Examining the Carbon Footprint of Orthopaedic Outpatient Care and Comparing the Emissions From In-Person Versus Virtual Models of Care: A Systematic Review
Lucy Lee-Smith, Joseph Andrews

TL;DR
This paper reviews how virtual care in orthopaedics reduces carbon emissions compared to in-person visits, mainly by cutting down patient travel.
Contribution
The study systematically compares emissions from virtual and in-person orthopaedic care, highlighting travel reduction as a key factor.
Findings
Virtual care reduces carbon emissions by a median of 11.8 kgCO₂e per patient interaction.
Patient travel is the primary source of emission reduction in virtual care models.
Low certainty of evidence calls for better measurement of travel and associated emissions.
Abstract
Healthcare systems are responsible for a significant proportion of global greenhouse gas emissions. Trauma and orthopaedics has an exceptionally high emission profile in comparison to other specialities. This systematic review synthesises the available literature regarding the impact of virtual care/telemedicine on the carbon footprint of outpatient orthopaedics. Nine studies, encompassing over 500,000 patients, were included following a search across major databases. Virtual care has consistently been shown to have a smaller carbon footprint than traditional in-person appointments, primarily by reducing patient travel, resulting in a median reduction of 11.8 kgCO₂e per patient interaction. Secondary benefits, such as patient cost savings and improved accessibility, were also observed. However, the certainty of evidence was low due to the risk of bias across the studies; future research…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
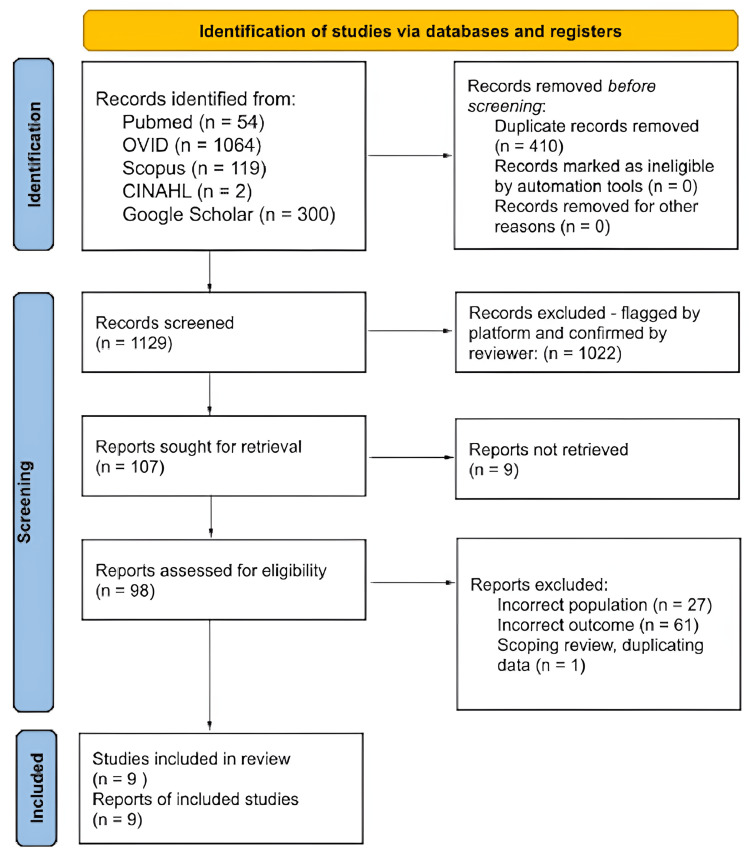 Figure 1
Figure 1 Figure 2
Figure 2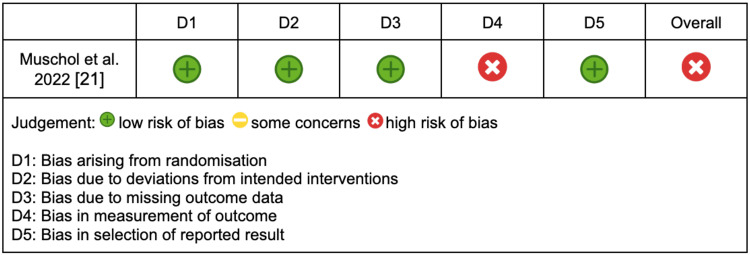 Figure 3
Figure 3| PICO research question | |
| Population | All patients attending orthopaedic outpatient services |
| Intervention | Virtual outpatient care |
| Comparators | In-person or hybrid outpatient care |
| Outcomes | Carbon footprint/GHG emissions/kgCO2e/lifecycle assessment/LCA |
| Author | Design | Sample size and setting | Intervention | Method to estimate emissions | Reduction in CO2e (kg) | Cost savings |
| Richards et al. 2022 [ | Retroscpective cohort | 52 - hip arthroplasty clinic - UK DGH | Telephone clinic | Travel, lighting, heating, waste vs nil | 62.9 | £7.18 for the patient, £162 per patient for the hospital |
| Parker et al. 2025 [ | Cross-sectional study | 508394 - general orthopaedics - USA large hospital and associated community clinics | Virtual - not explicitly specified | Travel, supplies, facility energy use vs technology energy use | 7.08 | Not reported |
| Arndt et al. 2023 [ | Observational | 51 - general orthopaedics - German University Hospital | Video | Travel vs power consumption of the data centre | 11.8 | Not reported |
| Platt and Bolland 2025 [ | Retrospective analysis | 319 - arthroplasty clinic - UK large hospital | Video - MS teams and telephone | Travel, heating, lighting, waste vs nil | 65.2 | Not reported |
| Curtis et al. 2021 [ | Retrospective cohort | 52 - trauma clinic - UK DGH | NF2F - not explicitly specified | Travel, heating, lighting, waste vs nil | 59.1 | £8.96 - 12 for the patient |
| Fawdry et al. 2025 [ | Retrospective service review | 107 - hand surgeon clinic - UK | Telephone | Travel vs nil | 2.28 | £1.84 - 2.80 for the patient |
| Arora et al. 2025 [ | Retrospective review | 416 - hand clinic - USA VA medical centre | Telephone | Travel vs nil | 54.0 | $30.69 for the patient |
| Wang et al. 2021 [ | Retrospective cross-sectional analysis | 298 - spinal clinic - USA hospital | Optimised telehealth - not explicitly specified | Travel, clinic facilities, telehealth infrastructure, laboratory energy vs the same | 8.09 | Not reported |
| Muschol et al. 2022 [ | Prospective RCT | 52 - general orthopaedics - German University Hospital | Video - digital health app | Travel vs nil | 11.4 | €9.53 for the patient |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClimate Change and Health Impacts · Telemedicine and Telehealth Implementation · Global Health and Surgery
Introduction and background
Sustainability has gained interest in healthcare, with a strong intent to transition to greener practices [1]. The United Kingdom’s National Health Service has pledged to become the first carbon net-zero healthcare system by 2040 [2]. This evolution is crucial, as global healthcare systems contribute substantially to climate change, accounting for approximately 5% of global greenhouse gas (GHG) emissions [3].
Trauma and orthopaedics is one of the top three highest-emitting specialities [4]. This is partially due to the high volume of patients requiring regular follow-up, imaging, and examinations, which often involve travelling long distances. Notably, 7% of healthcare system emissions are derived from transportation [5]. A solution to this could be the adoption of virtual care or telemedicine, the delivery of patient care using technology, as conducting an outpatient review remotely negates the need for patient travel.
Telemedicine has been shown to lower the carbon footprint of healthcare, demonstrated in a 2024 systematic review [6]. The safety and financial advantages of virtual orthopaedic outpatient care are also well-supported by research [7]. To ascertain how telemedicine affects the carbon footprint of outpatient orthopaedic care, in particular, this systematic review synthesises currently available data in this field.
Review
Methods
A systematic review was conducted in accordance with the standards described in the Cochrane Handbook and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [8,9]. It is registered in the International Prospective Register of Systematic Reviews (PROSPERO) under Protocol No. CRD420251132499.
Search Strategy and Study Selection
Systematic searches were conducted from 27th to 29th September 2025 across multiple databases, including PubMed, Scopus, Ovid (MEDLINE and Embase), CINAHL, and Google Scholar, using specific PICO boolean strings (Appendices), as described in Table 1.
We included peer-reviewed studies published in English from 2008 onwards that examined patients attending orthopaedic outpatient services. Eligible studies evaluated virtual outpatient care (including telemedicine) compared with in-person or hybrid outpatient care. They reported empirical data on environmental outcomes, such as carbon footprint, GHG emissions, kgCO₂e, or life cycle assessment, including patient travel-related emissions. The post-2008 timeframe was applied to ensure technological relevance and comparability of sustainability outcomes. Studies were excluded if they focused on non-orthopaedic specialities or inpatient care, did not report emissions data or other environmental outcomes, or were published as reviews, editorials, or conference abstracts/posters without full empirical data. Publications not available in English and those published prior to 2008 were also excluded.
Due to the high volume of records retrieved from Google Scholar, only the first 300 results sorted by relevance were screened. Google Scholar was used as a supplementary search platform to identify peer-reviewed studies that may not yet be indexed or easily retrievable through traditional bibliographic databases. Search strings are detailed in the Appendices section.
Search results were imported into a reference manager, Zotero, and a systematic review platform, Rayyan, for practicality. The screening process was conducted in two distinct stages. Initially, titles and abstracts were reviewed against the predetermined inclusion criteria, followed by a full-text screening of potentially relevant articles. All screening and subsequent data extraction were carried out independently by two reviewers to ensure accuracy, and any discrepancies or ambiguities were settled through discussion to reach a consensus.
Data Extraction and Synthesis
Relevant data was extracted and recorded in a standardised form. Key data included study details (author, year, journal, country, design), population (setting, subspeciality, sample size), and intervention details (virtual platform, comparator, conversion methods). They reported outcomes (emissions in kgCO₂e, energy use, travel data and assumptions, and cost). To facilitate comparison, emission outcomes were converted to reductions in kgCO₂e per patient interaction and mean patient travel in miles.
The final list of eligible studies was assessed for risk of bias using established tools. The Risk of Bias in Non-randomised Studies of Interventions (ROBINS-I) tool was used for all non-randomised studies, and the Cochrane Risk of Bias 2 (RoB 2) tool was applied to the sole randomised controlled trial (RCT) [10,11]. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to rate the certainty of the evidence synthesised [12].
Due to heterogeneity in methodologies and modelling assumptions, a random-effects meta-analysis was not feasible. A narrative synthesis was performed to summarise and interpret the findings of the literature.
Results
Figure 1 displays the PRISMA flow diagram, outlining the study identification and screening process used in this systematic review [9]. The search encompassed 1129 records across all databases after duplicates were removed. Nine articles met the inclusion criteria for the analysis.
PRISMA sheet for the studies identified for reviewPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Eight of the included studies were non-randomised retrospective cohort studies; therefore, the ROBINS-I tool was applied to assess quality and outcomes presented in Figure 2 [13-20]. A predominant source of bias arose from the measurement of outcomes across all eight studies, specifically related to the reliance on assumed travel data rather than direct measurement. This limitation resulted in a unanimous overall rating of serious bias for these non-randomised studies.
ROBINS-I tool for assessing risk of bias in non-randomised studiesROBINS-I: Risk of Bias in Non-randomised Studies of Interventions
One study was an RCT and was assessed using the RoB 2 tool, with the results displayed in Figure 3 [21]. This study received an overall rating of high risk of bias, primarily driven by the same outcome measurement assumptions regarding patient travel and emissions calculations as in the non-randomised studies.
RoB 2 assessment for RCTRoB 2: Risk of Bias 2, RCT: randomised controlled trial
Table 2 summarises the characteristics and outcomes of the nine studies included. Studies were conducted between 2021 and 2025 in the United Kingdom (UK), the United States of America (USA), and Germany. The sample sizes varied significantly across the articles, as did the data sources and methods used to estimate emissions.
Reported Carbon Footprint Impact
All nine studies consistently reported a reduction in carbon footprint, predominantly attributed to decreased patient travel. The magnitude of this reduction, measured in kilograms of carbon dioxide equivalents (kgCO₂e), ranged from 2.28 to 65.2, with a median reduction of 11.8 kgCO₂e.
All studies derived emission data from estimates rather than direct measurement at the patient level. Emissions were derived from estimated patient travel distances using study-specific conversion factors.
Variability in Emissions Estimation Methods
A significant finding was the lack of consistency for converting patient travel to kgCO₂e, with no more than two studies using comparable methods. Two studies used the UK government GHG reporting conversion factors 2020, which estimate 0.28 kgCO₂e per mile [13,17]. Whilst another two used the Environmental Protection Agency GHG equivalences calculator, which estimates 0.411 kgCO₂e per mile in an average petrol car [14,19]. A further two used the computer programme TREMOD, developed by the German Federal Environment Agency, which assumes 0.143 kgCO₂e per kilometre in a car [15,21]. A single study converted average patient travel distance to kgCO2e using the Royal Automobile Club emission data, which, similar to the UK government, suggests a car produces 0.28 kgCO2e per mile [16]. The final two studies did not quote their conversion methods but used an online calculator or a life cycle assessment [18,20].
Assumptions regarding the mode of patient travel also differed. The majority of studies assumed that all patients travelled by car from their home address [13-16,19-21]. Only two studies deviated from this assumption; one surveyed patients to determine their actual travel modes (82% car, 18% other modes), whilst the other used Census data to estimate a probable 80% car-use rate [17-18].
Emission Sources Included
Five of the nine studies accounted for secondary emissions associated with clinic operations such as lighting, heating, and waste [13,14,16,17,20]. One study quoted 0.026 kgCO₂e per appointment, and another reported 0.004 kgCO₂e per appointment for their virtual platforms [14,15]. A single study described a life cycle assessment [20].
Certainty of Evidence
The certainty of evidence, assessed using the GRADE approach, was rated as low.
Reported Secondary Impacts
Five of the nine studies extended their analyses to secondary impacts, including patient time, cost savings, and accessibility benefits [13,17-19,21]. The primary benefit identified for patients was financial savings on petrol/fares and parking, followed by time saved from commuting and absence from work or school. Reported cost savings have been detailed in Table 2. These costs were not converted into a single currency to avoid introducing ambiguity from year-to-year exchange rate fluctuations. The certainty of the evidence for secondary impact data was low, as these outcomes were not directly measured in any study.
Subspecialities Analysis
The literature encompassed a variety of orthopaedic subspecialities, including general orthopaedics, trauma, hip arthroplasty, hand surgery, spinal surgery, and knee and shoulder surgery. No discernible correlation was found between the specific orthopaedic subspeciality studied and the magnitude of carbon footprint reduction achieved through the introduction of virtual care.
Discussion
Synthesising nine studies and encompassing 509,869 patients, the review demonstrated a median reduction of 11.8 kgCO₂e per patient, associated with a median travel distance of 24.6 miles. There was considerable variation in travel distance, ranging from 12 to 129.9 miles. Emission data was extrapolated from travel data using assorted conversion methods. This reliance on assumption introduced a notable risk of bias in the measurement of outcomes in both the ROBINS-I and RoB2 tools, as described in Figures 1-2. This introduced uncertainty regarding absolute effect estimates, as reflected by the low GRADE score.
These findings align with wider telemedicine literature. Van der Zee et al. conducted a systematic review assessing the carbon footprint of telemedicine across all medical specialities. Their overall conclusion that telemedicine reduces the healthcare carbon footprint by lowering patient travel aligns with and reinforces the findings of this review. They reported an average reduction of 25.6 kgCO₂e per consultation, primarily driven by reduced patient travel [6]. This figure is higher than the reductions observed in this review, which is consistent with their substantially greater median travel distance of 131 km per patient. Interestingly, in this review, the study that reported the lowest average patient travel distance also found the smallest reduction in carbon footprint with the introduction of telephone follow-up [18]. However, one study recorded considerably higher patient travel distances than the other studies, yet their reported kgCO₂e reduction was not an anomaly amongst the results [15]. This highlights the heterogeneity in emission calculation methods across the studies in this review.
Although patient travel was the dominant contributor to emissions savings, the methods used to estimate travel-related emissions were often simplistic. All included studies assumed petrol car travel and applied generic conversion factors, rather than capturing real-world driving patterns. The use of public transport should be considered more readily, and future work could also incorporate emissions measurement systems, routinely used in automotive testing, which more accurately quantify real-world emissions [22]. The increasing uptake of hybrid and electric vehicles may also reduce the relative benefit of telemedicine over time [23]. None of the studies accounted for evolving transport trends, and failure to include these variables limits the contemporary relevance and precision of their estimates.
The scope of emissions was often limited across the studies. Four studies did not consider secondary emissions associated with clinic operations such as lighting, heating, and waste. Emissions from virtual care were largely ignored, but when accounted for, their magnitude varied considerably. The unmeasured variables increased the risk of bias due to confounding in the ROBINS-I tool, which was depicted in Figure 2. The systematic review across all medical specialities also highlighted the omission of key variables in many primary studies, such as heating, lighting, and staff travel. It emphasised the need for streamlined life cycle assessments to strengthen the evidence base [6]. No study in this review reported whether clinicians conducted virtual clinics from home or from their workplace, and therefore, none incorporated staff commuting emissions into their calculations. Current practice suggests that most clinicians deliver virtual consultations on-site, meaning associated emissions remain unchanged. However, as digitalisation and flexible working become more widespread, remote clinic delivery may become feasible, potentially amplifying the carbon savings attributable to telemedicine. In the same vein, orthopaedic follow-up often requires obtaining a radiograph prior to the review. Patients may travel shorter distances for an X-ray than for a clinic, but the impact on the carbon footprint should be considered. Future analyses should capture these nuances to more accurately quantify the complete environmental impact of virtual care pathways.
The feasibility and equity of telemedicine warrant consideration. Orthopaedic outpatient populations include a large proportion of older adults, many of whom may have limited digital literacy or restricted access to appropriate technology. One study reported that patients unable to participate in video consultations were, on average, 17 years older than those who could [17]. This reinforces the need for structured triage systems to ensure only clinically appropriate and technologically capable patients are issued virtual appointments. The study conducted at a Veterans Affairs medical centre reported the greatest patient travel distance [19]. Excessive travel distance is a known barrier to accessing healthcare for many veterans, and reducing the need for travel provides significant accessibility benefits in this population [24].
Despite the limitations discussed, this study has methodological strengths that enhance the validity of its findings. It was conducted in accordance with a predefined protocol and adhered to PRISMA guidance, reducing bias in study selection and reporting. We used a structured PICO framework to run a broad, systematic search and capture all the necessary evidence. For reliability, two reviewers independently screened and extracted the key data. Only peer-reviewed primary studies were included, and established tools were used to appraise the risk of bias and certainty of evidence to provide a transparent evaluation of study quality.
Achieving net-zero healthcare emissions is a strategic priority for health systems worldwide. Outpatient services and exceptionally patient travel represent meaningful and modifiable contributors to the healthcare carbon footprint. While telemedicine is not a complete solution for net-zero healthcare, the consistent reduction in travel-related emissions demonstrated in this review supports its immediate implementation as a decarbonisation strategy. The findings highlight both the potential environmental benefits of virtual orthopaedic care and the areas that require refinement to achieve maximum future impact.
Conclusions
Implementing or optimising existing virtual outpatient orthopaedic care pathways offers a solution that benefits both the planet and the patient. Although telemedicine is not a complete solution for net-zero healthcare, it consistently has a smaller carbon footprint than traditional in-person appointments, primarily by reducing patient travel. Patients also receive secondary benefits, including saving money on petrol and fares, taking less time away from work or school, and removing accessibility barriers for those who find long journeys challenging. The current research is consistent in its direction, but most available studies are observational, and the certainty of the evidence is low due to indirectness and assumptions in data collection. Therefore, further RCTs with standardised protocols and direct measurements of emissions are warranted to strengthen these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1upporting the sustainability agenda in healthcare Orthop Trauma Syed H Syed L Stone A Phadnis J 284290362022
- 2Delivering a net zero NHS 11 2025 2025 https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/
- 3The environmental footprint of health care: a global assessment Lancet Planet Health Lenzen M Malik A Li M 2712794202010.1016/S 2542-5196(20)30121-232681898 · doi ↗ · pubmed ↗
- 4Carbon emissions from clinical activities by speciality in secondary and tertiary care in England: an exploratory cross-sectional analysis of routine administrative data Lancet Reg Health Eur Begum H Gray WK Simpson RM Ingleton R Phull MK 1013335420254051977010.1016/j.lanepe.2025.101333 PMC 12167066 · doi ↗ · pubmed ↗
- 5Global road map for health care decarbonization 11 2025 2021 https://healthcareclimateaction.org/roadmap
- 6Assessing the carbon footprint of telemedicine: a systematic review Health Serv Insights van der Zee C Chang-Wolf J Koopmanschap MA van Leeuwen R Wisse RP 117863292412715621720243913939510.1177/11786329241271562 PMC 11320403 · doi ↗ · pubmed ↗
- 7Telemedicine in orthopaedics during COVID-19 and beyond: a systematic review J Telemed Telecare Haider Z Aweid B Subramanian P Iranpour F 3914032820223276227010.1177/1357633 X 20938241 PMC 9124641 · doi ↗ · pubmed ↗
- 8Handbooks and manuals 11 2025 2025 https://www.cochrane.org/authors/handbooks-and-manuals