Trends in the Incidence of Ramsay Hunt Syndrome and Zoster Sine Herpete Following the Introduction of Routine Varicella Vaccination in Hokkaido, Japan
Yasushi Furuta, Hiroko Yanagi, Michiya Matsumura, Keishi Fujiwara

TL;DR
This study found that after routine varicella vaccination in Japan, younger adults had a higher risk of developing HZ-related facial palsy, including Ramsay Hunt syndrome and zoster sine herpete.
Contribution
The study reveals a significant increase in HZ-related facial palsy among 15-29-year-olds post-varicella vaccination, highlighting a new clinical trend.
Findings
The overall proportion of HZ-related facial palsy did not change significantly after routine varicella vaccination.
Among patients aged 15-29 years, the proportion of HZ-related facial palsy increased significantly from 38.9% to 63.3%.
Younger patients had approximately 2.7 times higher odds of developing HZ-related facial palsy after vaccination.
Abstract
Background: Routine varicella vaccination was introduced in Japan in October 2014. A large-scale epidemiological study conducted in Miyazaki Prefecture subsequently reported a marked increase in the incidence of herpes zoster (HZ) among the child-rearing population aged 20-40 years following this introduction. Objective: This study aimed to investigate long-term trends in the incidence of HZ-related facial palsy, Ramsay Hunt syndrome (RHS) and zoster sine herpete (ZSH), among patients with acute peripheral facial palsy (APFP) aged 15 years or older, treated at a single institution in Hokkaido, Japan, over a 15-year period (2007-2022), and to compare the proportions before and after the introduction of routine varicella vaccination. Methods: This retrospective cohort study included 641 patients (15 years old or older) diagnosed with APFP, including Bell’s palsy, ZSH, and RHS, between…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
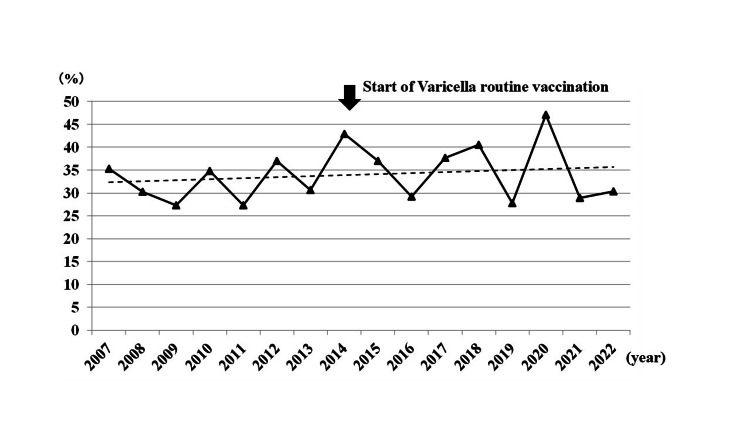 Figure 1
Figure 1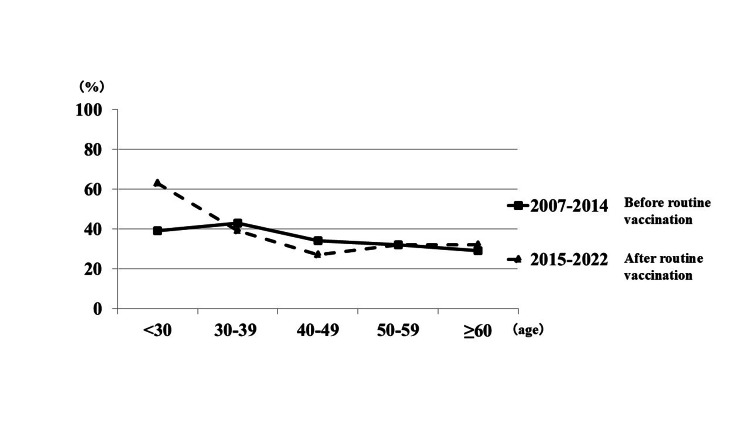 Figure 2
Figure 2| Year | Bell | ZSH | RHS | ZSH + RHS | Total APFP cases | ||||||
| n | % | n | % | n | % | n | % | ||||
| 2007 | 11 | 64.7 | 1 | 5.9 | 5 | 29.4 | 6 | 35.3 | 17 | ||
| 2008 | 30 | 69.8 | 7 | 16.3 | 6 | 14.0 | 13 | 30.2 | 43 | ||
| 2009 | 24 | 72.7 | 4 | 12.1 | 5 | 15.2 | 9 | 27.3 | 33 | ||
| 2010 | 30 | 65.2 | 5 | 10.9 | 11 | 23.9 | 16 | 34.8 | 46 | ||
| 2011 | 24 | 72.7 | 3 | 9.1 | 6 | 18.2 | 9 | 27.3 | 33 | ||
| 2012 | 34 | 63.0 | 10 | 18.5 | 10 | 18.5 | 20 | 37.0 | 54 | ||
| 2013 | 25 | 69.4 | 3 | 8.3 | 8 | 22.2 | 11 | 30.6 | 36 | ||
| 2014 | 24 | 57.1 | 11 | 26.2 | 7 | 16.7 | 18 | 42.9 | 42 | ||
| 2015 | 29 | 63.0 | 13 | 28.3 | 4 | 8.7 | 17 | 37.0 | 46 | ||
| 2016 | 34 | 70.8 | 8 | 16.7 | 6 | 12.5 | 14 | 29.2 | 48 | ||
| 2017 | 33 | 62.3 | 8 | 15.1 | 12 | 22.6 | 20 | 37.7 | 53 | ||
| 2018 | 25 | 59.5 | 7 | 16.7 | 10 | 23.8 | 17 | 40.5 | 42 | ||
| 2019 | 26 | 72.2 | 6 | 16.7 | 4 | 11.1 | 10 | 27.8 | 36 | ||
| 2020 | 18 | 52.9 | 6 | 17.6 | 10 | 29.4 | 16 | 47.1 | 34 | ||
| 2021 | 32 | 71.1 | 5 | 11.1 | 8 | 17.8 | 13 | 28.9 | 45 | ||
| 2022 | 23 | 69.7 | 6 | 18.2 | 4 | 12.1 | 10 | 30.3 | 33 | ||
| Total | 422 | 65.8 | 103 | 16.1 | 116 | 18.1 | 219 | 34.2 | 641 | ||
| Diseases | Before (2007-2014) | After (2015-2022) | Odds ratio | 95% confidential interval | Chi-square value | p-value | ||||
| n | % | n | % | |||||||
| Bell | 202 | 66.4 | 220 | 65.3 | 0.949 | 0.685-1.316 | 0.097 | 0.803 | ||
| HZ-related (ZSH and RHS) | 102 | 33.6 | 117 | 34.7 | 1.053 | 0.760-1.460 | ||||
| Age, yrs | Periods, yrs | Odds ratio | 95% confidential interval | Chi-square value | p-value | |||||
| Before (2007-2014) | After (2015-2022) | |||||||||
| ZHS and RHS (total APFP cases) | % | ZHS and RHS (total APFP cases) | % | |||||||
| <30 | 14 (36) | 38.9 | 19 (30) | 63.3 | 2.714 | 1.009-7.301 | 3.910 | 0.048 | ||
| 30-39 | 18 (42) | 42.9 | 16 (41) | 39.0 | 0.853 | 0.358-2.034 | 0.130 | 0.723 | ||
| 40-49 | 17 (50) | 34.0 | 16 (60) | 26.7 | 0.706 | 0.314-1.587 | 0.698 | 0.403 | ||
| 50-59 | 18 (56) | 32.1 | 21 (66) | 31.8 | 0.985 | 0.462-2.100 | 0.001 | 0.970 | ||
| ≥60 | 35 (120) | 29.2 | 45 (140) | 32.1 | 0.869 | 0.513-1.473 | 0.264 | 0.604 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Facial Nerve Paralysis Treatment and Research · Ocular Diseases and Behçet’s Syndrome
Introduction
Varicella-zoster virus (VZV) is not eliminated from the body after primary varicella (chickenpox) infection. Instead, it remains latent in the sensory ganglia throughout life. Reactivation of latent VZV, typically occurring years or even decades later, results in herpes zoster (HZ, shingles). Ramsay Hunt syndrome (RHS), also known as herpes zoster oticus, is characterized by zoster lesions around the auricle or in the oropharynx, acute peripheral facial palsy (APFP), and symptoms involving the vestibulocochlear nerve. VZV reactivation can also cause APFP in the absence of skin lesions, a condition known as zoster sine herpete (ZSH). ZSH can be distinguished from Bell’s palsy using appropriate serological and/or molecular diagnostic methods [1].
RHS accounts for approximately 20% of APFP cases, and ZSH is diagnosed in 8-19% of patients initially presumed to have Bell’s palsy [2,3]. Consequently, VZV reactivation is the second most common cause of APFP, following Bell’s palsy. Clinically, APFP associated with VZV reactivation tends to be more severe and is associated with poorer recovery outcomes compared to Bell’s palsy [4].
In Japan, the varicella vaccine (Oka strain) had been available since 1987; however, until October 2014, it was administered only as a voluntary (nonroutine) vaccination. The uptake under this voluntary program remained relatively low, with reported national coverage of approximately 40% [5]. Consequently, prior to the introduction of routine childhood immunization in October 2014, the vaccine’s impact on overall varicella epidemiology was limited [5]. Routine varicella vaccination has led to a marked decline in annual varicella incidence [5,6].
Previous epidemiological studies analyzing HZ incidence by age group revealed a transient decline in individuals in their 30s, followed by a steady increase with advancing age [7]. This temporary reduction in incidence among people in their 30s has been attributed to the boosting effect, in which frequent exposure to pediatric varicella cases stimulates cell-mediated immunity against VZV in child-rearing adults [7,8]. With the widespread adoption of varicella vaccination and the resulting decline in natural varicella infections, it has been hypothesized that this boosting effect is diminished, potentially leading to a decline in VZV-specific immunity among adults and an increased risk of HZ reactivation [9,10]. A recent study reported an increased incidence of HZ following the introduction of routine varicella vaccination in Japan, particularly among the child-rearing population aged 20-40 years [11].
Therefore, to better understand the long-term epidemiological trends in HZ-related facial palsy (RHS and ZSH) in the context of routine childhood varicella vaccination, we conducted a retrospective study of patients aged 15 years or older with APFP treated at a single institution in Hokkaido, Japan. The aim of this study was to evaluate changes in the proportion of HZ-related facial palsy among these patients over a 15-year period (2007-2022) and to compare the proportions before and after the introduction of routine varicella vaccination.
Materials and methods
Study population
This retrospective observational cohort study included patients aged 15 years or older who were diagnosed with APFP, including Bell’s palsy, ZSH, and RHS, and who presented to Teine Keijinkai Hospital between July 2007 and December 2022. All patients were treated within seven days of symptom onset.
Of the 767 eligible patients, 126 who did not undergo serological testing were excluded from the analysis. Consequently, a total of 641 patients with APFP were included in the final analysis. All patients were residents of Hokkaido Prefecture.
Study setting
Teine Keijinkai Hospital is a 660-bed tertiary care hospital located in Sapporo, Hokkaido, Japan, providing comprehensive emergency and outpatient services to a large regional population. The hospital serves as a major referral center for neurological and otolaryngological disorders, enabling consistent surveillance of APFP cases.
Data collection
Data were retrospectively collected from electronic medical records. Clinical data were extracted by the staff of the Medical Support Division. Extracted variables included patient demographics, clinical diagnosis (Bell’s palsy, ZSH, or RHS), symptom onset and timing of treatment initiation, serological test results, and residential area. Only patients with completed VZV serological testing were included in the final analysis.
Diagnosis of VZV reactivation in APFP
Paired serum samples were collected from all APFP patients at the initial visit and again 2-4 weeks later (convalescent phase). VZV-specific immunoglobulin (Ig) G and IgM antibodies were measured using an enzyme-linked immunosorbent assay (ELISA) performed at an external accredited laboratory (SRL Laboratory, Tokyo, Japan). According to the manufacturer’s criteria, VZV IgG titers <2.0 are interpreted as negative, and VZV IgM titers <0.80 are considered negative. VZV reactivation was diagnosed when either a ≥twofold increase in anti-VZV IgG titers was observed or when IgM antibodies were positive. In addition, patients with a high anti-VZV IgG titer (≥50 × 10² mIU/mL) were considered positive for VZV reactivation if an increase in anti-VZV IgG was confirmed in the convalescent sample [12,13].
RHS was diagnosed in patients with APFP who exhibited typical zoster lesions on the auricle, in the oropharyngeal epithelium, or who presented with cochleovestibular symptoms. All RHS cases had serologically confirmed VZV reactivation. ZSH was diagnosed in patients with no zoster lesions or cochleovestibular symptoms, but in whom serologic evidence of VZV reactivation was present. All remaining cases were diagnosed with Bell’s palsy.
Calculation of HZ rate
The annual rate of HZ-related facial palsy was calculated by dividing the number of patients with RHS and ZSH by the total number of APFP patients seen each year. The same method was applied to calculate the age-specific incidence rates.
Data analysis
Descriptive statistics were used to present the annual and age-stratified proportions of Bell’s palsy, ZSH, and RHS. The proportions of HZ-related facial palsy (ZSH and RHS combined) before and after the introduction of routine varicella vaccination were compared using chi-square tests. A two-sided p-value < 0.05 was considered statistically significant. We also calculated odds ratios with 95% confidence intervals to evaluate the effect size. All analyses were performed using EZR [14] (Saitama Medical Center, Jichi Medical University, Japan), which is a graphical user interface for R.
Ethical approval
This retrospective cohort study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Board of Teine Keijinkai Hospital, Sapporo, Japan.
Results
VZV reactivation in APFP patients
Among the 641 patients diagnosed with APFP, 116 presented with typical zoster lesions on the skin or oral epithelium and were thus diagnosed with RHS. VZV reactivation in these patients was confirmed by ELISA. Of the remaining 525 patients tested using paired sera, 103 (19.6%) were diagnosed with ZSH based on evidence of VZV reactivation. Overall, 219 of the 641 APFP patients (34.2%) showed evidence of VZV reactivation at the onset of facial paralysis and were classified as having HZ-related facial palsy. The remaining 422 patients were diagnosed with Bell’s palsy.
Annual rate of HZ in APFP patients
Table 1 summarizes the number of APFP patients per year. The annual proportion of HZ-related facial palsy (ZSH and RHS) during the 15-year study period is shown in Figure 1. The proportion was 33.6% (102/304 cases) before the introduction of routine varicella vaccination and 34.7% (117/337 cases) after its implementation (Table 2). There was no significant difference between the two periods (odds ratio, 1.053; 95% CI, 0.760-1.460; χ² = 0.097; p = 0.803).
Annual trend in the proportion of herpes zoster-related facial palsy among patients with acute peripheral facial paralysisZSH: zoster sine herpete; RHS: Ramsay Hunt syndromeThe line graph depicts the annual proportion (%) of herpes zoster-related facial palsy (ZSH and RHS) among patients with acute peripheral facial paralysis from 2007 to 2022. The introduction of routine varicella vaccination (October 2014) is indicated by a vertical arrow
Age-specific rate of HZ in APFP patients
Next, we analyzed the age-specific rates of HZ-related facial palsy during the prevaccination (2007-2014) and postvaccination (2015-2022) periods (Table 3). In patients aged 15-29 years, the proportion of HZ significantly increased from 38.9% (14/36) in the prevaccination period to 63.3% (19/30) in the post-vaccination period (odds ratio, 2.714; 95% CI, 1.009-7.301; χ² = 3.910; p = 0.048, chi-square test). This odds ratio indicates that patients in this age group had approximately 2.7 times higher odds of developing HZ-related facial palsy after the introduction of routine varicella vaccination compared with the prevaccination period, which is consistent with the statistically significant difference observed. In contrast, no significant differences were observed in any age group over 30 years between the two time periods. Figure 2 illustrates the changes in age-specific rates of HZ-related facial palsy across both periods.
Age-specific change in the proportion of herpes zoster-related facial palsy before and after routine varicella vaccinationZSH: zoster sine herpete; RHS: Ramsay Hunt syndromeLine graphs comparing the age-specific proportions (%) of herpes zoster-related facial palsy (ZSH and RHS) among patients with acute peripheral facial paralysis during the prevaccination (2007-2014) and postvaccination (2015-2022) periods
Discussion
In Japan, routine varicella vaccination was introduced in October 2014 for children aged 12-36 months old. Following its implementation, the number of reported varicella cases among children under five years of age declined rapidly [6]. As the incidence of varicella in children has decreased, the booster effect of natural infection has diminished. This raised concerns about a possible increase in HZ incidence among adolescents and a younger age at onset [9,10]. In the United States, the incidence of HZ among individuals aged 1-29 years has temporarily increased following the introduction of routine varicella vaccination [15]. However, more than 25 years after the program's initiation, the incidence has been declining [15].
The Miyazaki study, a large-scale epidemiological study in Japan [7], reported that the incidence of HZ was already increasing among older adults even prior to the introduction of routine vaccination in 2014. While the exact reasons remain unclear, contributing factors may include societal shifts toward nuclear families with fewer children, improved access to healthcare and increased consultation rates, and reduced natural boosting due to the milder clinical course of varicella and HZ resulting from widespread antiviral use. Furthermore, the Miyazaki study noted an increased incidence of HZ among child-rearing generations (20-40 years) following the introduction of routine vaccination [11], likely due to further attenuation of the natural booster effect.
In the present study, we investigated trends in the incidence of ZSH and RHS among patients with APFP in Hokkaido before and after the initiation of routine varicella vaccination. No significant change in the overall proportion of HZ-related facial palsy (ZSH and RHS) was observed. We observed annual fluctuations in the proportion of HZ cases, which may reflect known seasonal and year-to-year variability in VZV reactivation [7]. Notably, however, a significant increase in the proportion of HZ among patients aged 15-29 years was observed after the introduction of routine childhood varicella vaccination. This finding is consistent with the Miyazaki study, which reported a similar increase in this younger age group in Japan [11]. To provide a broader epidemiological context, we also referenced long-term data from the United States, where the incidence in this age group initially increased but subsequently declined after 25 years of widespread vaccination [15]. These international data are provided solely as epidemiological context and are not intended to imply any direct extrapolation from our findings.
The preceding section addressed age-specific trends in the incidence of HZ in relation to childhood varicella vaccination. In contrast, HZ prevention in older adults involves a different public-health strategy, namely, the use of zoster vaccines. The incidence and the severity of HZ tend to increase with age. Elderly patients also have a higher risk of developing postherpetic neuralgia, which significantly impairs their quality of life. A large US clinical trial demonstrated that HZ vaccination (Zostavax®) significantly reduced the incidence of both HZ and postherpetic neuralgia in individuals aged ≥50 years [16,17]. In Japan, the live attenuated varicella vaccine (BIKEN®) was approved in 2016 for HZ prevention in people aged 50 and older, as it contains a viral titer similar to that of Zostavax®. Additionally, the recombinant subunit vaccine Shingrix® was approved in 2018 [18]. With wider adoption of these vaccines, the incidence of ZSH and RHS may decrease.
Clinically, recovery rates for facial nerve palsy caused by ZSH and RHS remain modest, at approximately 60-70%, with many patients experiencing sequelae. While a meta-analysis of real-world data showed that Zostavax® reduced the incidence of ocular HZ by 30% [19], no such evidence currently exists for RHS. Moreover, HZ vaccines are currently approved only for individuals aged 50 and older, leaving younger patients ineligible. Therefore, careful diagnosis and appropriate treatment of APFP are especially important for patients aged 15-29 years.
This study had several limitations. First, we did not analyze the incidence of Bell’s palsy, ZSH, or RHS in the general population. Instead, we calculated only the proportion of ZHS and RHS among the APFP cases. This assumes that the overall incidence of Bell’s palsy remained stable throughout the study period. Unfortunately, no comprehensive epidemiological data on Bell’s palsy have been reported in Japan since a nationwide survey in collaboration with 28 medical facilities in 1988 [20]. However, in our cohort, the annual number of Bell’s palsy cases ranged from 23 to 34 (mean: 26.4), with no notable fluctuations. Second, this study was conducted at a single institution in northern Japan with a limited number of patients, making it difficult to determine whether the observed patterns are unique to our institution or reflect broader epidemiological trends. In addition, the diagnostic work-up and clinical diagnoses were performed at a single institution and may differ from practices at other centers, which could limit the generalizability and reproducibility of our findings. Nonetheless, our findings are consistent with those of a large-scale study conducted in Miyazaki Prefecture, southern Japan, particularly among younger patients [11]. Third, we should consider selection bias inherent to tertiary care hospital-based datasets, as well as potential misclassification bias between ZSH and Bell’s palsy. However, the use of standardized serological criteria to distinguish ZSH from Bell’s palsy represents a methodological strength of our study. The proportion of ZSH among patients diagnosed with Bell’s palsy (19.6%) was nearly identical to that reported in a Japanese multi-institutional study (18.7%) [2].
Although future studies incorporating multicenter or national registry data would substantially enhance the generalizability and relevance of the findings, our results provide a valuable baseline for future research on the incidence of HZ in APFP patients following the introduction of routine varicella vaccination in Japan. The rising incidence of HZ-related facial palsy among younger individuals in Hokkaido should be carefully considered in the diagnosis and management of APFP.
Conclusions
In this 15-year cohort study of 641 patients with APFP in Hokkaido, Japan, no significant overall change was observed in the proportion of HZ-related cases, including ZSH and RHS, before and after the introduction of routine varicella vaccination in 2014. However, a significant increase in HZ among APFP patients aged 15-29 years suggests a reduction in VZV immunity due to decreased natural exposure following widespread childhood vaccination.
Although recovery rates for APFP caused by ZSH and RHS remain modest, early diagnosis and timely antiviral treatment are essential. Continued epidemiological surveillance and multicenter studies are warranted to validate these findings and to better understand the long-term impact of routine varicella vaccination on VZV reactivation in Japan.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Detection of varicella-zoster virus DNA in patients with acute peripheral facial palsy by polymerase chain reaction and its use for early diagnosis of zoster sine herpete J Med Virol Furuta Y Fukuda S Suzuki S Takasu T Inuyama Y Nagashima K 3163195219979210042 · pubmed ↗
- 2Reactivation of herpes simplex virus type 1 and varicella-zoster virus and therapeutic effects of combination therapy with prednisolone and valacyclovir in patients with Bell's palsy Laryngoscope Kawaguchi K Inamura H Abe Y 14715611720071720294510.1097/01.mlg.0000248737.65607.9e · doi ↗ · pubmed ↗
- 3Valacyclovir and prednisolone treatment for Bell's palsy: a multicenter, randomized, placebo-controlled study Otol Neurotol Hato N Yamada H Kohno H 4084132820071741404710.1097/01.mao.0000265190.29969.12 · doi ↗ · pubmed ↗
- 4Ramsay Hunt facial paralysis: clinical analyses of 185 patients Otolaryngol Head Neck Surg Robillard RB Hilsinger RL Jr Adour KK 292297951986310877610.1177/01945998860953 P 105 · doi ↗ · pubmed ↗
- 5Universal varicella vaccine immunization in Japan Vaccine Yoshikawa T Kawamura Y Ohashi M 196519703420162694471110.1016/j.vaccine.2016.02.058 · doi ↗ · pubmed ↗
- 6Japan Institute for Health Security. Changes in varicella outbreak trends after routine varicella vaccination-from the Survey of Infectious Disease Outbreak Trends, as of Week 262022 https://id-info.jihs.go.jp/niid/ja/varicella-m/varicella-idwrs/10892-varicella-20220113.html
- 7Epidemiology of herpes zoster and its relationship to varicella in Japan: a 10-year survey of 48,388 herpes zoster cases in Miyazaki prefecture J Med Virol Toyama N Shiraki K 205320588120091985646610.1002/jmv.21599 · doi ↗ · pubmed ↗
- 8Contacts with varicella or with children and protection against herpes zoster in adults: a case-control study Lancet Thomas SL Wheeler JG Hall AJ 67868236020021224187410.1016/S 0140-6736(02)09837-9 · doi ↗ · pubmed ↗