Longitudinal Association of Maternity Care Practices with Exclusive Breastfeeding in U.S. Hospitals, 2018–2022
Lucas Gosdin, Kristin J. Marks, O. Yaw Addo, Lauren O’Connor, Sofia Awan, Daurice A. Grossniklaus, Heather C. Hamner

TL;DR
Hospitals that improved their maternity care practices saw higher rates of exclusive breastfeeding over time.
Contribution
This study shows that sustained improvements in maternity care practices lead to increased exclusive breastfeeding rates in U.S. hospitals.
Findings
Hospitals with higher maternity care scores had consistently higher exclusive breastfeeding rates from 2018 to 2022.
A 10-point increase in maternity care scores was linked to a 2 percentage point rise in exclusive breastfeeding rates.
Higher 2018 maternity care scores predicted higher 2022 exclusive breastfeeding rates through improved practices in 2018 and 2020.
Abstract
What are the main findings? Certain maternity care practices and policies can support families to breastfeed. Across the United States, hospitals that improved and sustained maternity care practices were more likely to have higher in-hospital exclusive breastfeeding rates. What is the implication of the main finding? Improving and sustaining maternity care practices and policies supportive of breastfeeding might increase in-hospital exclusive breastfeeding over time. Background/Objectives: Breastfeeding has health benefits for infants and mothers, and hospitals play an important role in supporting breastfeeding. This analysis examines the longitudinal association of hospital maternity care practices and policies with in-hospital exclusive breastfeeding rates from 2018 to 2022. Methods: U.S. hospitals completing ≥2 surveys during 2018, 2020, and 2022 cycles of CDC’s Maternity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
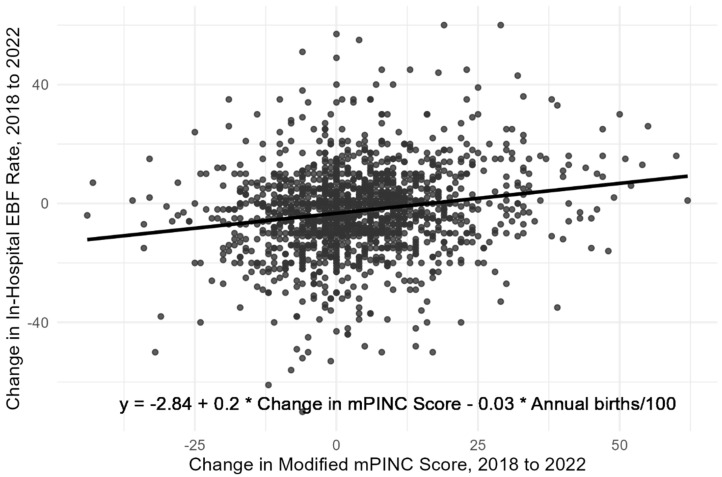 Figure 1
Figure 1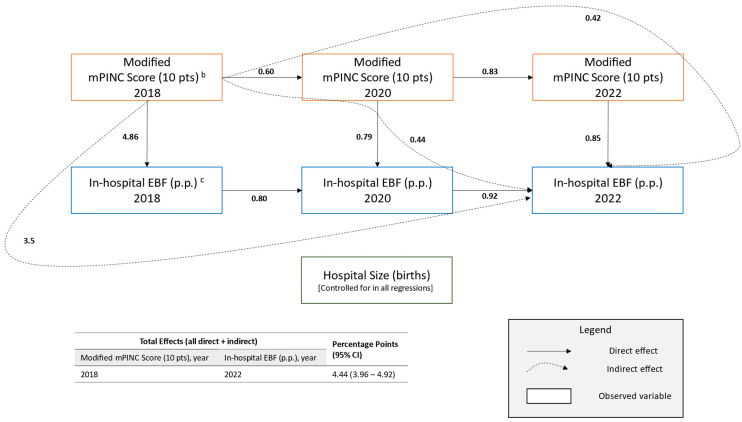 Figure 2
Figure 2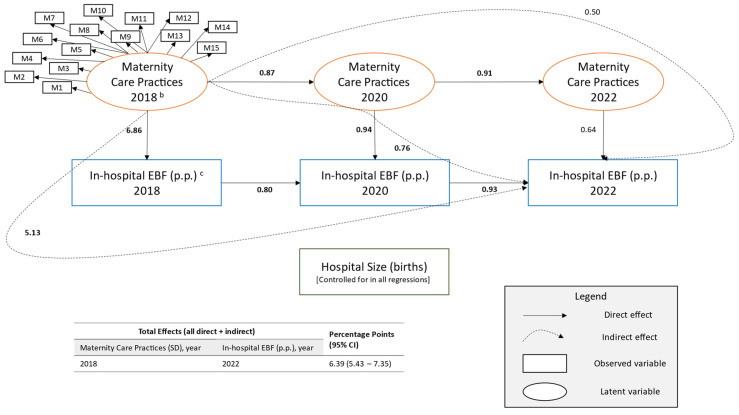 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Maternal Mental Health During Pregnancy and Postpartum · COVID-19 Impact on Reproduction
1. Introduction
Breast milk is the optimal form of nutrition for most infants and has health benefits for children and women who breastfeed them [1,2,3,4]. While most families in the United States initiate breastfeeding (84.1% for children born in 2021) [5], fewer achieve recommendations to exclusively feed breast milk through about 6 months of age [6,7,8] (27.2% for children born in 2021) [5]. Families are more likely to provide breast milk to their children when they are supported to do so [9]. Because around 98% of deliveries in the United States are in hospitals [10], they are the first environment where most infants are fed and are important partners in supporting families to start breastfeeding.
Certain maternity care practices are associated with better breastfeeding outcomes including in-hospital exclusive breastfeeding [9]. The World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) established the Baby-Friendly Hospital Initiative to implement a collection of hospital practices and policies supportive of breastfeeding called the Ten Steps to Successful Breastfeeding (Ten Steps) [11].
Various cross-sectional studies have found that hospitals with maternity care practices and policies supportive of breastfeeding are more likely to have higher in-hospital exclusive breastfeeding rates [12,13,14]. Prospective studies in the United States have also found that individuals who receive maternity care consistent with the Ten Steps have better breastfeeding outcomes [13]. Other studies have examined the effects of quality improvement initiatives in hospitals and found that improving maternity care practices and policies to align with the Ten Steps was associated with improved in-hospital exclusive breastfeeding rates [15,16]. However, there is limited evidence, representing the diversity of hospitals in the United States, that documents the effects of maternity care practices supportive of breastfeeding on hospital-level breastfeeding outcomes over time at the national level.
This analysis examines the longitudinal association of maternity care practices supportive of breastfeeding on in-hospital exclusive breastfeeding within diverse hospitals across United States and territories during 2018 to 2022.
2. Materials and Methods
The Centers for Disease Control and Prevention (CDC) conducts a biennial survey of Maternity Practices in Infant Nutrition and Care (mPINC) for which all hospitals that provided maternity care in United States and territories in the preceding year are eligible [17].
This analysis was limited to the survey cycles that occurred after it was revised in 2018 to capture more recent developments in infant feeding-related U.S. maternity care. Hospitals completing at least two surveys during the 2018, 2020, and 2022 survey cycles were included to form a nested longitudinal cohort (n = 2109).
In 2018, 2045 of 2913 eligible hospitals participated (70%), of which 1811 completed at least one subsequent survey cycle. In 2020, 2103 of 2810 eligible hospitals participated (75%), of which 1949 completed at least one additional survey cycle. In 2022, 1994 of 2779 eligible hospitals participated (72%), of which 1822 completed at least one previous survey cycle. There were 1521 hospitals that participated in both 2018 and 2022.
2.1. Measures
The mPINC questionnaire includes 21 measures of maternity care practices and policies that are consistent with national and international recommendations and supported by scientific evidence [18]. These measures are scored relative to best practices in maternity care and are sorted into domains and averaged. Then, the domain scores are combined into an overall score for each participating hospital [19]. Because this analysis focuses on in-hospital exclusive breastfeeding, practices that related directly to the outcome (proportion of breastfed newborns fed infant formula and the proportion of formula-fed infants whose parents were taught formula preparation and formula feeding techniques) or that occurred after the outcome (discharge support) were excluded from the exposure, resulting in a modified mPINC score. The remaining measures within the feeding practices and feeding education domains were combined after removing the excluded measures because they were conceptually similar. Combining these two domains also ensured that each domain has at least three component measures. The modified mPINC score consisted of 15 measures covering four domains: immediate postpartum care; rooming-in; feeding practices, education, and support; and institutional management (Table 1). The measures were scored within each domain by taking the mean of its component survey items, and the modified mPINC score is an average of the four domains. The modified score ranges from 0 points (implementing none of the 15 best practices and policies) to 100 points (fully implementing all 15 best practices and policies).
In-hospital exclusive breastfeeding rate was reported by each hospital as the percent of healthy newborns who received only breast milk—and no water or formula at any time during hospitalization as well as no glucose water or sucrose solution except during painful procedures. Hospitals reported either an actual percentage (51% of hospitals) or an estimated percentage (49% of hospitals) of in-hospital exclusive breastfeeding. Hospitals did not report how they arrived at estimates. Within each survey year, mean in-hospital exclusive breastfeeding was approximately 3 percentage points higher for those who reported an actual percentage than those who reported an estimated percentage.
2.2. Analysis
First, mean in-hospital exclusive breastfeeding rates are presented by modified mPINC domain scores and overall scores within each survey cycle. Since the mPINC survey is a census and, therefore, has no sampling error, descriptive statistics are presented without inferential statistics.
Second, to isolate the effects of changes in maternity care practices, an ordinary least squares model of differences was used to estimate the average change in in-hospital exclusive breastfeeding rate between 2018 and 2022 for each 10-point change in modified mPINC score over the 4-year period. A 10-point change was used because it is a familiar difference for a 100-point scale and represents implementation of one or two improved practices. This method quantifies the magnitude and direction of changes and treats no change in maternity care practices and exclusive breastfeeding rate as zero for the exposure and outcome, respectively.
Third, to assess the longitudinal association of both changing and sustaining higher mPINC scores with in-hospital exclusive breastfeeding rate, a multi-mediation structural equation model (path analysis), with full information maximum likelihood for missing data, was fit. This model estimated the direct, indirect, and total effects of modified mPINC score on in-hospital exclusive breastfeeding rates across time. Model fit was assessed by both omnibus—chi-square, root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR)—and incremental fit indices—comparative fit index (CFI) and Tucker-Lewis index (TLI) [20]. The final model was equivalent to the a priori model. Structural equation models can account for both changing and sustaining maternity care practices through multiple, simultaneous regression equations.
Finally, as a sensitivity analysis, a full structural equation model was fit to examine how the association might change if the modified mPINC score was substituted with a data-driven approach to combining the measured practices and policies. This model was equivalent to the path analysis except that the modified mPINC score was replaced with a latent factor (“maternity practices”) representing the 15 observed measures that make up the modified mPINC score. The measures were dichotomized based on the ideal response for each. Factor loadings for each observed measure were constrained across time so that latent factors were equivalent for each survey cycle. This model was refit to include covariance parameters among the endogenous variables of latent factors as suggested by modification indices and consistent with operating hypotheses [21].
All analyses were conducted in R version 4.2.1 (The R Foundation for Statistical Computing, Vienna, Austria) using the “tidyverse” and “lavaan” packages [21,22]. All models were adjusted for hospital size. Other variables were assessed for confounding, including hospital type, geographic region, and level of neonatal care, but did not change estimates or interpretation and were left out in favor of a more parsimonious model. An a priori alpha was set at 0.05 for statistical significance.
3. Results
Hospitals included in this nested cohort were diverse and geographically well distributed. Most hospitals were non-profit (77.1%), had fewer than 1000 annual births (56.7%), and did not have a neonatal advanced care unit (70.7%) (Table 2).
Overall, among hospitals with modified mPINC scores of 100 points (highest score), the mean in-hospital exclusive breastfeeding rates were 62.0% in 2018, 62.2% in 2020, and 61.7% in 2022; whereas hospitals with scores of <60 points (lowest scores) had in-hospital exclusive breastfeeding rates of 40.6%, 41.9%, and 37.8%, respectively (Table 3). In each survey year and within each domain of maternity care practices and policies, there was an increase in in-hospital exclusive breastfeeding rate with increasing modified mPINC score. For example, in 2022, hospitals with scores of <60, 60–79, 80–99, and 100 points in the Rooming-In domain had in-hospital exclusive breastfeeding rates of 49.1%, 52.9%, 53.6%, and 56.1%, respectively. Hospitals with scores of <60, 60–79, 80–99, and 100 points in the Feeding Practices, Education, and Support domain had in-hospital exclusive breastfeeding rates of 37.5%, 47.0%, 51.4%, and 56.7%, respectively.
In an ordinary least squares model of differences (n = 1521), a 10-point increase in mPINC score between 2018 and 2022 was associated with a 2.00 (95% CI, 1.46–2.54) percentage point (p.p.) increase in the rate of in-hospital exclusive breastfeeding during the same period, controlling for the number of births in the hospital (Figure 1).
In an adjusted path analysis (n = 2109), each 10-point higher modified mPINC score for a hospital in 2018 was associated with a 4.44 (3.96–4.92) p.p. (Figure 2) higher in-hospital exclusive breastfeeding rate in 2022 (standardized coefficient = 0.34 [0.30–0.37]; Table A1). This association was driven by increasing the likelihood of higher subsequent modified mPINC scores (indirect effect: 0.42 [0.20–0.65] p.p.), higher in-hospital exclusive breastfeeding rates in previous years (indirect effect: 3.58 [3.14–4.01] p.p.), and higher scores with higher exclusive breastfeeding rates in the intervening years (indirect effect: 0.44 [0.21–0.66] p.p.) (Figure 2).
Results were similar when the modified mPINC score was replaced with a latent variable of its component measures. In a full structural equation model (n = 2109), with each one standard deviation increase of the latent variable “maternity care practices” for a hospital in 2018 there was a 6.39 (5.43–7.35) p.p. higher in-hospital exclusive breastfeeding rate in 2022 (standardized coefficient = 0.30 [0.26–0.34]; Table A2). This association was also driven by indirect effects through increasing the likelihood of higher subsequent modified mPINC scores (indirect effect: 0.50 [−0.07–1.08] p.p.), higher in-hospital exclusive breastfeeding rates in previous years (indirect effect: 5.13 [4.33–5.92] p.p.), and higher scores with higher exclusive breastfeeding rates in the intervening years (indirect effect: 0.76 [0.22–1.29] p.p.) (Figure 3).
4. Discussion
Over a 4-year period, U.S. hospitals with better maternity care practices and policies supportive of breastfeeding had higher rates of in-hospital exclusive breastfeeding. For example, hospitals with 10-point higher modified mPINC scores in 2018 had 4.4 p.p. higher in-hospital exclusive breastfeeding rates in 2022 by increasing the likelihood of having higher subsequent modified mPINC scores and exclusive breastfeeding rates. Hospitals that increased their modified mPINC score by 10 points during the same period, regardless of their score in 2018, had a 2.0 p.p. increase in their exclusive breastfeeding rate. This shows that both sustaining and improving maternity practices supportive of breastfeeding can potentially result in improvements of in-hospital exclusive breastfeeding. For example, a 10-point increase in modified mPINC score, as examined in this analysis, is equivalent to implementing two policies in the institutional management domain or approximately one to two practices from the remaining domains. These policy or practice differences are associated with meaningful improvements for in-hospital exclusive breastfeeding.
Previous studies have found similar results when examining maternity care practices cross-sectionally with higher mPINC scores being correlated with higher rates of in-hospital exclusive breastfeeding [23]. Other evaluations have found that increasing hospital supports for breastfeeding were associated with increased breastfeeding rates. In one evaluation of a state quality improvement collaborative, hospitals that began implementing an average of 2.2 more of the Ten Steps over 2 years had approximately 17 p.p. higher in-hospital exclusive breastfeeding rates [24]. In an ecological analysis, a state’s average hospital mPINC score increased by 15 points over 4 years and coincided with an increase of 17 p.p. in the state in-hospital exclusive breastfeeding rate [15]. The aforementioned evaluations estimated larger effects than this analysis; however, they may not be directly comparable because they were done in the context of intensive interventions in smaller geographic areas. Data that are more directly comparable to the present analysis are limited.
This study is strengthened by national, hospital-level data that spans multiple years with robust and consistent response rates. The evidence-based practices and policies were assessed holistically, which more closely mirrors how they are implemented rather than examining individual practices. The study examined the effects associated with both changing practices and maintaining better practices, which also better reflects their implementation than examining changes alone.
4.1. Limitations
This study is also subject to several limitations. First, this is an observational analysis and, therefore, limits the ability to infer a causal relationship between the exposure and outcome. This design is also unable to account for changes in unobserved factors that might have affected exclusive breastfeeding rates during this period, such as changes in the patient population and other potential unmeasured confounding variables. Second, the mPINC survey is completed by the person(s) most knowledgeable of infant feeding in the hospital but might not reflect hospital practices and policies with complete accuracy. In-hospital exclusive breastfeeding is also reported by the hospital respondent as either the actual percentage or an estimate. It is unclear how hospitals arrive at their estimates and are likely subject to error. However, those reporting actual percentages had slightly higher proportions of in-hospital exclusive breastfeeding, which is expected given that tracking exclusive breastfeeding is part of the Ten Steps. Third, while the survey is a census, the response rates varied, and there may have been differential participation by hospital maternity practices and in-hospital exclusive breastfeeding rates. However, the nested cohort design limits the effects of any such biases since the longitudinal comparisons are made among the same group of hospitals over time. Fourth, the modified mPINC score, which treats each measure within a domain as equal, might not optimally capture maternity care practices and policies as they relate to in-hospital exclusive breastfeeding. However, the mPINC score is associated with breastfeeding outcomes and is an important tool for hospitals and public health surveillance [14,17]. Fifth, we removed measures of practices related to formula feeding and discharge, which further focused the modified mPINC score on practices and policies that could affect in-hospital exclusive breastfeeding. Thus, the modified score cannot be directly compared to the mPINC score.
Because of the potential limitations of the modified mPINC score, maternity care practices and policies were also modelled as a latent variable of its component measures using a full structural equation model. This did not change the pattern of the relationships observed, adding credibility to the modified mPINC score when examining in-hospital exclusive breastfeeding as an outcome. In fact, the standardized coefficients for the examined total effects are very similar.
Model fit indices indicated good fit for the path model [20]. The full structural equation model has only fair fit, but its composition is guided by causal hypotheses and was therefore not refit with additional parameters that veered from the hypothesized relationships. We interpret the full structural equation model as confirming the pattern seen in the path model.
4.2. Implications
This analysis observes improvements of in-hospital exclusive breastfeeding rates among hospitals with maternity care practices and policies supportive of breastfeeding—during a period of little to no improvement in mPINC scores at the national level [25]. This highlights opportunities to improve maternity care and infant nutrition.
5. Conclusions
These results can be used to build support for improving and maintaining maternity care practices supportive of breastfeeding, which can have lasting effects on breastfeeding outcomes in hospitals. Though hospitals have relatively limited time with each patient, their evidence-based practices and policies can support families to start and sustain breastfeeding during their hospital stay and build a foundation for good infant nutrition thereafter.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chowdhury R. Sinha B. Sankar M.J. Taneja S. Bhandari N. Rollins N. Bahl R. Martines J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis Acta Paediatr.20151049611310.1111/apa.1310226172878 PMC 4670483 · doi ↗ · pubmed ↗
- 2Stoody E.E. Spahn J.M. Casavale K.O. The Pregnancy and Birth to 24 Months Project: A series of systematic reviews on diet and health Am. J. Clin. Nutr.2019109(Suppl. S 7)685S 697S 10.1093/ajcn/nqy 37230982878 · doi ↗ · pubmed ↗
- 3Ip S. Chung M. Raman G. Chew P. Magula N. De Vine D. Trikalinos T. Lau J. Breastfeeding and maternal and infant health outcomes in developed countries Evid. Rep. Technol. Assess. Full Rep.20071531186 PMC 478136617764214 · pubmed ↗
- 4Feltner C. Weber R.P. Stuebe A. Grodensky C.A. Orr C. Viswanathan M. AHRQ Comparative Effectiveness Reviews Breastfeeding Programs and Policies, Breastfeeding Uptake, and Maternal Health Outcomes in Developed Countries Agency for Healthcare Research and Quality (US)Rockville, MD, USA 201830204377 · pubmed ↗
- 5Centers for Disease Control and Prevention NIS-Child Breastfeeding Rates Available online: https://www.cdc.gov/breastfeeding-data/survey/results.html(accessed on 4 October 2024)
- 6Meek J.Y. Noble L. Technical Report: Breastfeeding and the Use of Human Milk Pediatrics 2022150 e 202205798910.1542/peds.2022-05798935921641 · doi ↗ · pubmed ↗
- 7U.S. Department of Agriculture U.S. Department of Health and Human Services Dietary Guidelines for Americans, 2020–2025 U.S. Department of Agriculture Washington, DC, USA 2020
- 8World Health Organization (WHO) Breastfeeding Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_2(accessed on 20 December 2023)