Eosinophilic Granulomatosis With Polyangiitis Presenting as a Mononeuritis Multiplex Mimicking Guillain-Barré Syndrome
Mohamad Zikir Ismail, Fathin Hadi, Wan Syamimee Wan Ghazali, Bazli Md Yusoff

TL;DR
A woman with a history of allergies was misdiagnosed with Guillain-Barré syndrome but later found to have a rare autoimmune condition called EGPA, which responded well to steroid treatment.
Contribution
This case highlights the diagnostic challenge of distinguishing EGPA from GBS in patients with acute neuropathy.
Findings
Initial diagnosis of Guillain-Barré syndrome was incorrect; the patient was later diagnosed with EGPA.
The patient showed significant neurological improvement with corticosteroid therapy and methotrexate.
Systemic features like asthma, eosinophilia, and vasculitic signs are crucial for accurate diagnosis.
Abstract
A 41-year-old Malay woman with a background of allergic rhinitis, nasal polyps, and eczema presented with bilateral foot numbness and weakness. Neurological examination revealed bilateral foot drop and sensory loss over the L5-S1 dermatomes. Nerve conduction studies showed bilateral peroneal and tibial axonal neuropathy. She was initially diagnosed with Guillain-Barré syndrome (GBS) and treated with intravenous immunoglobulin (IVIG), but showed no clinical improvement. Further evaluation revealed pansinusitis on CT imaging, vasculitic rashes, marked eosinophilia of 8.7 × 10⁹/L, and positive p-ANCA (1:160), leading to a revised diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) with mononeuritis multiplex. She responded well to corticosteroid therapy and methotrexate, with significant neurological improvement and no relapse observed at follow-up. This case highlights the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3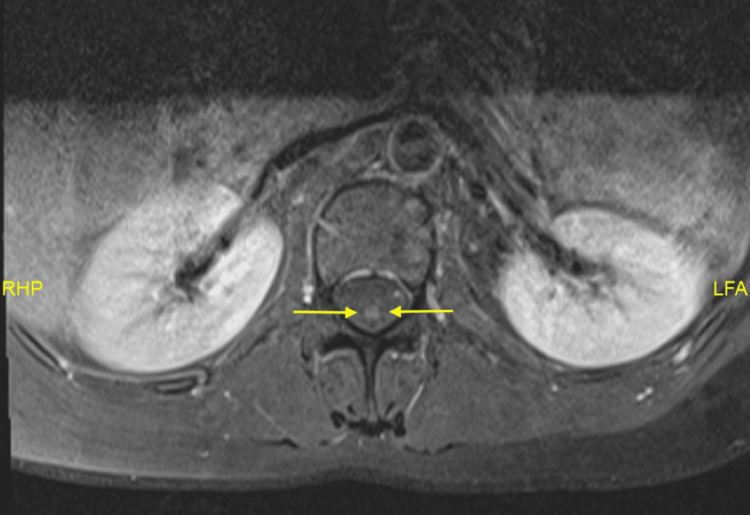 Figure 4
Figure 4| Nerve/Site | Latency (ms) | Amplitude | Conduction Velocity | Normal Amplitude (mV) | Normal Velocity (m/s) |
| Peroneal motor – right (popliteal segment) | 3.6 | 2.3 mV | 100 m/s | 2–6 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Peroneal motor – left (popliteal segment) | 4.2 | 1.1 mV | 59 m/s | 2–6 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Tibial motor – right (popliteal segment) | 12.6 | 0.1 mV | 42 m/s | 4–20 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Tibial motor – left (popliteal segment) | 11.9 | 0.2 mV | 51 m/s | 4–20 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Median motor – right | 3.2 | 13.0 mV | 63 m/s | 4–15 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Ulnar motor – right | 3.3 | 6.8 mV | 63 m/s | 6–12 mV | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Sural sensory – right | 2.1 | 14 µV | 61 m/s | ≥6 µV (sensory) | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Sural sensory – left | 1.9 | 8 µV | 68 m/s | ≥6 µV (sensory) | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Superficial peroneal sensory – R/L | — | 0 µV | — | ≥6 µV (sensory) | ≥50 m/s (approx for lower limb), ≥55 m/s (upper limb) |
| Parameter | Value | Reference Range |
| WBC | 18.99 × 10⁹/L | 3.8–10.6 × 10⁹/L |
| Neutrophils (absolute) | 7.9 × 10⁹/L | 1.80–7.70 × 10⁹/L |
| Lymphocytes (absolute) | 1.82 × 10⁹/L | 1.10–4.00 × 10⁹/L |
| Eosinophils (absolute) | 8.7 × 10⁹/L | 0.00–0.70 × 10⁹/L |
| ESR | 81 mm/hour | 0–10 mm/hour |
| CRP | 63.9 mg/L | < 5 mg/L |
| BUN | 3.1 mmol/L | 2.76-8.07 mmol/L |
| Creatinine | 43 μmol/L | 44-80 μmol/L |
| GFR (CKD-EPI) | 122 | |
| p-ANCA | Positive (1:160) | <1:20 |
| c-ANCA | Negative | <1:20 |
| Time | Key Events | Findings/Actions |
| Week 0 | Onset of symptoms | Bilateral foot numbness and progressive difficulty walking for two weeks |
| Week 2 (first admission) | Neurological findings | Bilateral foot drop (3/5), impaired dorsiflexion, eversion, inversion; sensory loss in L5–S1 dermatomes; diminished ankle reflexes; knee reflexes intact; steppage gait |
| Cutaneous and dermatologic findings | Maculopapular rashes on both lower limbs (Figures | |
| Imaging | CT brain: no intracranial abnormality; pansinusitis changes (Figure | |
| MRI lumbosacral spine | Bilateral symmetrical peripheral nerve root enhancement with patchy dural and central canal enhancement (Figure | |
| Nerve conduction study | Bilateral distal peroneal and tibial axonal neuropathy | |
| Working diagnosis and management | Guillain-Barré syndrome (GBS) diagnosed; treated with IVIG for 5 days → partial improvement → discharged | |
| Week 8 (readmission) | New neurological symptom | Sudden-onset numbness in the right hand (ulnar distribution) |
| Laboratory findings | Leukocytosis with marked eosinophilia (8.7 × 10⁹/L; 45.8%), positive p-ANCA (1:160), negative ANA, non-reactive hepatitis B/C | |
| Systemic features identified | History of bronchospasm and nebulizer use; CT showing pansinusitis | |
| Week 9 | Revised diagnosis | Eosinophilic granulomatosis with polyangiitis (EGPA) with mononeuritis multiplex confirmed based on systemic, hematologic, and neurologic findings |
| Week 9 onward (follow-up) | Treatment and response | High-dose prednisolone (tapered) and methotrexate 10 mg weekly → marked neurological improvement after 3 months: no relapse on follow-up |
| Feature | Eosinophilic Granulomatosis With Polyangiitis (EGPA) | Guillain-Barré Syndrome (GBS) |
| Clinical onset | Subacute onset over 2 weeks with progressive bilateral foot numbness and weakness | Usually acute, rapidly progressive (within days) ascending weakness |
| Symptom distribution | Asymmetric involvement (bilateral foot drop → later right hand numbness) consistent with mononeuritis multiplex | Symmetric ascending weakness and sensory loss |
| Reflexes | Diminished ankle reflexes with preserved knee reflexes | Global areflexia or hyporeflexia |
| Systemic features | Asthma, allergic rhinitis, nasal polyps, pansinusitis, and vasculitic rash on lower limbs | Typically absent; systemic involvement uncommon |
| Laboratory findings | Marked eosinophilia (8.7×10⁹/L, 45.8%), leukocytosis, positive p-ANCA (1:160) | Normal eosinophil count; may show mild albuminocytologic dissociation in CSF |
| Neurophysiology | Bilateral distal peroneal and tibial axonal neuropathy (asymmetric, motor-predominant) | Demyelinating or mixed axonal-demyelinating pattern, usually symmetric |
| Radiology (MRI/CT) | MRI lumbosacral spine: nerve root enhancement; CT sinuses: pansinusitis | MRI spine typically normal |
| Treatment response | Partial improvement after IVIG, but full response only after corticosteroids and methotrexate | Good response expected after IVIG or plasma exchange |
| Final diagnosis | EGPA with mononeuritis multiplex | GBS (initial working diagnosis) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Eosinophilic Disorders and Syndromes · Peripheral Neuropathies and Disorders
Introduction
Mononeuritis multiplex is a common neurological manifestation of eosinophilic granulomatosis with polyangiitis (EGPA), also known as Churg-Strauss syndrome [1]. Meanwhile, the peripheral nervous system involvement observed in Guillain-Barré Syndrome (GBS), characterised by mixed axonal and demyelinating neuropathy affecting both sensory and motor nerves, can overlap with the neuropathic manifestations seen in EGPA [2]. In clinical practice, patients who initially present with acute bilateral limb weakness and areflexia may be misdiagnosed as having GBS. However, the subsequent appearance of systemic features such as asthma, sinusitis, eosinophilia, or ANCA positivity should prompt reconsideration of EGPA as the underlying cause [2,3]. Differentiating between EGPA and GBS, therefore, requires a dynamic diagnostic approach that integrates neurological, haematological, and systemic findings.
Case presentation
We present the case of a 41-year-old Malay woman with a history of allergic rhinitis, nasal polyps, and chronic eczema. She presented with bilateral foot numbness and difficulty walking for two weeks. Neurological examination showed bilateral foot drop (3/5 strength) with impaired dorsiflexion, eversion, and inversion. Sensory loss was noted in the bilateral L5 and S1 dermatomes, and ankle reflexes were diminished, while knee reflexes remained intact. Gait analysis revealed a steppage gait. Further examination revealed maculopapular rashes on both lower limbs (Figures 1, 2). She was referred to dermatology for further evaluation, and the rashes were thought to represent vasculitis. A skin biopsy was planned, but the patient declined. A non-contrast CT scan of the brain showed no significant intracranial abnormalities. However, there was mixed iso-dense and hyperdense soft tissue material filling the ethmoid and bilateral maxillary sinuses (Figure 3), which may represent pansinusitis or chronic infection. An MRI of the lumbosacral spine revealed bilateral symmetrical peripheral nerve root enhancement, along with patchy enhancement of the dura and central canal (Figure 4). Nerve conduction studies indicated bilateral distal peroneal axonal neuropathy and tibial neuropathy (Table 1).
Vasculitic rashes on left lower limb (medially)
Vasculitis rashes on left lower limb (anteriorly)
Non-contrast computed tomography of the head shows mixed iso-dense and hyperdense soft tissue material filling up the ethmoid and bilateral maxillary sinuses (yellow arrow)
MRI lumbosacral with gadolinium (T1 sequence) shows enhancement of the central canal (yellow arrow)
A diagnosis of GBS was made, and the patient began a five-day course of intravenous immunoglobulin (IVIG). After completing the IVIG course, her symptoms showed partial improvement, and she was allowed to be discharged.
Six weeks later, she was readmitted, complaining of sudden-onset numbness in her right hand. Neurological examination revealed sensory loss in the ulnar area of the right hand. Further tests revealed a positive p-anti-neutrophil cytoplasmic antibody (p-ANCA) result with a titre of 1:160. The complete blood count showed leukocytosis with an eosinophil count of 8.7 × 10⁹/L (45.8%) (Table 2). Antinuclear antibody testing was negative, and viral screening for hepatitis B and C was non-reactive.
Upon further inquiry, she had a history of frequent nebuliser use in 2023 and 2024 due to bronchospasm. Given the presentation of mononeuritis multiplex, vasculitic rashes, allergic rhinitis with nasal polyps, asthma, hypereosinophilia, pansinusitis on CT, and positive p-ANCA, the final diagnosis was EGPA with mononeuritis multiplex. She was started on high-dose prednisolone with a tapering regimen. During follow-up at the rheumatology clinic, she was started on weekly methotrexate 10 mg. After three months, she showed marked neurological improvement, with resolution of sensory deficits and partial restoration of motor function. No signs of disease relapse were observed, and corticosteroids were successfully tapered (Table 3).
Discussion
EGPA and GBS are distinct disorders with overlapping clinical and pathological features, leading to diagnostic and therapeutic considerations. EGPA, formerly known as Churg-Strauss syndrome, is a systemic vasculitis characterised by eosinophil-rich granulomatous inflammation that affects multiple organs, most commonly the lungs, skin, and peripheral nerves [4]. In contrast, GBS is an acute, immune-mediated polyneuropathy characterised by progressive muscle weakness and sensory disturbances, often triggered by preceding infections, with subtypes including acute inflammatory demyelinating polyneuropathy and acute motor axonal neuropathy [5]. Both EGPA and GBS involve the peripheral nervous system, manifesting as neuropathy, which can lead to diagnostic challenges. Thus, differentiating between EGPA and GBS is crucial for appropriate management, as the treatment strategies differ significantly.
Although GBS was initially suspected based on the patient’s subacute weakness and bilateral sensorimotor involvement observed through the clinical, radiological, and neurophysiological tests, the evolving clinical picture suggested an alternative aetiology. The presence of multiplex mononeuritis, eosinophilia, positive p-ANCA, and systemic features, including asthma, sinusitis, and vasculitic rashes, strongly favoured EGPA-associated neuropathy over GBS.
Our patient initially presented with neurological symptoms mimicking GBS. However, persistent progression despite IVIG, eosinophilia, and p-ANCA positivity helped differentiate EGPA. This highlights the need for clinicians to consider ANCA vasculitis in GBS-like presentations, particularly in patients with allergic or eosinophilic histories.
The 2022 American College of Rheumatology and European Alliance of Associations for Rheumatology Classification Criteria for EGPA outline specific criteria for diagnosing EGPA, with each criterion assigned a particular weight. These include a maximum eosinophil count ≥1 × 10⁹/L (+5), obstructive airway disease (+3), nasal polyps (+3), cytoplasmic ANCA or anti-proteinase 3-ANCA positivity (-3), extravascular eosinophilic predominant inflammation (+2), mononeuritis multiplex or motor neuropathy not due to radiculopathy (+1), and haematuria (-1). After ruling out other conditions that mimic vasculitis, a patient with small- or medium-vessel vasculitis can be classified as having EGPA if their cumulative score is ≥6 points [6]. This system demonstrates high sensitivity (85%) and specificity (99%) for identifying EGPA patients. In our case, the patient scored 9 points, strongly indicating EGPA. While highly recommended, biopsies are not always practical and often yield non-specific findings [7]. If the peripheral nerves are involved and diagnostic ambiguity continues, a nerve biopsy might be an option. The nerve biopsy would show vasculitis, eosinophilic infiltration, and granuloma formation.
The mainstay of treatment for EGPA consists of corticosteroids and immunosuppressive drugs to control eosinophilic inflammation and vasculitis. On the other hand, GBS is usually treated with intravenous immunoglobulin or plasma exchange to eliminate or neutralise the harmful autoantibodies. While both conditions are immune-mediated, they involve different targets and pathways, requiring distinct treatment strategies. According to the 2022 EULAR recommendations, for induction of remission in patients with new or relapsing EGPA with organ- or life-threatening disease, a combination of glucocorticoids and either rituximab (RTX) or cyclophosphamide (CYC) is proposed. For non-organ- or non-life-threatening EGPA, glucocorticoids combined with RTX are recommended, with methotrexate (MTX) or mycophenolate mofetil (MMF) as alternative options to RTX. In our case, the patient was started on MTX [3].
The prognosis of EGPA-related neuropathy varies depending on the extent of nerve damage and the timing of treatment initiation. Studies indicate that with early diagnosis and appropriate immunosuppressive therapy, significant neurological recovery can be achieved in most patients [8]. However, delayed treatment or severe nerve involvement may lead to persistent deficits, including residual weakness, sensory loss, and chronic pain. In some cases, long-term immunosuppression is required to prevent disease relapse. A retrospective study on EGPA neuropathy found that up to 70% of patients showed partial or full recovery of nerve function after immunosuppressive therapy, although some required ongoing steroid-sparing agents such as methotrexate or azathioprine to maintain remission [1]. In contrast, GBS has a more predictable recovery pattern, with most patients regaining function within 6-12 months, although some experience residual fatigue, weakness, or autonomic dysfunction [9]. In this patient, the early introduction of corticosteroids and methotrexate led to neurological improvement, but long-term follow-up is essential to monitor for relapse, steroid dependence, or progression to systemic vasculitis.
This case highlights the importance of differentiating EGPA-associated neuropathy from GBS, given the differing pathophysiology and treatment approaches. The patient responded well to corticosteroids and methotrexate, emphasising the importance of early recognition and intervention to prevent long-term neurological sequelae (Table 4).
Conclusions
Mononeuritis multiplex is the most typical manifestation of vasculitic neuropathy in EGPA, but it can also resemble GBS, particularly when presenting with acute or subacute limb weakness. Nerve root enhancement on MRI may occur in both conditions; however, the asymmetric and patchy pattern often favours a vasculitic aetiology, whereas GBS more commonly demonstrates diffuse and symmetric enhancement. Although CSF analysis was not performed in this case, albuminocytologic dissociation would have supported GBS, while its absence would not exclude EGPA. Similarly, electromyography/nerve conduction velocity findings demonstrated axonal involvement of the peroneal and tibial nerves, which, although not specific, aligned more with mononeuritis multiplex than with the typical early demyelinating features expected in GBS. Clinical localisation of weak dorsiflexion, eversion, inversion, and sensory deficits in L5-S1 dermatomes further supported multifocal peripheral nerve involvement consistent with EGPA rather than the symmetric pattern classically seen in GBS.
The presence of systemic features such as asthma, sinus disease, eosinophilia, and vasculitic skin lesions should prompt reconsideration of EGPA, especially when there is poor or no response to IVIG. While partial recovery in demyelinating GBS may begin within the first month of treatment, full recovery usually evolves more slowly over 6-12 months, in contrast to the variable course of vasculitic neuropathy. Early recognition of these distinguishing clinical, electrophysiological, and imaging findings, together with prompt initiation of immunosuppressive therapy, is essential to prevent further neurological deterioration and improve functional outcomes. This case underscores the importance of a thorough clinical assessment and a multidisciplinary approach in atypical neuropathy presentations to ensure accurate diagnosis and timely management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical characteristics and treatment response of peripheral neuropathy in the presence of eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome): experience at a single tertiary center J Clin Neurol Cho HJ Yune S Seok JM 77831320172807931610.3988/jcn.2017.13.1.77PMC 5242145 · doi ↗ · pubmed ↗
- 2Eosinophilic granulomatosis with polyangiitis imitating Guillain-Barré syndrome: a case report Egypt J Neurol Psychiatry Neurosurg Khandelwal D Singh A Meena DS 173572021 https://link.springer.com/article/10.1186/s 41983-021-00411-3
- 3A rare case report of polyangiitis overlap syndrome: granulomatosis with polyangiitis and eosinophilic granulomatosis with polyangiitis BMC Pulm Med Quan MV Frankel SK Maleki-Fischbach M Tan LD 181182018 https://link.springer.com/article/10.1186/s 12890-018-0733-23049743810.1186/s 12890-018-0733-2PMC 6267840 · doi ↗ · pubmed ↗
- 4Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): state of the art Allergy Vaglio A Buzio C Zwerina J 2612736820132333081610.1111/all.12088 · doi ↗ · pubmed ↗
- 5Diagnosis and management of Guillain-Barré syndrome in ten steps Nat Rev Neurol Leonhard SE Mandarakas MR Gondim FAA 671683152019 https://www.nature.com/articles/s 41582-019-0250-93154121410.1038/s 41582-019-0250-9PMC 6821638 · doi ↗ · pubmed ↗
- 62022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis Arthritis Rheumatol Grayson PC Ponte C Suppiah R 3863927420223510696810.1002/art.41982 · doi ↗ · pubmed ↗
- 7EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update Ann Rheum Dis Hellmich B Sanchez-Alamo B Schirmer JH 30478320243692764210.1136/ard-2022-223764 · doi ↗ · pubmed ↗
- 8Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome)Stat Pearls [Internet] Chakraborty RK Aeddula NR Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 537099/