Constructing Directed Acyclic Graphs (DAGs) to Inform Tobacco Cessation Intervention Research: A Methodological Extension Using Evidence Synthesis
Sanchita Sultana, Naiya Patel, Joseph Inungu

TL;DR
This study uses a new method to map out factors affecting tobacco cessation, showing how social and healthcare factors influence success in quitting smoking.
Contribution
The study introduces the ESC-DAG protocol to synthesize evidence into a causal framework for tobacco cessation interventions.
Findings
Structural factors like socioeconomic disadvantage and digital inequities strongly influence tobacco cessation outcomes.
Healthcare system factors such as provider engagement and outreach are key facilitators of successful cessation.
Digital access and culturally tailored interventions are underexplored but promising areas for improving cessation outcomes.
Abstract
Background: Tobacco use remains a leading preventable cause of morbidity and mortality in the United States, with persistent disparities in cessation outcomes across socioeconomic and racial groups. While numerous interventions exist, their effectiveness is shaped by complex interrelated factors at individual, social, and healthcare system levels. Identifying and modeling these causal pathways is essential to inform equitable intervention design. Methods: This study applied the Evidence Synthesis for Constructing Directed Acyclic Graphs (ESC-DAG) protocol to integrate empirical findings from 35 quantitative studies examining barriers and facilitators of tobacco cessation intervention uptake in the United States. Using the Andersen and Aday Health Services Research Model as a guiding framework, we extracted, harmonized, and synthesized significant causal relationships into a unified DAG,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
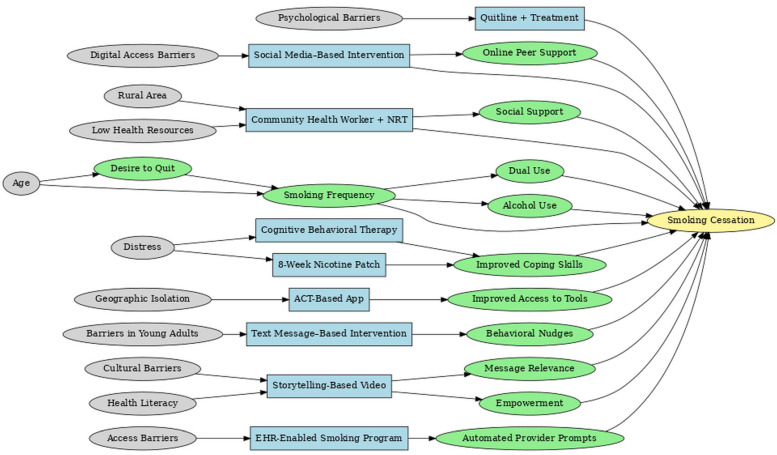 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4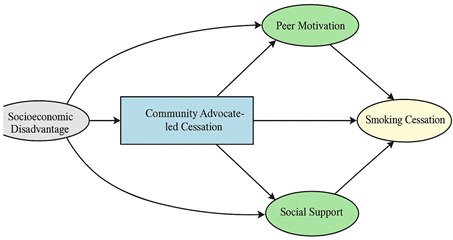 Figure 5
Figure 5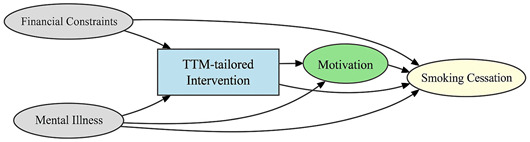 Figure 6
Figure 6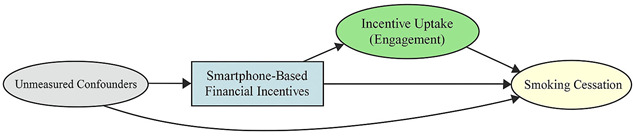 Figure 7
Figure 7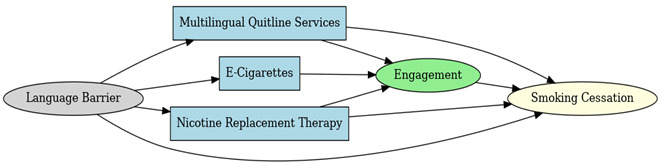 Figure 8
Figure 8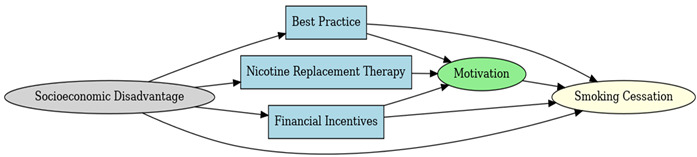 Figure 9
Figure 9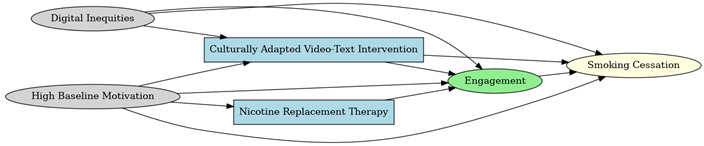 Figure 10
Figure 10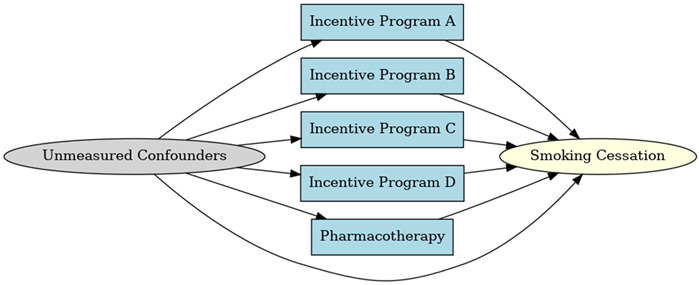 Figure 11
Figure 11 Figure 12
Figure 12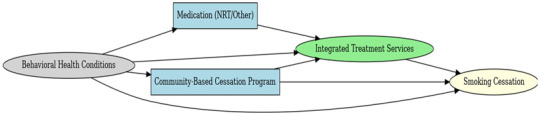 Figure 13
Figure 13 Figure 14
Figure 14 Figure 15
Figure 15 Figure 16
Figure 16 Figure 17
Figure 17 Figure 18
Figure 18 Figure 19
Figure 19 Figure 20
Figure 20 Figure 21
Figure 21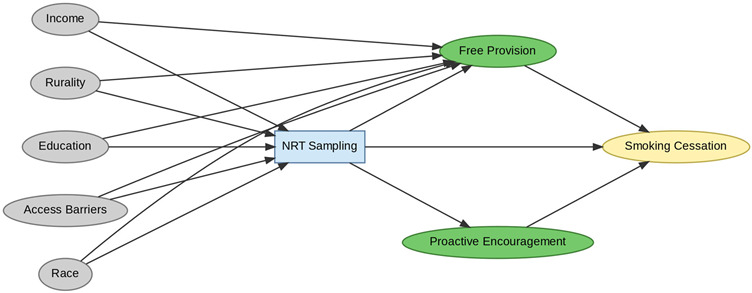 Figure 22
Figure 22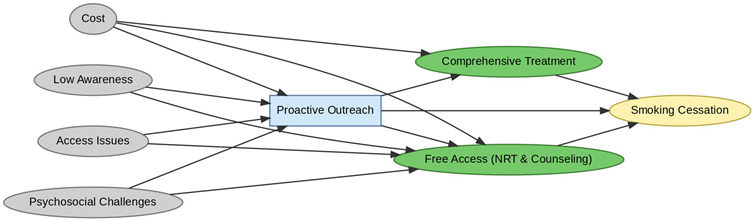 Figure 23
Figure 23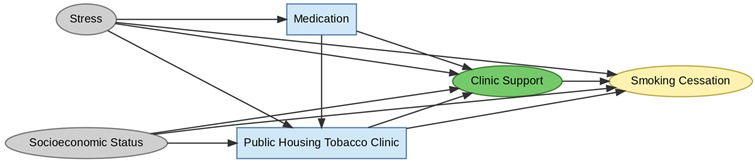 Figure 24
Figure 24 Figure 25
Figure 25 Figure 26
Figure 26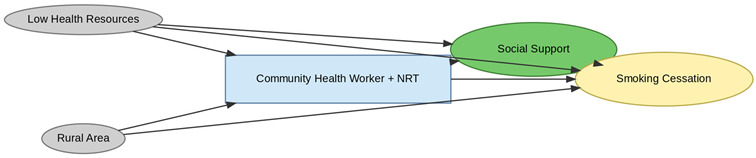 Figure 27
Figure 27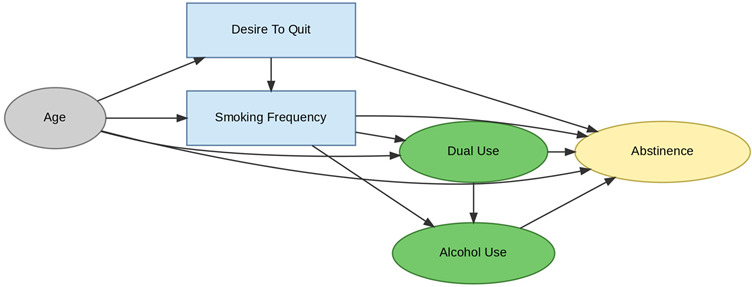 Figure 28
Figure 28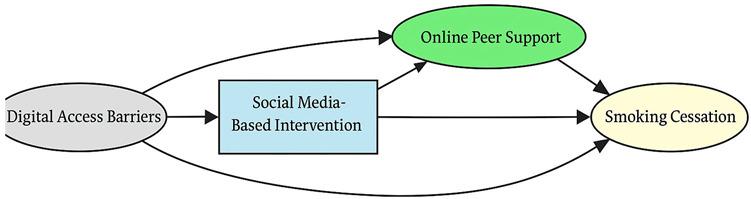 Figure 29
Figure 29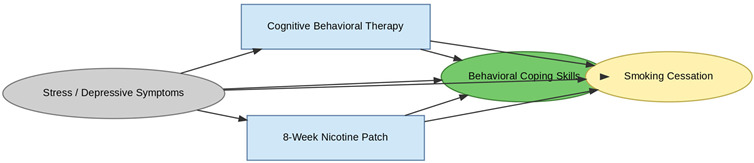 Figure 30
Figure 30 Figure 31
Figure 31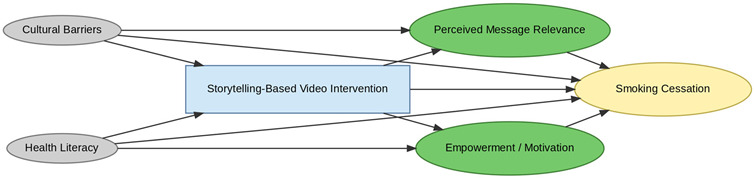 Figure 32
Figure 32 Figure 33
Figure 33 Figure 34
Figure 34Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Causal Inference Techniques · Bayesian Modeling and Causal Inference · Statistical Methods and Bayesian Inference
1. Introduction
Smoking is one of the leading preventable causes of premature death and health inequities in the United States. According to a study conducted in the U.S. from 2014 to 2019 using U.S. population data, a persistent sociodemographic inequality was identified. Although a similar or higher quit interest exists among non-White and lower socioeconomic status groups, significantly lower sustained cessation rates, i.e., only about 7.5% were observed. The tobacco cessation treatment uptake remained low, i.e., 34% and the disparities in treatment receipt did not improve significantly [1]. The NHIS data examination reported similar underlying trends in disparities in receiving professional cessation advice. Those who are older adults, reside in urban areas, have access to primary care, and are diagnosed with COPD were highly likely to receive tobacco cessation treatment assistance, disproportionately affecting rural, younger, uninsured, and racial minority smokers [2,3].
As per a recent CDC MMWR report, about 50% of adult smokers among 28.8 million U.S. adult smokers tried to quit, but only about 10% succeeded, and less than 40% utilized tobacco cessation interventions, i.e., medical or non-medical interventions [4]. Lower access to tobacco cessation interventions and lower sustained quitting are associated with lower socio-economic status and rural residence. Although the cessation intervention exists, access to pharmacotherapy, counselling, or other types of cessation interventions remains limited due to unaligned care coordination, cost, or lower healthcare engagement [2,3,5]. Prior work has identified key barriers and facilitators of cessation intervention utilization in the United States at both the population and healthcare system levels. The key barriers identified across diverse cessation intervention types are digital inequities for digital interventions, socioeconomic disadvantage, and low motivation at the population level. At the healthcare system level, barriers to care access and inadequate healthcare provider engagement have been identified as further system-level barriers in effective tobacco cessation intervention utilization in the U.S., while the key facilitators identified are financial incentives, culturally tailored interventions, and digital engagement strategies [6].
The effectiveness of treatment interventions outside a strict clinical trial environment is affected by several confounding barriers and facilitating factors [7]. It is crucial to identify such factors to develop a Directed Acyclic Graph (DAG), a visual representation of complex relationships between key factors affecting the exposure and outcome variables relationship in any observational data study, as it informs the statistical modeling for causal inferences [6,7,8]. A conventional statistical model due to parametric assumptions might not capture the comprehensive causal relationship of a study context; however, a DAG can graphically depict the complex causal relationship between a key exposure and outcome factors. According to PubMed, Embase, Web of Science, and Google searches, there exists no scientific literature that develops evidence-based DAG on factors affecting tobacco cessation intervention utilization in the United States. As established, it is vital to build such DAGs to identify causal relationships that affect the tobacco cessation intervention utilization to improve the health inequities and smoking prevalence rate in the United States. Although evidence-based cessation intervention exists, there is a need to identify measurable factors that affect the causal relationship between socioeconomic factors and cessation or quit outcomes in the presence of key confounders. Hence, this study builds upon a prior systematic review to develop an evidence synthesis DAG [6].
2. Materials and Methods
2.1. Study Design and Evidence Base
This study utilized the Evidence Synthesis for Constructing Directed Acyclic Graphs (ESC-DAG) protocol to identify the causal factors affecting tobacco cessation intervention uptake in the United States. In observational research, the ESC-DAG methodology helps to integrate causal relationships from existing empirical evidence [9].
A total of 35 studies were identified in the prior extension of this work, a systematic review [6] about barriers and facilitators to tobacco cessation interventions at the population and healthcare system levels. The study included randomized control trials, quasi-experimental, and observational quantitative studies that examined determinants of smoking cessation intervention uptake and treatment disparities at both the population and healthcare system level.
Although ESC-DAG methodology typically integrates multiple evidence sources, this study used a prior systematic review that synthesized 35 quantitative studies examining barriers and facilitators of tobacco cessation intervention uptake in the United States. Given the methodological rigor, comprehensive scope, and quality appraisal within that review, it served as a consolidated and sufficient evidence base for DAG construction consistent with established ESC-DAG applications.
2.2. ESC-DAG Protocol Application
The mapping stage included edge identification and coding in DAGitty software (v 3.1) [10]. Each study included was reviewed to extract empirically supported causal relationships/arrows (interchangeably used with terminology edges) between exposure and outcome variables. Edges that were statistically significant between exposure and outcome variables and coded within the original study context were extracted verbatim. The direct and indirect pathways were established without any directionality rules implied to preserve the original study context.
The translation stage included thematic grouping and categorization by imposing ESC-DAG protocol directionality rules. The conceptual framework used to determine the temporality and directionality of constructs was frequently the Andersen and Aday Health Services Research framework [11]. Overlapping constructs, such as digital access and digital inequities, were combined into a single standardized category. The bidirectionality was assessed, and constructs were aligned with theoretical determinants from the conceptual framework.
The integration stage involved synthesis into a final compiled ESC-DAG. The harmonized constructs and their edges were synthesized into a single DAG that included confounders, mediators, and potentially other effect modifiers. Two reviewers (N.P. and S.S.) independently conducted edge extraction from each included study, identifying statistically supported directional relationships (edges) between constructs. The third reviewer (J.I.) synthesized the independent extraction files and conducted a consensus reconciliation. All reviewers jointly applied thematic grouping and temporal alignment following the Andersen and Aday Health Services Research Model. N.P. implemented the final harmonized Directed Acyclic Graph (DAG) using DAGitty software, and all three reviewers validated node placement and directionality through iterative review.
2.3. Conceptual Framework and Quality Assurance
The Andersen and Aday Health Services Research Model was utilized as an organizing framework to contextualize constructs across predisposing, enabling, and need-based factors. The protocol recognized the need for a conceptual framework to inform its translation stage, ensuring that the DAG represented statistical associations aligned with established theory on healthcare access and utilization.
3. Results
3.1. Mapping Stage Findings
A total of 35 included studies identified a wide range of causal pathways that linked individual, social, and structural factors to smoking cessation outcomes (Table 1). Each study contributed multiple causal pathways, i.e., edges establishing several potential pathways. Frequently mapped factors included socioeconomic disadvantage, digital access and literacy, motivation to quit, and healthcare system barriers, i.e., provider engagement and treatment availability (Table 2). Nicotine Replacement Therapy (NRT), financial incentives, and mobile-based supports were recurrent intervention-specific nodes. As depicted in Table 1, the yellow nodes represent outcome variables, the blue nodes represent exposure variables, the green nodes represent mediators, and the grey nodes represent confounders, as identified across each included study.
Across the 35 included studies, socioeconomic disadvantage was the most frequently identified barrier (reported in 54% of studies), followed by digital inequities or low digital access (43%), low motivation or readiness to quit (37%), and healthcare access barriers (34%). The most frequently reported facilitators were provider engagement or proactive outreach (49%), financial incentives (40%), digital engagement supports (34%), and culturally tailored interventions (29%). These constructs were consistently represented across RCTs, quasi-experimental, and observational studies, indicating their robustness within the synthesized evidence base.
3.2. Translation Stage and Integration of Extracted DAGs
Following the extraction of individual Directed Acyclic Graphs (DAGs), a structured translation procedure was implemented to harmonize constructs and establish temporal consistency across studies (Table A1 and Table A2). This process comprised three sequential steps:
3.2.1. Semantic Aggregation
Extracted nodes and edges, i.e., arrows between the nodes (hereafter referred to as edges or causal pathways), were systematically reviewed to identify and reconcile conceptual overlaps. Constructs with equivalent or closely related meanings (e.g., “technology literacy barriers” and “digital access challenges”) were merged into unified categories such as “Digital Access Barriers” or “quitting/vaping/smoking/cessation”. Similarly, outcome constructs, including quit attempt, abstinence, and relapse prevention, were standardized under the category Smoking Cessation. This ensured terminological coherence and reduced redundancy across datasets.
3.2.2. Temporal Re-Alignment
Constructs were organized according to their logical order of influence into upstream determinants, interventions, mechanisms, behaviors, and outcomes. Temporal sequencing was inferred using established causal reasoning and a health behavior framework, including Andersen and Aday’s Behavioral Model of Health Services Use. For example, distress consistently preceded intervention access and was thus retained as an upstream determinant rather than reclassified as a mechanism.
3.2.3. Directional Mapping and Validity Assessment
Causal edges were redrawn only when directionality was explicitly supported by primary data or demonstrated consistency across multiple sources. Recourse theory and temporal precedence informed the polarity of edges, thereby avoiding ambiguous or circular paths. Constructs with uncertain directionality were excluded. Face validity of the integrated map was assessed iteratively through expert consensus (n = 3) and triangulated with an established conceptual model.
No single study design was privileged. Instead, causal edges were extracted based on statistical support and mapped uniformly across RCTs, quasi-experimental, and observational studies. Edge direction and placement within the DAG were confirmed using cross-study consistency, temporal precedence, and theoretical plausibility.
3.3. Integrated DAG
The final Integrated Directed Acyclic Graph (iDAG) presents a comprehensive systems-level representation of the causal architecture underpinning smoking cessation interventions (Figure 1). By synthesizing 35 individual DAGs into a single unified framework, the iDAG illustrates the multilevel and interdependent processes that characterize tobacco cessation through the lens of Andersen and Aday’s Health Services Research conceptual model framework. It delineates how structural inequities cascade through access barriers, intervention modalities, psychological mechanisms, and behavioral mediators to shape cessation outcomes ultimately.
3.3.1. Structural: Upstream Determinants
The leftmost domain of the IDAG comprises upstream structural determinants, encompassing demographic and contextual factors such as psychological distress, age, digital access limitations, rural residence, health literacy, and psychosocial barriers. Although these constructs are largely non-manipulable, they are foundational in conditioning access to interventions and moderating treatment effectiveness. For example, psychological distress initiates two distinct causal trajectories: one leading toward Cognitive Behavioral Therapy (CBT) and another toward Nicotine Replacement Therapy (NRT) sampling, both mediated by improvements in coping capacity.
3.3.2. Intervention: Modality-Specific Pathways
The intervention layer identifies modality-specific pathways that align with the aforementioned upstream constraints. Geographic isolation directs individuals toward Acceptance and Commitment Therapy (ACT) based mobile applications, facilitating access to evidence-based tools. Digital access limitations and low health literacy channel participants toward social media and storytelling-based interventions that enhance message relevance and peer engagement. Psychological barriers are associated with the use of quitline services, which mitigate in-person access limitations. Each intervention node is linked to distinct mechanisms of action, highlighting how delivery modality and contextual appropriateness influence downstream behavioral change.
3.3.3. Mechanistic: Mediators of Change
Centrally positioned within the iDAG are mechanistic nodes such as improved coping skills, empowerment, social support, and behavioral nudges that mediate the causal effects of interventions. Their centrality underscores their critical role in translating intervention exposure into behavioral outcomes. CBT, NRT, and ACT-based approaches all converge on coping skill enhancement, suggesting strong theoretical coherence across modalities. Mechanisms such as automated provider prompts in electronic health record (EHR) systems and online peer engagement in digital platforms are intervention-specific, reinforcing the importance of causal pathway specificity in understanding intervention efficacy.
3.3.4. Behavioral: Modifiable Risk Factors
The behavioral layer comprises dynamic, modifiable mediators, including smoking frequency, dual use (cigarettes and vaping), alcohol consumption, and motivation to quit. These behavioral constructs link psychological mechanisms to cessation outcomes and capture known confounding relationships. For example, dual use and alcohol consumption often co-occur and collectively diminish cessation likelihood. Age and motivation to quit further moderate these dynamics, highlighting the complex feedback between readiness to change, behavioral risk factors, and cessation success.
3.3.5. Outcome: Smoking Cessation
At the terminal point of the IDAG lies the smoking cessation node, where all causal pathways converge. Cessation outcomes are influenced by both direct intervention effects and indirect pathways mediated through behavioral and psychological mechanisms. Notably, no upstream determinant connects directly to cessation without traversing intermediate nodes, underscoring the mediated and multistage nature of effective tobacco control strategies.
4. Discussion
The integrated ESC-DAG establishes complex and multifactorial causal pathways that affect tobacco cessation intervention outcomes in the United States. One of the key identified barriers was structural, i.e., socioeconomic disadvantage, digital inequities, and rurality, which affected access to interventions. These factors affected both the direct cessation outcomes and indirect mediators, including motivation, engagement, and treatment adherence. One of the key identified facilitators was provider engagement, emphasizing that healthcare system interactions remain crucial for cessation success.
The findings of this study are consistent with emerging international evidence emphasizing the importance of cultural tailoring and digital innovation in smoking cessation interventions. For instance, Bhatt et al. (2024) demonstrated that culturally and disease-specific multi-component interventions significantly improved cessation rates among patients attending non-communicable disease clinics in India, supporting the present study’s identification of cultural adaptation as a key facilitator [45]. Similarly, Okpako et al. (2024) found substantial interest in digital and virtual-reality–based cessation supports among smokers in Great Britain, reinforcing our DAG-derived conclusion that digital access and engagement pathways are pivotal to enhancing intervention reach and adherence [46].
Some of the underexplored pathways, i.e., cultural tailoring, minority stress, and stigma, emphasize crucial gaps in existing evidence as only a few edges supported these domains from existing empirical studies. This study has several limitations. First, the evidence base was restricted to studies conducted in the United States, which may limit the generalizability of the resulting DAG to other healthcare or cultural contexts. Second, as the synthesis relied on published quantitative studies, potential publication bias cannot be fully excluded, despite the comprehensive search and inclusion strategy of the source review. Third, challenges arose in harmonizing conceptually overlapping constructs such as stress, depression, and minority stress. While constructs were consolidated using theoretical and empirical alignment, this harmonization may have reduced specificity in some psychosocial pathways.
4.1. Methodological Contributions
This study demonstrates the added value of the ESC-DAG methodology over traditional narrative or systematic reviews. By translating empirical evidence into a unified graphical model, we identified confounders, mediators, and moderators that are often overlooked in conventional statistical synthesis. Unlike meta-analysis, which emphasizes effect sizes, ESC-DAG enables researchers to map relationships across diverse study designs and uncover the underlying causal architecture. This methodological innovation is particularly valuable for complex behavioral and health services interventions, where context and interaction effects are critical.
4.2. Policy and Practice Implications
The integrated DAG provides insights for designing equity-focused and targeted cessation interventions. It encompasses digital equity, socio-economic support, provider engagement, and cultural tailoring, which reinforces the need for multi-level interventions addressing not only individual motivation but also other systemic barriers to healthcare access.
The integrated DAG could be utilized to guide confounder adjustment in observational studies of tobacco cessation interventions by applying DAG-informed simulation models to predict the potential impact of scaling specific strategies. It could guide the design of tailored digital platforms that account for motivation levels, literacy, and socio-economic context. Beyond visualizing causal relationships, the integrated ESC-DAG can serve as a strategic framework to prioritize interventions and resource allocation. For instance, structural determinants such as digital inequities and socioeconomic disadvantage occupy upstream positions in the DAG, influencing multiple downstream mediators including motivation, engagement, and access to cessation support. Addressing these upstream nodes through digital equity initiatives (e.g., subsidized internet access, device provision, digital literacy training) or financial support mechanisms (e.g., free NRT, incentive-based programs) is likely to yield broader system-level impact than focusing solely on individual-level behavior change. Conversely, downstream facilitators such as provider engagement and motivational support can be targeted for shorter-term implementation or pilot interventions.
The DAG also provides a foundation for future simulation modeling and quasi-experimental trials by identifying high-priority mediators for targeted testing. For example, a comparative trial could evaluate whether addressing digital inequities produces greater cessation gains than financial incentive programs within resource-constrained settings. Furthermore, by mapping interdependencies between structural and psychosocial factors, the DAG can guide the sequencing of interventions, informing whether structural interventions should precede or accompany behavioral supports.
5. Conclusions
This study extends the methodological application of ESC-DAG to tobacco cessation research, synthesizing evidence from 35 studies into a unified causal framework. The integrated DAG highlights the central role of structural inequities, digital access, and provider engagement in shaping cessation outcomes.
By visualizing these relationships, our analysis demonstrates how DAGs can inform statistical modeling, guide intervention design, and prioritize equity-oriented policy solutions. Future research should build on this framework through simulation studies, quasi-experimental evaluations, and longitudinal designs to test targeted strategies for reducing disparities in cessation uptake.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leventhal A.M. Dai H. Higgins S.T. Smoking Cessation Prevalence and Inequalities in the United States: 2014–2019 JNCI J. Natl. Cancer Inst.202111438110.1093/jnci/djab 208PMC 890234634850047 · doi ↗ · pubmed ↗
- 2Maki K.G. Volk R.J. Disparities in Receipt of Smoking Cessation Assistance Within the USJAMA Netw. Open 20225 e 221568110.1001/jamanetworkopen.2022.1568135648402 PMC 9161016 · doi ↗ · pubmed ↗
- 3Lapoint D.N. Quigley B. Monegro A.F. Health Care Disparities and Smoking Cessation Counseling: A Retrospective Study on Urban and Non-Urban Populations Chest 2023164 A 639010.1016/j.chest.2023.07.4118 · doi ↗
- 4Van Frank B. Malarcher A. Cornelius M.E. Schecter A. Jamal A. Tynan M. Adult Smoking Cessation—United States, 2022 Morbidity and Mortality Weekly Report (MMWR)Centers for Disease Control MMWR Office Atlanta, GA, USA 202410.15585/mmwr.mm 7329 a 1PMC 1129090939052529 · doi ↗ · pubmed ↗
- 5Goodin A. Talbert J. Freeman P.R. Hahn E.J. Fallin-Bennett A. Appalachian Disparities in Tobacco Cessation Treatment Utilization in Medicaid Subst. Abus. Treat. Prev. Policy 202015510.1186/s 13011-020-0251-0PMC 697192231959212 · doi ↗ · pubmed ↗
- 6Sultana S. Inungu J. Jahanfar S. Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review Int. J. Environ. Res. Public Health 20252282510.3390/ijerph 2206082540566253 PMC 12193092 · doi ↗ · pubmed ↗
- 7Patel N. Karimi S.M. Little B. Egger M. Antimisiaris D. Applying Evidence Synthesis for Constructing Directed Acyclic Graphs to Identify Causal Pathways Affecting U.S. Early-Stage Non-Small Cell Lung Cancer Treatment Receipt and Overall Survival Therapeutics 20241649410.3390/therapeutics 1020008 · doi ↗
- 8Greenland S. Pearl J. Robins J.M. Causal diagrams for epidemiologic research Epidemiology 199910374810.1097/00001648-199901000-000089888278 · doi ↗ · pubmed ↗