Evaluating the Utility of Fresh Tissue in Molecular Diagnostics of Colorectal Cancer
Tadeusz Kałużewski, Szymon Wcisło, Kinga Sałacińska, Łukasz Kępczyński, Izabela Kubiak, Magdalena Grabiec, Ewa Kalinka, Bogdan Kałużewski, Agnieszka Gach

TL;DR
This study shows that fresh tissue from colorectal cancer surgeries can provide high-quality DNA for molecular testing, potentially improving diagnostic accuracy and speed.
Contribution
The study demonstrates the feasibility of using fresh tissue for molecular diagnostics in colorectal cancer, offering a potential alternative to FFPE tissue.
Findings
All 24 fresh tissue samples provided high-quality DNA suitable for sequencing.
Oncogenic mutations were identified in 87.5% of samples, primarily in APC, TP53, and KRAS genes.
Three samples lacked typical mutations, possibly due to low tumor cellularity or limitations of the gene panel.
Abstract
Colorectal cancer is a common oncological disease in which treatment decisions increasingly rely on detailed molecular testing of the tumor. In daily practice, such tests are usually performed on formalin-fixed, paraffin-embedded (FFPE) tissue, but fixation can damage DNA and reduce the quality of sequencing results. In this study, we explored whether small pieces of fresh tumor tissue collected directly during surgery could be used instead. We analyzed samples from 24 patients with colorectal cancer using a multigene next-generation sequencing panel. All fresh samples provided high-quality DNA and robust sequencing data, and cancer-driving mutations were identified in most tumors, mainly in APC, TP53 and KRAS genes. Our findings indicate that fresh tissue is a promising source of high-quality material for molecular diagnostics and may help shorten turnaround time, but careful control…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
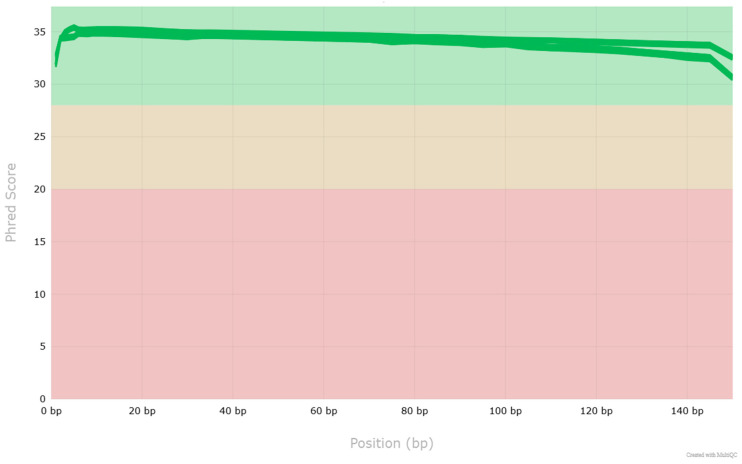 Figure 1
Figure 1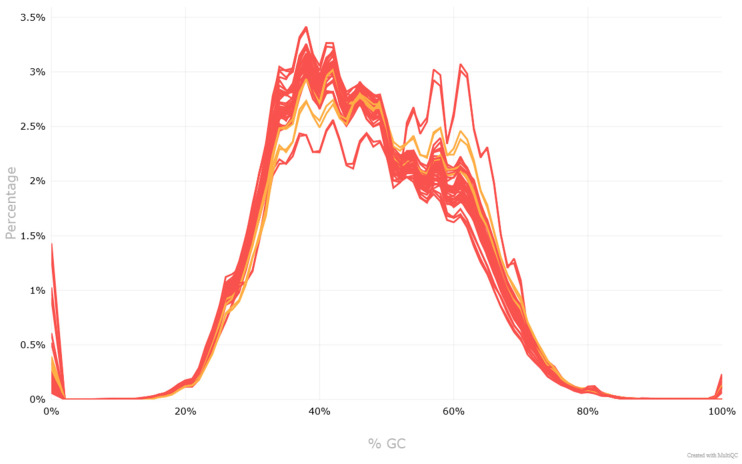 Figure 2
Figure 2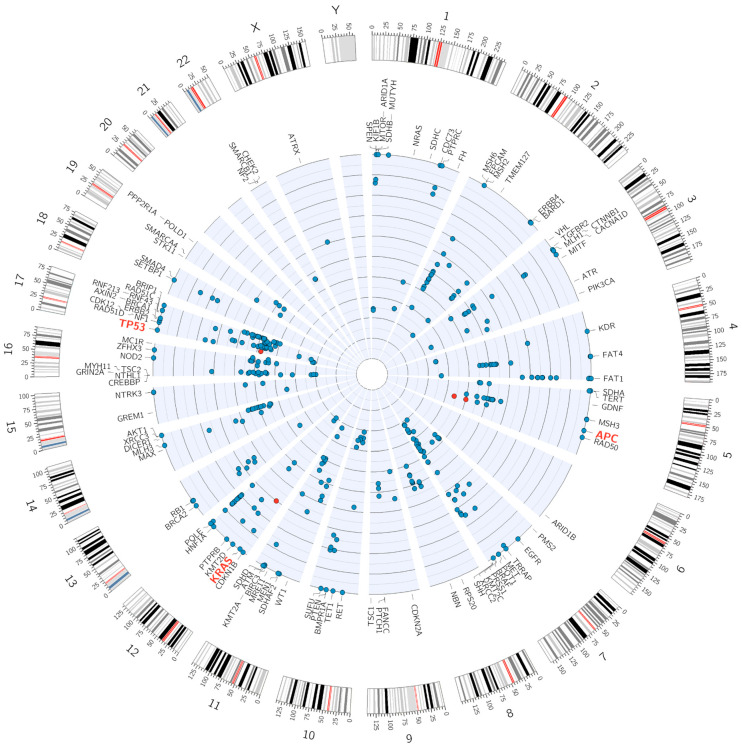 Figure 3
Figure 3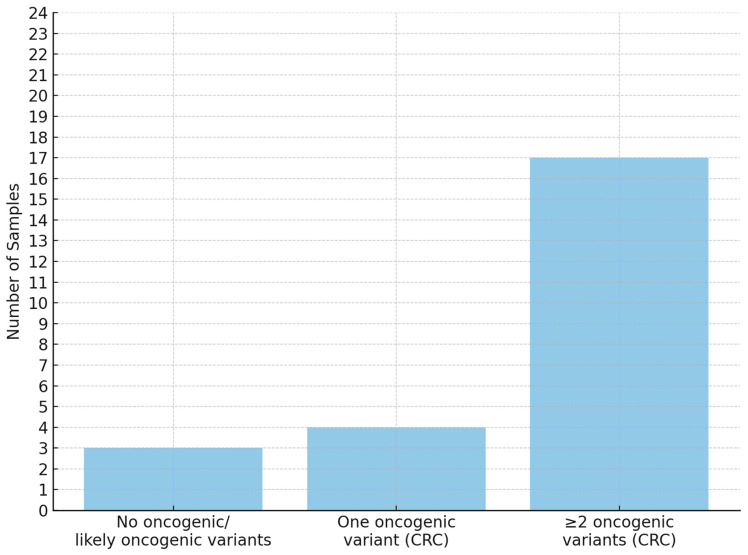 Figure 4
Figure 4- —Polish Mother’s Memorial Hospital—Research Institute (PMMH-RI)
- —Ministry of Science and Higher Education
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Genomics and Diagnostics · Molecular Biology Techniques and Applications · Genetic factors in colorectal cancer
1. Introduction
Colorectal cancer (CRC) remains one of the leading causes of cancer-related mortality worldwide and continues to represent a significant public health challenge [1]. In Poland, in 2021, CRC ranked as the third most common cancer among men and the fourth among women, with 10,009 and 7998 new cases, respectively. In terms of cancer-related deaths, it was the second leading cause among men (6570 cases) and the third among women (5022 cases) [2].
Advancements in diagnostic and therapeutic strategies have improved outcomes for CRC patients, with molecular testing emerging as a key component in expanding available treatment options [3]. Accurate and reliable molecular profiling of colorectal tumors is essential for guiding individualized treatment decisions and assessing prognosis [4]. Historically, molecular testing focused primarily on PCR-based detection of recurrent KRAS, NRAS, and BRAF mutations [5]. However, recent studies have continued to identify additional genes and molecular biomarkers relevant to colorectal cancer therapy [6]. As a result, there is a growing need to detect multiple concurrent alterations in tumor DNA using high-throughput technologies such as next-generation sequencing (NGS) [7,8]. However, high-throughput sequencing requires high-quality DNA to ensure reliable and accurate results [9,10]. This requirement highlights the importance of selecting appropriate sample types and preservation methods in clinical and research settings.
Formalin-fixed, paraffin-embedded (FFPE) tissue is currently the most commonly used sample type for molecular analysis [7]. Yet, fixation and long-term storage can lead to DNA cross-linking, fragmentation, and degradation. These factors may compromise both the quantity and quality of extracted DNA, potentially affecting the accuracy of mutation detection [11,12,13,14].
A key limitation associated with poor-quality DNA extracted from FFPE samples is the reduced presence of amplifiable DNA fragments of sufficient length [15]. This limitation negatively impacts the efficiency of library preparation, often leading to an increased proportion of PCR duplicates and uneven coverage across the sequenced regions, which are commonly observed characteristics of FFPE-derived material [16,17].
Particularly in the case of CRC, comparative studies emphasize that FFPE tissue stored for less than two years may serve as an acceptable source for mutation detection. However, various preanalytical and analytical factors—such as fixation time, storage conditions, and DNA integrity—can significantly impact the accuracy of results. From this perspective, FFPE should be used as an alternative only when fresh frozen tissue is not available, as discrepancies in mutation profiles may occur [18].
Nevertheless, an essential advantage of FFPE material is the ability to precisely assess tumor cell content through microscopic evaluation [19]. Consequently, current clinical guidelines recommend performing molecular testing only after prior or parallel histopathological verification by a pathologist, since the risk of obtaining a false-negative result due to the absence of tumor cells is considered higher than the risk associated with nucleic acid degradation during FFPE processing [20].
In cases of sufficiently large tumors, macroscopic evaluation during surgery may theoretically be adequate to identify tumor tissue suitable for molecular testing, which could then be conducted in parallel with histopathological assessment. This approach, applied selectively, may enable the acquisition of higher-quality material for genetic analysis and significantly shorten the time required to obtain molecular results. The present study aimed to evaluate this hypothesis using an in-house NGS-based multigene panel on fresh tissue samples collected during surgical resection from patients diagnosed with colorectal cancer.
2. Materials and Methods
2.1. Material Acquisition
Tissue samples were obtained from 24 patients diagnosed with colorectal adenocarcinoma during surgical procedures performed as part of routine therapeutic management. Small fragments of tissue, each measuring a few millimeters, were selected based on macroscopic examination, clearly indicative of tumor presence. Particular care was taken to ensure that sample collection did not interfere with the concurrent histopathological assessment, thereby preserving the diagnostic integrity of the specimens. The samples were immediately preserved in RNA Save solution (Biological Industries, Kibbutz Beit Haemek, Israel) and stored at 20 °C until nucleic acid isolation. All of the subjects included in the study had confirmed tumor cell content in sample parts that were subjected to parallel histopathological examinations.
2.2. DNA Isolation and Next-Generation Sequencing
Manual extraction of genomic DNA was performed using the Sherlock AX Kit (A&A Biotechnology, Gdansk, Poland) in accordance with the manufacturer’s instructions, following prior mechanical homogenization of the samples. Next-generation sequencing (NGS) was conducted using a 150 bp paired-end method on the MiniSeq platform (Illumina, San Diego, CA, USA). AmpliSeq DNA On-Demand libraries were prepared following the manufacturer’s instructions using the Mid Output Kit (Illumina, San Diego, CA, USA). A custom gene panel comprising 110 genes was designed using Illumina Design Studio software (Illumina, San Diego, CA, USA) to enable the sequencing of coding exons and adjacent non-coding regions. Panel content was based on a comprehensive review of the literature and databases such as PubMed and COSMIC. The following genes associated with colorectal cancer were included: AKT1, APC, ARID1A, ARID1B, ATM, ATR, ATRX, AXIN2, BARD1, BIRC3, BMPR1A, BRAF, BRCA1, BRCA2, BRIP1, CACNA1D, CDC73, CDK12, CDKN1B, CDKN2A, CHEK2, CREBBP, CTNNB1, DICER1, EGFR, EPCAM, ERBB2, ERBB4, FANCC, FAT1, FAT4, FH, GDNF, GREM1, GRIN2A, HNF1A, HNF1B, HOXB13, KDR, KIF1B, KMT2A, KMT2C, KMT2D, KRAS, MAX, MC1R, MEN1, MET, MITF, MLH1, MLH3, MRE11, MSH2, MSH3, MSH6, MTOR, MUTYH, MYH11, NBN, NF1, NF2, NOD2, NTHL1, NRAS, NTRK3, PIK3CA, PMS2, POLD1, POLE, POT1, PPP2R1A, PRKAR1A, PRSS1, PTCH1, PTEN, PTPRB, PTPRC, RAD50, RAD51C, RAD51D, RB1, RET, RNF213, RNF43, RPS20, SDHA, SDHAF2, SDHB, SDHC, SDHD, SETBP1, SHH, SMAD4, SMARCA4, SMARCB1, SPEN, STK11, SUFU, TERT, TET1, TGFBR2, TMEM127, TP53, TRRAP, TSC1, TSC2, VHL, WT1, XRCC2, XRCC3, ZFHX3.
2.3. Bioinformatics and Variant Classification
The identification of single-nucleotide variants (SNVs) as well as short insertions and deletions (delins) was performed using the GATK software suite (v4.6.0.0) [21], following the Best Practices recommendations [22,23]. Prior to variant calling, sequencing reads were aligned to the hg19 reference genome using BWA (v.0.7.17) [24], and converted to BAM format using SAMtools (v1.10). Quality metrics were generated with MultiQC (v1.22.2). Variant annotation was conducted using the Franklin platform (QIAGEN N.V., Hilden, Germany), and variant classification was performed according to the AMP/ACMG guidelines for pathogenicity and the ClinGen-CGC-VICC guidelines for oncogenicity. A graphical representation of the variant distribution was generated using Circos software (v0.69.9) [25].
3. Results
3.1. Patient Characteristics
A total of 24 patients were included in the study, comprising 6 men (mean age: 74.3 years) and 18 women (mean age: 70.0 years). The group comprised two female patients representing early-onset cases (age ≤ 50 years). The majority of patients were either overweight (n = 10) or obese (n = 7), while six patients had a normal body weight, and only one was underweight. Tumor samples were described in terms of size, pathological TNM classification (pTNM), and presence of metastases. Primary tumor location was rectum in 8/23 (34.8%) and colon in 15/23 (65.2%). Among colonic tumors, right-sided sites (cecum, ascending, transverse) accounted for 9/23 (39.1%), whereas left-sided sites (descending, sigmoid) accounted for 6/23 (26.1%). Histologic grade was predominantly G2 in 15/23 (65.2%) and G3 in 2/23 (8.7%). Grade was unreported/indeterminate in 6/23 (26.1%). Additionally, data on patients’ smoking history (pack-years) were collected. Detailed patient characteristics are presented in Table 1.
3.2. NGS Results
Next-generation sequencing was successfully performed for all samples. Quality assessment confirmed that the raw sequencing reads exhibited high quality across all 48 FASTQ files (Figure 1). Per-base sequence quality scores were consistently above Q30 for the majority of read positions, and no significant adapter contamination was detected. The GC content distribution matched the expected range of approximately 40–60% for human genomic DNA (Figure 2). Duplication levels were within acceptable limits for genomic DNA libraries. Mapping-based evaluation of the aligned BAM files revealed a mean sequencing depth of 101.56× across all tumor samples, with coverage values ranging from 56.29× to 129.89×. Coverage was uniformly distributed across the targeted genomic regions, with no pronounced dropout regions, confirming the suitability of the data for downstream analyses, including somatic mutation calling.
The applied panel enabled the detection of a broad spectrum of point mutations as well as small insertions and deletions (Figure 3). In 18 out of 24 cases, oncogenic or potentially oncogenic variants were identified in genes associated with the conventional pathway (CIN—chromosomal instability pathway) of colorectal cancer development. The detected CIN-associated variants are presented in the following tables: APC (Table 2), TP53 (Table 3), and KRAS (Table 4). In 3 out of 24 cases, oncogenic variants associated with the serrated or MSI (microsatellite instability) pathways were detected: the oncogenic BRAF c.1799T > A p.(Val600Glu) variant was found in two samples (classification criteria: OS1 + 4, OS3 + 4, OP1 + 1, OP4 + 1), while oncogenic MSH6 NM_000179.3:c.3261dup p.(Phe1088Leufs5) and likely oncogenic TGFBR2 NM_003242.6:c.382_383del p.(Lys128Alafs3) variants were found together in one sample (classification criteria: OVS1 + 8, OS1 + 4, OP4 + 1 and OVS1 + 8, OP4 + 1, respectively). In 3 of the 24 samples, no mutations typically associated with colorectal cancer were detected. The summary of oncogenic variant frequencies is presented in Figure 4.
3.3. Clinical Characteristics
Although investigating associations between patients’ clinical characteristics and detected genetic variants was not the primary objective of this study, exploratory analyses were conducted to expand the current understanding of variant relevance in a clinical context. The distribution of identified variants was analyzed in relation to tumor grade, size and localization, presence of metastases, patient age (<50 vs. ≥50 years), sex, body mass index (BMI), and duration of smoking history. No statistically significant correlations were observed within the examined cohort, which is likely attributable to the limited sample size and relatively low clinical heterogeneity of the study population. However, the applied panel allowed for the identification of a potentially germline variant in the HOXB13 gene, NM_006361.6:c.251G>A p.(Gly84Glu), in a female patient. This specific variant is a well-characterized European founder mutation known to be associated with a significantly increased risk of prostate cancer, particularly in individuals of European ancestry [26]. Current evidence does not support an association between this variant and an increased risk of colorectal cancer or malignancies typically affecting women, such as breast or ovarian cancer [27]. The clinical relevance of this incidental finding in the context of a non-prostate cancer setting remains uncertain.
4. Discussion
The aim of this study was to evaluate the use of fresh tumor tissue for next-generation sequencing (NGS) in colorectal cancer (CRC) as a source of high-quality molecular data. All 24 fresh samples in our cohort were successfully sequenced with adequate depth and uniform coverage. Oncogenic or likely oncogenic variants were identified in the majority of cases (21/24, 87.5%). These results suggest that, when sufficient tumor content is present, intraoperative sampling of fresh tissue can provide DNA of excellent quality for mutation analysis and may potentially reduce turnaround time by enabling parallel processing with histopathology. Avoiding formalin fixation allows avoiding DNA crosslinking and degradation, which are known to introduce sequencing artifacts and reduce detectable variant yield, as previously described [18]. However, a critical limitation emerged in the few cases where no oncogenic variants were detected despite macroscopic tumor identification. In three patients, the used NGS panel did not reveal any typical CRC-associated mutations, raising concern for false-negative results. One possible explanation is an insufficient tumor cell content in the analyzed tissue fragment, meaning that the sample may have contained mostly non-neoplastic cells despite appearing tumorigenic on macroscopic evaluation. Another possibility is the absence of typical sequence mutations in the genes covered by the panel, which does not exclude other molecular alterations such as DNA methylation, genomic imbalances, or epigenetic instability [28]. Both of the above scenarios highlight the well-recognized risk of performing molecular testing on tissue that has not been histologically verified. The risk of a false-negative result might outweigh the advantages of improved DNA quality gained by immediate fresh tissue testing. Our observation of mutation-negative cases supports this concern, especially when considering the methodology used. Another notable finding from the study is that a subset of tumors harbored isolated APC mutations as the single driver alteration. APC is a tumor suppressor gene that acts as a gatekeeper in colorectal tumorigenesis, and it is well established that its mutations occur in more than 80% of sporadic CRCs very early in tumorgenesis [29,30,31]. Since these changes without additional findings may point to either biologically indolent tumor areas or limitations of the testing panel, the presence of an isolated APC truncating mutation in an apparently malignant tumor sample cannot be treated as a definitive molecular marker confirming the presence of CRC. These considerations naturally raise the question of how molecular diagnostic panels might be expanded. One strategy to increase diagnostic yield seems to be the use of broader DNA sequencing approaches, such as whole-exome or whole-genome sequencing, which could identify rare or novel driver mutations not included in targeted panels. Another complementary approach is to incorporate RNA-based profiling that could detect pathogenic gene fusions and aberrant splice variants that are undetectable through DNA sequencing.
The incidental finding in the study was the detection of a germline HOXB13 p.(Gly84Glu) pathogenic variant in a female patient. It is a well-characterized hereditary mutation associated with increased prostate cancer risk. Therefore, its presence in a female patient with CRC is most likely a coincidental finding unrelated to her colorectal tumor. However, this case serves as an example of how broad tumor sequencing may incidentally uncover germline variants of potential clinical significance with implications for genetic counseling. As such, offering extended NGS panels should ideally include strategies for distinguishing somatic from germline variants, for example, by performing parallel sequencing of a matched peripheral blood sample. Determining the relevance of such findings seems to be a critical component of modern precision oncology.
5. Conclusions
In summary, our evaluation of fresh tissue for molecular diagnostics in CRC highlights both the promise and limitations of this approach. Performing NGS on unfixed tumor samples can provide highly accurate genomic information and potentially shorten the path to clinically actionable results. However, the applied methodology does not currently support routine clinical implementation for diagnostic purposes. The used custom-designed gene panel did not allow detection of many alterations currently known to be characteristic of tumor cells. Moreover, the cohort size limits the statistical significance and generalizability of our findings. Future strategies that enable the capture of the full spectrum of genomic alterations—including regulatory variants, deep intronic alterations, complex or large structural variants, epigenetic changes, and gene expression signatures—could refine the sensitivity of molecular diagnostics in CRC and better leverage the advantages of fresh tissue use. Recent advances in computational pathology, such as AI-based tumor cellularity assessment, may help address the limitations observed in our study. As recently demonstrated by Gertych et al. [32], artificial intelligence models trained on histology images can accurately predict the likelihood of successful molecular testing by quantifying tumor cell content prior to sequencing. Integrating such tools into routine workflows may significantly reduce the risk of false-negative results arising from inadequate tumor sampling. As precision oncology continues to advance, such approaches may become increasingly important in delivering timely and comprehensive genomic data to guide cancer patient management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Keum N. Giovannucci E. Global Burden of Colorectal Cancer: Emerging Trends, Risk Factors and Prevention Strategies Nat. Rev. Gastroenterol. Hepatol.20191671373210.1038/s 41575-019-0189-831455888 · doi ↗ · pubmed ↗
- 2Didkowska J. Barańska K. Miklewska M.J. Wojciechowska U. Cancer Incidence and Mortality in Poland in 2023 Nowotw. J. Oncol.202474759310.5603/njo.99065 · doi ↗
- 3De Stefanis R.A. Kratz J.D. Emmerich P.B. Deming D.A. Targeted Therapy in Metastatic Colorectal Cancer: Current Standards and Novel Agents in Review Curr. Color. Cancer Rep.201915616910.1007/s 11888-019-00430-6PMC 652881331130830 · doi ↗ · pubmed ↗
- 4Fleming M. Ravula S. Tatishchev S.F. Wang H.L. Colorectal Carcinoma: Pathologic Aspects J. Gastrointest. Oncol.2012315317310.3978/j.issn.2078-6891.2012.03022943008 PMC 3418538 · doi ↗ · pubmed ↗
- 5Mármol I. Sánchez-de-Diego C. Pradilla Dieste A. Cerrada E. Rodriguez Yoldi M.J. Colorectal Carcinoma: A General Overview and Future Perspectives in Colorectal Cancer Int. J. Mol. Sci.20171819710.3390/ijms 1801019728106826 PMC 5297828 · doi ↗ · pubmed ↗
- 6Goel G. Molecular Characterization and Biomarker Identification in Colorectal Cancer: Toward Realization of the Precision Medicine Dream Cancer Manag. Res.2018105895590810.2147/CMAR.S 16296730510457 PMC 6250110 · doi ↗ · pubmed ↗
- 7Normanno N. Rachiglio A.M. Roma C. Fenizia F. Esposito C. Pasquale R. La Porta M.L. Iannaccone A. Micheli F. Santangelo M. Molecular Diagnostics and Personalized Medicine in Oncology: Challenges and Opportunities J. Cell. Biochem.201311451452410.1002/jcb.2440122991232 · doi ↗ · pubmed ↗
- 8Rey J.-M. Ducros V. Pujol P. Wang Q. Buisine M.-P. Aissaoui H. Maudelonde T. Olschwang S. Improving Mutation Screening in Patients with Colorectal Cancer Predisposition Using Next-Generation Sequencing J. Mol. Diagn.20171958960110.1016/j.jmoldx.2017.04.00528502729 · doi ↗ · pubmed ↗