal awakening due to pain.
On re-evaluation, she had significant right optic disc swelling (Figures 4, 5). Visual acuity was 6/12 (right) and 6/6 (left), with a marked reduction in colour vision (Ishihara: 2/21 right vs 21/21 left). A slight RAPD was present, and visual field testing revealed central and inferior field loss in the right eye. Her extraocular range of motion, retina and macula were normal.
A: Optical coherence tomography (OCT) image of right eye from first presentation in the second recurrence showing swollen optic disc. B: OCT image from ophthalmology follow-up in second recurrence showing persistent right swollen optic disc. C: OCT image three weeks post-discharge from second recurrence showing resolution and normal right optic disc.
Fundus photograph of the right fundus on re-presentation
Two weeks later, her right visual acuity deteriorated further to 6/60, whilst left eye was 6/9. Intraocular pressure was 14 mmHg (right) and 6 mmHg (left). The right pupil was sluggish, and optic disc oedema persisted. There was no conjunctival injection. Her blood pressure was elevated at 190/123 mmHg. Her investigation results are as detailed in Table 2.
She was admitted for treatment with pulsed intravenous methylprednisolone for 1 g per day for three days in view of ocular involvement followed by a tapering course of oral prednisolone from 60 mg. This led to complete resolution in terms of her headache, pain, and colour vision within days.
On examination, the right temporal artery was pulseless. MRI of the head and orbits with contrast were normal (Figures 6, 7). Aquaporin-4 antibodies was negative. Despite atypical features, the overall clinical picture was in keeping with AAION secondary to GCA. The patient's symptom identification, investigation, and treatment timeline is given in Figure 8.
A: Normal axial T1 MRI head sequence pre-contrast from second presentation. B: Normal axial T1 MRI head sequence post-contrast from second presentation. C: Normal Axial T1 MRI Head sequence no contrast used on outpatient review after second discharge
A: Normal axial T2 MRI orbit sequence from second presentation. B: Normal axial T2 MRI orbit sequence on outpatient review after second discharge
The patient was then discharged after eight days of admission with the following the prednisolone tapering regime (Table 3). Safety net advice was also given to seek medical attention and increase her prednisolone dose should her symptoms recur. She was followed up shortly with neurology in the outpatient setting. She was discharged from the neurology service due to reassuring findings. She had an MRI head and orbit as an outpatient, which did not show any intracranial pathology nor cavernous sinus lesion.
Timeline of symptoms, investigations and treatments
She was then seen in the rheumatology clinic three weeks later with complete resolution and no recurrence of her symptoms.
She was also reviewed by the ophthalmology team and orthoptist in the outpatient setting again with reassuring eye exam and normal optical coherence tomography (OCT). Her visual acuity returned to 6/6 in both eyes with intraocular pressure of 14 mmHg in the right eye and 16 mmHg in the left eye. Fundus examination showed a healthy optic disc, with no significant visual field defect and colour vision on Ishihara chart was full bilaterally.
Discussion
The initial presentation of diplopia in GCA is uncommon, observed in only about 5% of cases, most often due to CN VI palsy in isolation followed by CN III palsy [4,5]. In this case, the absence of classical features such as jaw claudication or visual loss, along with a negative temporal artery biopsy, contributed to diagnostic uncertainty. However, temporal artery biopsy has a sensitivity of 85%-90%, and false-negatives due to skip lesions are well documented up to 7% despite being the gold standard investigation [9].
Isolated CN IV palsy in GCA is extremely rare, with only one previously reported case [6]. The reported case had a similar presentation to our encounter with rapid response to prednisolone; however, the patient’s temporal artery biopsy being positive was helpful in clinching the diagnosis [6]. The reported cases of GCA presenting with CN VI palsy were reassuring in terms of response to steroid treatment in more than 90% of patients, which may be mirrored in CN IV palsy presentations too [4].
Furthermore, inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) may be normal in about 7%-20% of patients with GCA [10]. The patient’s hypertension may have contributed to her cranial ischaemic complications, although hypertension itself is not a known risk factor for developing GCA [11]. Nonetheless, it highlights the importance of recognizing vascular risk factors in GCA management.
The European Alliance of Associations for Rheumatology (EULAR) recommends a slow corticosteroid taper over 12 months or more from a starting dose of 40-60 mg a day [7]. In this case, steroids were tapered over 14 weeks rapidly and discontinued, which may have led to an inadequate treatment response and subsequent relapse. A more gradual and lengthier approach to steroid tapering was adopted for the second presentation and the patient remained symptom-free 4.5 months since the onset.
It has been shown that immediate treatment along with prompt workup within 24 hours of presentation can reduce the risk of permanent visual loss [12]. Furthermore, it has been reported that untreated AAION secondary to GCA may lead to contralateral involvement within 10 days [2]. Therefore, in this case, prompt recognition of atypical GCA features at the second presentation, coupled with timely reinstitution of corticosteroids, resulted in reversal of visual symptoms, underscoring the importance of clinical judgment even in the face of negative biopsy and imaging.
Conclusions
This case illustrates a rare presentation of GCA with isolated cranial nerve IV palsy, followed by delayed AAION. It highlights the need for heightened clinical suspicion of GCA in elderly patients presenting with unexplained diplopia, even in the absence of classical features or a positive biopsy. Atypical presentations should not delay corticosteroid initiation, and a prolonged tapering regimen is essential to prevent relapse and irreversible visual loss.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giant cell arteritis (temporal arteritis)Stats Pearl Ameer MA Vaqar S Khazaeni B Treasure Island, FL Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 459376/29083688 · pubmed ↗
- 2Giant cell arteritis presenting as unilateral arteritic anterior ischemic optic neuropathy Cureus Mandura RA 013202110.7759/cureus.16653 PMC 838779334462685 · doi ↗ · pubmed ↗
- 3Occult giant cell arteritis: ocular manifestations Am J Ophthalmol Hayreh SS Podhajsky PA Zimmerman B 5215261251998955973810.1016/s 0002-9394(99)80193-7 · doi ↗ · pubmed ↗
- 4Sixth cranial nerve palsy in giant cell arteritis: a systematic review Arch Rheumatol Sawada H Nishimura Y Tamaki H 479487392024 https://www.archivesofrheumatology.org/full-text/16153950784510.46497/Arch Rheumatol.2024.10528 PMC 11537682 · doi ↗ · pubmed ↗
- 5Giant cell arteritis presenting with multiple cranial neuropathies - case report Neurohospitalist Ye JJ Bouffard MA Brooks E Hung YP Kimchi EY 1881911320223706493410.1177/19418744221139893 PMC 10091440 · doi ↗ · pubmed ↗
- 6Fourth nerve palsy as the presenting manifestation of giant cell arteritis Can J Neurol Sci Jafari S Micieli JA 12202410.1017/cjn.2024.34439539216 · doi ↗ · pubmed ↗
- 72018 Update of the EULAR recommendations for the management of large vessel vasculitis Ann Rheum Dis Hellmich B Agueda A Monti S 19307920203127011010.1136/annrheumdis-2019-215672 · doi ↗ · pubmed ↗
- 8Validation of the Southend giant cell arteritis probability score in a Scottish single-centre fast-track pathway Rheumatol Adv Pract Melville AR Donaldson K Dale J Ciechomska A 06202110.1093/rap/rkab 102PMC 876578935059557 · doi ↗ · pubmed ↗