Health Promotion and Disease Prevention in Public Housing Areas: A Scoping Review
Iben Engelbrecht Giese, Signe Lykke Justsen, Vibeke Brinkmann Løite, Stine Hangaard

TL;DR
This review explores health interventions in public housing to reduce health disparities, emphasizing community involvement and underused digital tools.
Contribution
The study provides a synthesized overview of health promotion interventions in public housing, highlighting community engagement and digital health gaps.
Findings
31 articles were identified covering eight intervention categories in public housing areas.
Digital health components were present in only five of the included studies.
Interventions with strong community engagement showed positive health outcomes.
Abstract
Residing in public housing is associated with adverse health outcomes, partly due to higher prevalence of unhealthy lifestyle behaviors linked to lower socioeconomic status. Health promotion and disease prevention interventions can mitigate these disparities but are often underutilized due to accessibility barriers and low health literacy. Delivering interventions directly within public housing areas may enhance reach and effectiveness. However, synthesized knowledge of such interventions remains limited. This scoping review aimed to identify and summarize available evidence on health-promoting and disease-preventive interventions in these settings. The review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRIMA-ScR) guidelines. A systematic search was performed in PubMed, CINAHL, Embase, and Scopus. Articles were screened…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
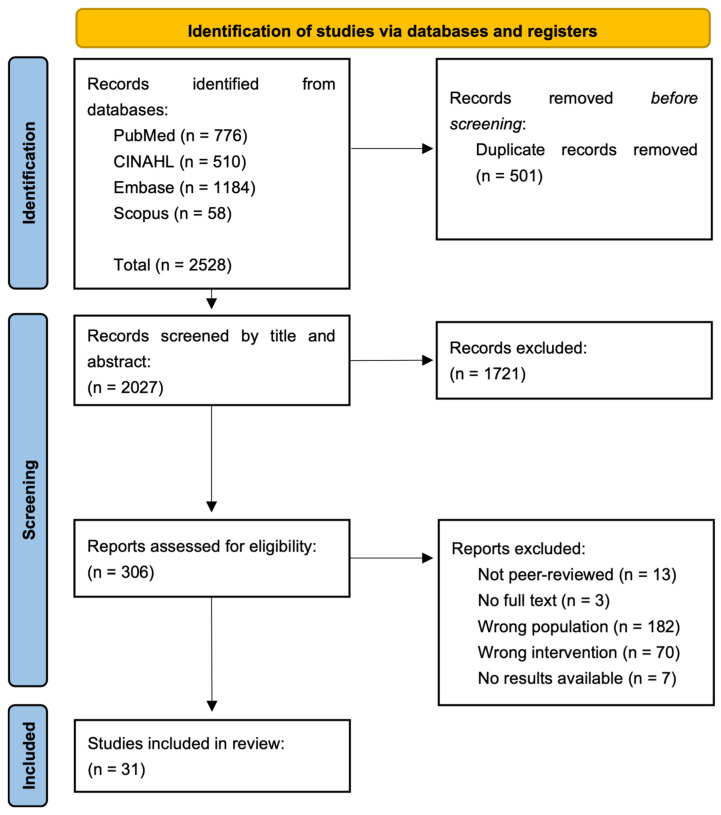 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth disparities and outcomes · Food Security and Health in Diverse Populations · Smoking Behavior and Cessation
1. Introduction
Residing in a public housing area is associated with adverse health outcomes [1]. The concept of public housing varies internationally and encompasses different governance models. In many contexts, public housing is not only provided directly by government authorities but also by non-profit housing organizations that operate to deliver affordable housing to low-income populations [2,3,4]. Non-profit-administered housing is often characterized by long-term tenancy, relatively stable resident populations, and a focus on community-oriented management [2,4]. Given these features, and to ensure a more consistent contextual basis, the present review defined public housing as affordable housing accessible to all individuals, primarily administered by non-profit organizations [3]. Public housing is primarily inhabited by individuals with lower socioeconomic status (SES), who often experience significantly adverse health outcomes compared to those with higher SES [5]. This health disparity is evidenced by an increased prevalence of chronic diseases, such as cardiovascular disease and type 2 diabetes, adverse mental health, obesity, and elevated mortality rates [6,7,8]. These disparities can be explained by the fact that individuals with a lower SES often exhibit a higher prevalence of unhealthy lifestyle behaviors, including smoking, physical inactivity, and poor dietary patterns [1,9,10,11,12,13,14]. Hence, addressing these health disparities requires targeted interventions regarding lifestyle behavior that consider the challenges faced by public housing residents.
Health promotion and disease prevention constitute essential intervention strategies for addressing these issues. Such interventions can reduce the risk of developing new health conditions, prevent the worsening of existing chronic diseases, and enhance individuals’ self-efficacy in managing their own health [15,16,17,18,19,20]. However, the utilization of such promotive and preventive healthcare interventions by residents in public housing areas is often hindered by multiple accessibility barriers. These barriers include significant geographical distances to healthcare services, which are typically located in health centers or similar facilities far from public housing areas [21,22]. In addition, the surrounding environment may lack walkability and perceived safety, making it difficult or unsafe for residents to engage in physical activity or to travel to these services on foot [21,22,23]. Limited public transportation options and time-consuming travel further restrict access [21,22]. Moreover, residents in public housing areas frequently experience limited health literacy, which may affect their understanding of both the importance and the content of health promotion and disease prevention initiatives [24,25]. This limited health literacy can lead to a lack of awareness and comprehension of available healthcare services and how to utilize them effectively [21,24,26]. Consequently, bringing health promotion and disease prevention initiatives closer to public housing areas may enhance accessibility and safety, and ensure that the interventions are more effective and widely utilized.
Despite the importance of health promotion and disease prevention interventions in public housing areas, there is a notable gap in the literature regarding the specific strategies that have been implemented in these settings. To the best of the authors’ knowledge, no literature review has been conducted to gather and synthesize the experiences from such interventions. Therefore, this scoping review seeks to identify and map the available evidence on health promotion and disease prevention interventions in public housing areas. It aims to address the research question: What health-promoting and disease-preventive interventions are identified in public housing areas? Additionally, digital components applied in the interventions will be identified and mapped, as digitalization has had a major impact in health promotion and preventive interventions, demonstrating great potential for increasing health outcomes and ensuring proximity of the interventions [27,28,29,30,31]. However, factors such as poverty, limited digital access and low literacy in public housing areas may affect the feasibility of these components, which makes it important not only to identify them but also to assess their effect [32].
2. Materials and Methods
The current scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines [33] (Supplementary Material S1). This scoping review was conducted without a preregistered protocol.
2.1. Inclusion and Exclusion Criteria
Original peer-reviewed articles that described completed health-promoting and disease-preventive interventions in public housing areas were included. Public housing was understood as non-profit administered, affordable housing, and studies conducted in temporary or exclusively government-owned housing models were excluded. The results of the interventions needed to be presented in the articles to be included. Full-text articles published between 1 January 2004 and 18 September 2024 were considered for inclusion. Articles written in English or any of the Scandinavian languages were accepted. Articles describing interventions in public housing areas exclusively government owned or reserved for specific social groups were excluded to ensure homogeneous contexts. Additionally, articles describing interventions focusing on environment or interior in relation to health promotion were excluded as the review focused solely on interventions targeting the individual. If an article reported on multiple interventions, it was included only if the results for environmental and individual-based interventions were presented separately.
2.2. Search Strategy
Initially, a non-systematic search was performed in PubMed, Embase, and Google Scholar to identify relevant search terms, keywords, and index terms to incorporate in the systematic search. Following this, the systematic literature search was performed in four relevant databases: PubMed, CINAHL, Embase, and Scopus on the 18th of September 2024. The search strategy involved a block search comprising two main blocks, using the overall search terms “Public Housing” and “Health-promoting or preventive interventions,” respectively. To broaden the search, we incorporated synonyms for the primary search term, utilizing a combination of MeSH terms and relevant keywords. An experienced research librarian was consulted to validate the search strategy. One review author (SLJ) performed the searches in the databases. For full-electronic search strategy, see Supplementary Material S2.
2.3. The Screening Process
First, all articles identified through the systematic search were collected and uploaded into RefWorks 2024, where duplicates were removed. Second, all remaining articles were screened by title and abstract by one review author (SLJ) to assess their eligibility based on the inclusion criteria. In case of uncertainty regarding the relevance of an article, another review author (IEG) was consulted. Third, the remaining articles were assessed for full-text screening (SLJ, IEG). During the full-text screening, reasons for exclusion of articles were registered and presented in a PRISMA flow diagram. Any disagreement between the review authors during the screening process was resolved through discussion or by involving a third author (SH).
2.4. Data Extraction and Synthesis
All articles included following full-text screening were read profoundly by one review author (IEG). The table function in Microsoft Word 2024 was utilized to extract data from each included article, following a predefined table format that was agreed upon by three of the review authors (SLJ, IEG, SH). The following article details were extracted: Author, year, population, type of housing, aim of intervention, description of the intervention, digital component (if any), and key findings. In case of uncertainty regarding article details, another review author (SLJ) was consulted. Any disagreement was resolved through discussion or by involving a third reviewer (SH).
Extracted details from the articles were utilized to synthesize categories based on the type of health-promoting or disease-preventive intervention by review author IEG. An article could be included under multiple categories if the intervention contained various aspects relevant to different categories. Separate tables based on the identified categories were created, and the content of each category was summarized. One review author, SH, validated the synthesis of categories. Furthermore, a separate table was created to summarize the articles in which a digital component was identified. This table provided descriptions of the digital elements involved in the interventions.
2.5. Ethics Approval
As the review used publicly available data from previously published studies, ethical approval was not required.
3. Results
3.1. Screening and Search Outcomes
A total of 2528 articles were identified in the systematic search, of which 501 were duplicates. After removing the duplicates, the remaining 2027 articles underwent screening on title and abstract, where 1721 articles were excluded due to irrelevance. Subsequently, 306 articles underwent full-text screening, where 275 articles were excluded, mainly because they focused on a wrong population (n = 182) or did not contain a health promotion or disease-preventive intervention (n = 70). After full-text screening, 31 articles were included in the current review. Figure 1 illustrates the full screening process.
3.2. Study Characteristics
The characteristics of the included articles are presented in Supplementary Material S3. The included articles were published between 2004 and 2024, of which the majority (n = 25) were carried out in USA (80.6%), two in Denmark (6.5%), two in Canada (6.5%), one in China (3.2%), and one in Australia (3.2%). Five articles (16.1%) included a digital intervention component. A mixed-methods approach was applied in eight (26%) of the included articles. Seven articles (23%) employed a pre-post-test design, and seven (23%) used a qualitative design. A cluster randomized trial design was applied in four articles (13%), while three (10%) articles used a feasibility study design. The remaining two articles employed a non-randomized pilot study design (3%) and a randomized controlled trial design (3%), respectively.
3.3. Synthesized Findings
The interventions described in the included 31 articles revealed eight different categories including: (1) Health promoter programs, (2) Nutrition programs, (3) Health screenings, (4) Health promotion messages, (5) Physical activity programs, (6) Mental health programs, (7) Oral health programs, and (8) Other health interventions. Eight articles were included in more than one category.
3.3.1. Health Promoter Programs
Health promoter programs (Table 1) included training residents to become community health advocates. In many cases, residents applied to participate in the health promoter programs [34,35,36,37,38,39,40,41,42], and they often reflected the broader resident population by having the same linguistic and cultural background [36,37,38,40]. The training content commonly included, leadership skills, needs assessments, health promotion activities (e.g., exercise, nutrition, mental health, health screenings, smoking cessation, and navigating healthcare services), self-management theories, and chronic disease education such as diabetes, hypertension, and asthma [34,35,36,37,38,39,40,41,42]. Following training, four studies reported that health advocates conducted needs assessments among residents and implemented health promotion activities based on identified priorities [34,35,37,41]. The health advocates were generally responsible for organizing activities, recruiting participants, and facilitating implementation [34,35,36,37,38,39,40,41,42]. The duration of training ranged from 30 to 56 h, and the subsequent community-based activities lasted from four weeks to two years. Several studies reported that the involvement of community health advocates contributed to increased community engagement, enhanced understanding of health promotion and disease prevention, improved trust, and better access to health services [34,35,36,37,39,41]. Community activities were often successfully implemented due to the engagement and leadership of the community health advocates [34,35,36,37,41]. Only one study reported challenges, primarily related to insufficient training and unclear role definitions for the health advocates [42]. Five of the nine studies reported positive health-related changes, such as reduction in blood glucose, blood pressure and weight, improvements in oral hygiene, and increases mental health [36,38,39,40,41].
3.3.2. Nutrition Programs
Nutrition programs (Table 2) included nutrition education, food-related skill development, interactive gardening, hands-on gardening and cooking, cooking demonstrations, easy access to fruits and vegetables, participatory theater show about making healthy choices, motivational interviewing counseling, cookbooks with healthy recipes, health promotion messages, weight management strategies, and strategies for eating healthy on a budget [35,43,44,45,46,47,48,49,50,51,52]. The frequency of the interventions varied from once a week to twice a week and lasted up to one year. One study included a “booster” session at the end of the program [49]. Several studies reported an increase in the average servings of fruits and vegetables [35,44,45,48], while only one study found no change [49]. Three studies reported an overall decrease in average total caloric intake, consumption of sugar-sweetened beverages and foods, and frequency of fast-food consumption [35,47,49]. Across many studies, participants experienced increased knowledge of gardening and healthy eating and willingness to try fruits and vegetables [44,46,47,52]. One study reported that the program improved social connections and reduced exposure to gangs and drugs [50].
3.3.3. Health Screenings
Health screenings (Table 3) contained life-style questionnaires, screening for psychosocial service needs, and physical examinations measuring, for example, blood pressure, glycated hemoglobin A1c, weight, height, waist circumference, and fitness level [35,40,43,53,54,55]. The screenings were offered to identify health risks such as diabetes [35,40,43,53,54,55]. The screening results were often shared with the participants through a dialogue with the health screener [35,40,43,53,55]. Those at risk were advised to consult a general practitioner or referred to relevant health programs [35,53,55]. Health screenings were primarily held at community centers [35,40,43,53,54] and offered approximately once or twice a week for a maximum of one year. In two studies, residents perceived the health screenings as valuable [53,55], whereas one study noted a lack of meaningful support and follow-up from healthcare professionals [55]. Several studies found decreases in BMI, healthier life-style behaviors, and improvements in mental well-being [35,40,43,53]. One study reported that high attendance at the screenings was linked to active community leaders [54].
3.3.4. Health Promotion Messages
Health promotion messages (Table 4) focused on HPV vaccination, cervical cancer screening, and sugar-sweetened beverages and foods [51,56]. The messages had an educational purpose targeting self-efficacy and motivation, and included photos, web-links, advice, and factual information [51,56]. One study delivered the messages through Twitter [56], while the other used SMS and other social media platforms [51]. The messages were delivered once a day or every other day for one month. Most participants perceived the health promotion messages as a suitable educational strategy [51,56], but no significant impact on the participants’ health behaviors or intentions were reported [56]. One study reported that messages targeting motivation were rated lowest in terms of satisfaction [51].
3.3.5. Physical Activity Programs
Physical activity programs (Table 5) included walking groups, women-only exercise activities, gentle exercise programs, workshop sessions focusing on exercise and its benefits, and physical activities delivered through fun and entertaining formats [35,47,48,50,52,53,57,58]. One program used prizes and acknowledgements to motivate the participants [57]. The frequency of the interventions varied from five times a week to one session per month. Some studies reported high participant satisfaction with the physical activities and workshop content [47,50,52,53]. Programs that included walking groups were associated with significant increases in minutes walked per day and enhanced social connections among neighbors [35,57]. Additionally, two studies focusing on adolescent girls found increases in physical activity levels [48,59]. One study reported that women-only exercise had high attendance, and participants appreciated the opportunity to join activities where they felt safe, which provided personal time and social opportunities [58].
3.3.6. Mental Health Programs
Mental health programs (Table 6) were delivered through group sessions or open workshops that focused on specific themes such as aging, depression, social isolation, men’s health, social support, and health topics like diabetes [53,60]. The frequency of sessions ranged from weekly to once every six to eight weeks. Participants in these studies generally perceived the programs as effective, reporting improved social interactions, and increased mental well-being [53,60].
3.3.7. Oral Health Programs
Oral health programs (Table 7) included motivational interviewing, which were used to analyze the participants situation and develop plans for oral hygiene, combined with practical training in tooth brushing and flossing techniques [61,62]. Moreover, one program also included health fairs with practical oral hygiene activities, question sessions, and campaign messages on oral hygiene to reinforce the motivational interviewing [61]. The interventions lasted six months. Participants in both studies demonstrated significant improvements in oral hygiene (plaque scores, Gingival index, and brushing/flossing skills) and improvements in Oral Health-related Quality of Life [61,62].
3.3.8. Other Health Interventions
The category other health interventions (Table 8) included a smoking cessation program [40], a sexual health program [63], and a social-enhancing activity [64].
The smoking cessation program included a weekly supply of nicotine replacement therapy and personal behavioral counseling [40]. It was held in the local community center. The intervention lasted four weeks. About 30.7% of the participants achieved cessation, but no significant change in exhaled carbon monoxide levels among the participants was reported [40].
The sexual health program included educational workshops supplemented with written material focusing on sexually transmitted infections, safe sex behaviors and symptoms, combined with few practical demonstrations and role-playing scenarios [63]. It was held at the community centres and lasted 30 to 45 min each time. Participants were satisfied with the sexual health program and expressed and demonstrated new skills and increased confidence [63].
Social-enhancing activities such as bus trips, guided tours, and lunch were organized for residents [64]. These activities were held two times over a four-month period. Participants expressed enhanced social interaction, which fostered a sense of community [64]. However, linguistic and cultural differences posed a significant challenge [64].
3.3.9. Digital Components
Five of the included articles utilized digital components as part of their interventions (Table 9). Velez et al. and Allen et al. provided health promotion information and advice via SMS or social media, while Schwinn et al. delivered an internet-based health promotion program [48,51,56]. Deville-Stoetzel et al. used automatically generated reminder messages to inform residents about health promotion workshops, whereas Ahluwalia et al. conducted motivational interviews with included residents over the phone and used educational videos about fruits and vegetables [44,54]. None of articles reported results directly related to the effect of using a digital component.
4. Discussion
The current scoping review aimed to identify and map the available evidence regarding health-promoting and disease-preventive interventions in public housing areas. The interventions were categorized into eight themes, with the most covered theme being nutrition education (36%), followed by health promoter program (30%) and physical activities (26%).
Nine of the included articles involved training residents to become health promoters in their own public housing area [34,35,36,37,38,39,40,41,42]. This involvement of residents in developing and implementing health promotion and disease-preventive interventions could be crucial for their success. A review by Cyril et al. explored the level of community engagement and health outcomes in health promotion interventions in urban areas. They found that a high level of community engagement was associated with positive health outcomes compared to interventions with low community engagement [65]. This finding is supported by several reviews, which found health promoters to be effective in health promotion in different settings [66,67,68]. The findings suggest that empowering residents to take an active role in health promotion within their communities can lead to more effective and sustainable interventions. Additionally, training residents as health promoters could be a cost-effective way to extend the reach of health interventions, particularly in resource-limited settings [69].
Only five (16%) of the included studies incorporated a digital component, and none of them reported outcomes directly related to the digital element. Although studies in other settings have shown promising effects on health outcomes related to health promotion and disease prevention when digital components are included [27,28,29,30,31], their use within public housing remains limited and insufficiently evaluated, indicating a need for greater scientific focus within this area. Digital health interventions may offer flexibility and potential to tailor content to residents’ needs and circumstances [70], which could be beneficial in public housing areas, where health needs and access to resources vary [5,21]. However, their implementation may be challenged by factors such as limited access to devices and low digital literacy [21,26]. Therefore, applicability of digital components in this context should be approached with caution, and future research is needed to determine under which conditions, and for whom, digital interventions can be both feasible and effective.
A significant number of studies within this scoping review reported the effects of their interventions through narrative or qualitative syntheses rather than quantifiable measures. While this may limit the ability to directly compare outcomes across studies [71], narrative syntheses and qualitative approaches are valuable within health promotion research because they can capture nuance and contextual complexity that quantitative measures may overlook [72,73]. However, the diversity in reporting formats and methodological approaches poses challenges for consistency, reproducibility, and generalizability of findings [71]. This suggests that the current evidence base may not yet be fully mature and highlights the need for methodological approaches that better integrate both qualitative and quantitative data to enable more comprehensive and comparable assessments of intervention effects.
The current scoping review has several limitations. One significant limitation is the variability in the definition of public housing across different countries. Public housing, also referred to as social housing, is subject to diverse interpretations and implementations depending on national policies, economic conditions, and cultural contexts. To minimize variability, public housing was defined as affordable housing accessible to all individuals and not exclusively government-owned. However, as this is a scoping review, the emphasis on homogeneity may have inadvertently constrained the breadth of the evidence base, thereby challenging the exploratory nature of the scoping methodology [74]. Thus, our findings may not be fully transferable to settings with different governance structures, such as entirely government-owned housing (e.g., the USA, England, and Canada) [75,76]. Future research should compare interventions across different public housing models to capture the full diversity of contexts in which health promotion interventions are implemented. Another limitation is that this review focused only on individually oriented interventions. This has excluded environmental or policy-level strategies, which are known to be highly effective in health promotion [77,78]. Future research should therefore examine multiple levels of intervention to capture the full scope of health promotion efforts in public housing contexts.
5. Conclusions
The current scoping review identified a range of health-promoting and disease prevention interventions in public housing areas, with nutrition education, health promoter programs, and physical activity being the most common. Notably, resident involvement through training as health promoters emerged as a key strategy, supporting evidence that community engagement enhances intervention effectiveness and sustainability. These findings highlight the importance of empowering residents to take active roles in shaping health initiatives within their communities. Despite the growing relevance of digital health, digital components were rarely incorporated and insufficiently evaluated, indicating a need for cautious consideration and further research to determine their feasibility in contexts characterized by limited access and digital literacy. Qualitative and narrative approaches offer valuable contextual insight, but the diversity of methods and reporting formats limits consistency and comparability across studies. Future research should examine different models of public housing and apply multi-level strategies—combining individual, environmental, policy-level, and potentially digital approaches—to strengthen the evidence base and support scalable health promotion interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pickett K.E. Multilevel Analyses of Neighbourhood Socioeconomic Context and Health Outcomes: A Critical Review J. Epidemiol. Community Health 20015511112210.1136/jech.55.2.11111154250 PMC 1731829 · doi ↗ · pubmed ↗
- 2Whitehead C.M.E. Social Housing in Europe School of Economics and Political Science London, UK 2007978-0-85328-100-9
- 3Nielsen R. Haagerup C. The Danish Social Housing Sector: Recent Changes and Future Challenges Crit. Hous. Anal.2017414214910.13060/23362839.2017.4.1.333 · doi ↗
- 4The Housing Europe Observatory The State of Social Housing in Europe 2023 Available online: https://www.housingeurope.eu/the-state-of-the-housing-in-europe-2023/(accessed on 12 June 2024)
- 5Barakat C. Konstantinidis T. A Review of the Relationship between Socioeconomic Status Change and Health Int. J. Environ. Res. Public Health 202320624910.3390/ijerph 2013624937444097 PMC 10341459 · doi ↗ · pubmed ↗
- 6Kivimäki M. Batty G.D. Pentti J. Shipley M.J. SipiläP.N. Nyberg S.T. Suominen S.B. Oksanen T. Stenholm S. Virtanen M. Association between Socioeconomic Status and the Development of Mental and Physical Health Conditions in Adulthood: A Multi-Cohort Study Lancet Public Health 20205 e 140e 14910.1016/S 2468-2667(19)30248-832007134 · doi ↗ · pubmed ↗
- 7Agardh E. Allebeck P. Hallqvist J. Moradi T. Sidorchuk A. Type 2 Diabetes Incidence and Socio-Economic Position: A Systematic Review and Meta-Analysis Int. J. Epidemiol.20114080481810.1093/ije/dyr 02921335614 · doi ↗ · pubmed ↗
- 8Stringhini S. Carmeli C. Jokela M. Avendaño M. Muennig P. Guida F. Ricceri F. d’Errico A. Barros H. Bochud M. Socioeconomic Status and the 25 × 25 Risk Factors as Determinants of Premature Mortality: A Multicohort Study and Meta-Analysis of 1·7 Million Men and Women Lancet 20173891229123710.1016/S 0140-6736(16)32380-728159391 PMC 5368415 · doi ↗ · pubmed ↗