Making Sense of Missense: Assessing and Incorporating the Functional Impact of Constitutional Genetic Testing
Meaghann Weaver

TL;DR
This paper explores the impact of diagnosing cancer predisposition syndromes in children and the psychosocial effects on families.
Contribution
The study introduces a systematic approach to include patient, parent, and provider perspectives in genetic testing for cancer predisposition.
Findings
Interviews revealed psychosocial themes relevant to genetic testing and diagnosis.
The study models the inclusion of multiple perspectives in familial cancer predisposition testing.
Findings suggest a need for longitudinal support for families receiving cancer predisposition diagnoses.
Abstract
What are the main findings? Assessing families for cancer predisposition syndromes is an increasingly common practice in pediatric oncology.Testing for cancer-predisposition syndromes in pediatric oncology enables cancer surveillance, helps tailor and inform cancer-directed treatments, and may assist in family risk assessment. Assessing families for cancer predisposition syndromes is an increasingly common practice in pediatric oncology. Testing for cancer-predisposition syndromes in pediatric oncology enables cancer surveillance, helps tailor and inform cancer-directed treatments, and may assist in family risk assessment. What is the implication of the main finding? Receiving a diagnosis of a cancer predisposition syndrome can be a complex experience with practical, existential, and psychosocial implications for patients and their families.Consideration should be given to each…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
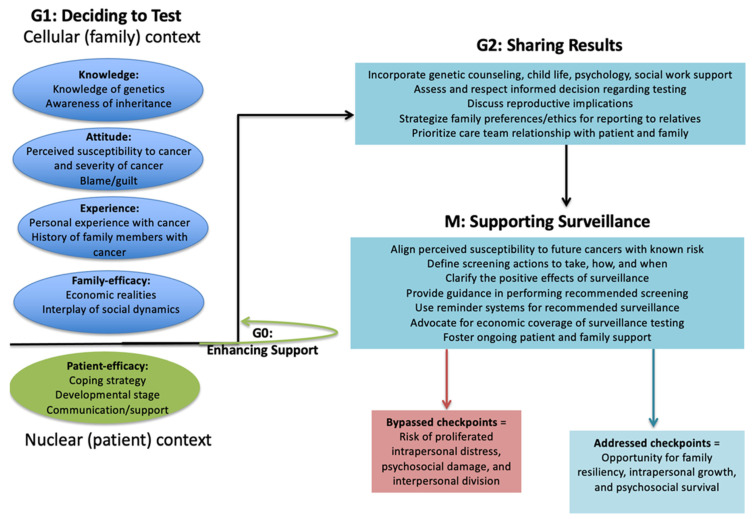 Figure 1
Figure 1- —Cancer Center Support (CORE)
- —National Institutes of Health
- —American Lebanese Syrian Associated Charities (ALSAC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLegal Systems and Judicial Processes
1. Introduction
A pre-teen male was diagnosed with acute myeloid leukemia after having been treated for localized osteosarcoma 5 years earlier. The family history contained a complex array of primary and secondary cancers in extended family members on the maternal line. The patient met Chompret criteria for Li–Fraumeni syndrome (LFS) and therefore underwent genetic testing for TP53 mutations. The patient harbored a TP53 mutation. His acute myeloid leukemia was recognized as high risk based on myelodysplastic features and 7q- and monosomy 5 karyotype, thereby expediting a bone marrow donor search. The patient’s mother and sister also had a TP53 mutation, thus excluding them from donating.
The tumor-suppressor gene TP53 represents a common denominator among human cancers [1]; therefore, the mechanism of TP53 action may serve as an analogy for an approach to genetic testing. With the emergence of accessible and affordable next-generation sequencing platforms, pediatric oncologists are now accountable to diligently ascertain the genetic causes of cancer with an amenable opportunity to test family members for cancer predisposition syndromes. The p53 protein guards the genome by regulating uncontrolled, hazardous cell division, thereby preventing harmful tumor formation. The clinical approach to testing for germline mutations may best be viewed as a guardian role—identifying individuals at risk of cancer and initiating tumor surveillance represents a protective extension of patient care. Just as p53 is in the cell nucleus, where it binds directly to DNA, pediatric oncologists attentively care for the child with cancer (“the nucleus”) while maintaining close therapeutic alliance with the patient’s family (“the cell”). TP53 encodes a transcription factor that is activated by cellular stress to minimize the propagation of harm [2]; therefore, the clinical team must approach constitutional genetic testing in a way that programmatically coordinates the antiproliferation of psychosocial stress, activation of support, and minimization of harm. Although recent evidence endorses tumor surveillance in pediatrics, this is not yet a universal practice [3,4]. Each individual and their family bring their own story and experiences, which motivate a methodological investment in eliciting narratives to guide future interventions for genetic testing, diagnosis, and overall care.
Receiving a cancer predisposition diagnosis is a life-altering experience that can compel a continuum of either negative factors of blame, guilt, and family instability or the positive factors of resilience, growth, and empowerment through knowledge. Concern about the psychological burden of genetic testing on families has been explored extensively in adult-onset cancer predisposition syndromes [5,6], but it is mostly speculative in pediatrics [7]. LFS models the destructive, divisive effects of accumulating damage; thus, families carrying germline TP53 mutations may experience a high risk of intrapersonal distress [8]. Although transient psychological anxiety may occur, long-standing, clinically significant distress need not be experienced when protective health delivery checkpoints are in place [9,10]. For genetic syndromes like LFS, with well-known medical benefits of strategic monitoring [3,4,11,12], the value of surveillance in the hope of detecting tumors at an early stage has been accompanied by a greater sense of control, security, and empowerment for families [13]. Caution should be contextually applied when discussing the perceived clinical benefits of surveillance, as those benefits may be more robust for some diagnoses (comprehensive LFS surveillance protocols) than others in which evidence is limited, lacking, or population-specific (e.g., founder variants in a particular geographical setting).
The relevance of genetic testing in this case was for personalized risk assessment and tailored treatment strategies. Psychosocial considerations included family counseling and cascade testing. The main research rationale was to determine how communication about cancer predisposition testing and diagnoses could improve prognostic understanding and enhance psychosocial adjustment to the news. Investigating patient- and family-specific motivations for and responses to genetic testing has the potential to translate into protective clinical checkpoints and improved psychosocial endpoints [14].
2. Materials and Methods
This qualitative study was developed through a protocol titled LiSTENING (Learning in Story: Elicited Narrative Informs Navigating Genetics). The Institutional Review Board at St. Jude Children’s Research Hospital approved this study under expedited categories, and informed consent was obtained from all study participants.
The LiSTENING protocol elicited patient and family narratives to inform interventions for genetic testing, diagnosis, and overall care. This qualitative approach mapped family members’ interpretation of their experience receiving a diagnosis of a germline TP53 mutation. This family-based qualitative case study enabled the study team to learn about potential psychosocial risks and benefits of genetic testing from a triangulated perspective of the patient, family, and care provider [15].
The family (n = 4 interviewed members) was recruited through study referral from the primary oncology clinic. The first approach included individual interpretations, as heard during family members’ recorded personal semi-structured interviews. The second approach included a collective perspective obtained through patient/parent/family semi-structured interviews. The bounded lens of this research was then interpreted through professional reflection with the multidisciplinary care providers. This approach enabled the acquisition of a detailed medical history, the social context, the chronology of events (both proximally and distally), and the interpretation of events from diverse vantage points [16]. Although the quantity of data gathered during interviews restricted its institutional implementation, targeted use of qualitative investigation enables teams to clarify themes and explore interpretations not readily accessible through quantitative methods [17,18].
This study followed strict qualitative investigation standards in study design (Appendix A.1) and implementation (Appendix A.2) [19]. Interview questions were first fielded by two qualitative research teams, one genetic counselor, one cancer psychologist, and were piloted on adult patients with cancer harboring a BRCA1 mutation (Appendix A.3). As a stakeholder participatory study, interviewees were given the opportunity to review and refine the interview transcripts prior to final data coding. Using an inductive approach to data analysis, interview words were used as the elements of data, and interview content was coded utilizing NVivo qualitative analysis software [20].
The field of genetics relies on meticulous coding; therefore, the interviews were attentively coded for social constructs. Coding reliability was ensured through inter-rater reliability (>94% for each domain), with differences in initial perspectives discussed until a consensus was reached. Social constructs were then interpreted into genetic language, thereby enabling social scientists and medical scientists to analyze and apply important themes via a shared language.
3. Results
Interview content revealed an opportunity to apply social themes analogous to TP53 biologic language (Table 1). Biological parents, one sibling, and one patient were offered the opportunity to participate in the qualitative interviews, as part of this in-depth original case study. The patient and parents emphasized the importance of the care team’s role to “check in” and elicit decisional preferences prior to each step in the diagnostic pathway: decision to undergo testing, receipt of results, and planning for surveillance. Before deciding about genetic testing, the family was asked to consider the ethical and relational aspects of disclosing test results to extended relatives.
Before testing, the care team had determined the family’s preferences for who would be present for conversations about the initial diagnosis. Because genetic findings would affect the person’s candidacy for bone marrow donor, each family member was pre-emptively encouraged to consider their coping with the test results, not as an isolated medical finding but as part of a larger care context. Thus, the team conducted conversations about testing, resulting, and monitoring prior to the testing to foster readiness. Mutated health system checkpoints could result in the proliferation of harm (e.g., testing without adequate partnership or preparation), or the other extreme––systematic blockage despite the potential benefits of genetic knowledge.
Comments to discourage genetic testing (“that’s so rare, it’s not worth testing,” or “most people don’t want to know”) were perceived by the family as imposing “selective pressure,” and yet they considered genetic testing a right and a responsibility. Regulatory checkpoints are best informed by clinical relations, as insight into family history and social context not only helps protect patients and families but also fosters safe progression toward the diagnosis of cancer predisposition syndromes.
The interviews revealed individual and collective stages of adjustment to the news of cancer predisposition, an adjustment equally important for framing the past and anticipating the future. The initial stress and shock of the diagnosis threatened personal growth arrest, requiring family members to individually and then collectively progress beyond the initial “devastation” into adjustment and acceptance. The family found strength in a unified interpersonal front, sharing poignant examples of aligning with one another (senescence) to face tensions and challenges. The theme of repair was depicted as repairing knowledge by correcting one another’s misinformation, repairing attitudes of guilt (carrier) and blame (noncarrier), and repairing perceptions that fear of a future cancer should steal today’s joys. Finding out about cancer predisposition was described as providing improved psychological adjustment to past loss, providing a new frame of reference for past events (frame shift).
The family history of multiple, concurrent cancer diagnoses and premature deaths was interpreted differently after germline discovery. The family’s imagination had previously leaned toward interpretations of loss as a scary and uncontrolled plight, whereas science now provided a cause that spoke reason to their past experience. Secret worries about what one family member termed a “mutant” or “freaky” extended family medical history could now be contained within a context of scientific explanation.
The most compelling insight gained during the interviews was the dominant theme of gain of function through genetic insight. Interviewees spoke of confidence and reduced uncertainty resulting from pre-symptomatic screening exams. Empowerment for advocacy, scientific knowledge, and validation of past suspicions were perceived as gains for older family members. Planning, self-knowledge, and early maturity were depicted as gains of functions for younger family members. The interviewees stated their goal of limiting the effect of cancer by discovering any future cancer early. For extended family members, monitoring was perceived as a gain of function, as targeted surveillance enabled them to believe cancer was now less likely “to sneak up, to surprise” them at an advanced stage.
By iteratively engaging with content from the interviews, the multidisciplinary study team formulated a conceptual model that supports patients and families through constitutional genetic testing (Figure 1). The figure applies the phases of a cell cycle to model a parallel psychosocial process for patients and families undergoing genetic testing. Genetic language translation helped connect the family’s lived narrative with the treatment team’s biomedical insights and the scientific team’s existing language. Genetic testing represents the science of medicine. Psychosocial engagement represents the art of medicine. Medicine merges science and art at the bedside. Translating genetic language into psychosocial principles fostered shared language as an opening for additional communication.
4. Discussion
This paper adds to the pediatric oncology literature by transforming the idea of cancer predisposition communication with families from a one-size-fits-all approach to a more precise, preventive, and family-centered discipline. The methods and findings from this paper demonstrate how cancer predisposition communication can inform treatment and support families.
Cancer predisposition testing warrants attention to ethical safeguards, beyond high-quality informed consent processes, that clearly communicate the purpose, benefits, risks, limitations, and alternatives to genetic testing; the voluntary nature of testing, free from coercion; and the right to withdraw or not receive test results. Additional ethics considerations include equitable access to genetic counseling before and after testing to review the implications, possible outcomes, and options, and to conceptualize the next steps after interpreting the test results. Protocols for providing emotional support to participants who receive distressing results should be part of a comprehensive care model.
Cancer predisposition results carry familial implications, which include not only the weight of self-determination but also the responsibilities associated with relational autonomy. Patients benefit from guidance on sharing relevant results with at-risk relatives, while also respecting their relatives’ individual autonomy. Ethical dilemmas arise in balancing patient confidentiality with the potential benefit of informing at-risk relatives. Therefore, ethics consultation services should be available and accessible in the setting of cancer predisposition testing. Cultural humility, fair access, and equity principles remain paramount to ensuring that the availability of cancer predisposition testing transcends economic barriers, while remaining tailored to cultural and linguistic needs. Privacy and confidentiality remain key health system ethics considerations with attentiveness to protecting data and disclosure. From a community perspective, legal protections that safeguard against genetic discrimination, in terms of insurance coverage and employment, have an increased importance in this era of genetic testing. Although cancer predisposition may be tested in one individual, the results of that testing have ethical implications across families; thus, psychosocial support needs are magnified.
This study explored the complex phenomena within one family, with specific attention to real-life contexts and contextual analysis. The methods included applying a biology metaphor to frame the psychosocial data. One limitation of metaphors is that they are used to compare unlike things, which can be ambiguous. Not all complex concepts, definitions, or arguments can be captured metaphorically, but metaphors can help foster understanding by illustrating such topics in a less complex way.
Subjective interpretation of the qualitative narrative risks researcher bias. Emotional recall, social desirability, and family dynamics risk participant bias, especially in the context of discussing sensitive genetic diagnoses. A limitation of this study was the single-site, single-family unit size, which prevents the generalizability of our findings. The in-depth, personalized engagement with the family demonstrated an exemplary approach for each family’s unique needs.
As pediatric oncology teams prepare to systematically approach genetic testing, there is an increasing, urgent need to gather the insight of those with lived experience. Understanding the nature of modifying effects, as well as the biological context in which they occur, has fostered new approaches aimed at controlling the clinical-biological impact of TP53 mutation [21]. Similarly, understanding genetic testing motivations and social context has the potential to promote innovative approaches to supporting clinical–social adjustments to cancer predisposition diagnoses.
The perspectives of those who have undergone cancer predisposition testing have the potential to teach care teams how to maximize psychosocial growth and minimize harm in the process. When DNA interfaces with potential harm, p53 plays an essential role in determining whether the DNA will be repaired or the organism will suffer. De-mystifying genetic testing, encouraging provider transparency, and unifying silos of interest are key to enabling clinical medicine to catch up with the speed at which potentially beneficial cancer predisposition data are being generated via next-generation sequencing. The first step to this end is the thoughtful inclusion of stakeholders’ perspectives, which may inform this era of genetic testing and speak sense to missense.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Junttila M.R. Evan G.I. p 53—A Jack of all trades but master of none Nat. Rev. Cancer 2009982182910.1038/nrc 272819776747 · doi ↗ · pubmed ↗
- 2Muller P.A. Vousden K.H. p 53 mutations in cancer Nat. Cell Biol.2013152810.1038/ncb 264123263379 · doi ↗ · pubmed ↗
- 3Villani A. Tabori U. Schiffman J. Shlien A. Beyene J. Druker H. Novokmet A. Finlay J. Malkin D. Biochemical and imaging surveillance in germline TP 53 mutation carriers with Li-Fraumeni syndrome: A prospective observational study Lancet Oncol.20111255956710.1016/S 1470-2045(11)70119-X 21601526 · doi ↗ · pubmed ↗
- 4Custodio G. Parise G.A. Kiesel Filho N. Komechen H. Sabbaga C.C. Rosati R. Grisa L. Parise I.Z. Pianovski M.A. Fiori C.M. Impact of neonatal screening and surveillance for the TP 53 R 337H mutation on early detection of childhood adrenocortical tumors J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol.2013312619262610.1200/JCO.2012.46.371123733769 PMC 3808236 · doi ↗ · pubmed ↗
- 5Meiser B. Psychological impact of genetic testing for cancer susceptibility: An update of the literature Psychooncology 2005141060107410.1002/pon.93315937976 · doi ↗ · pubmed ↗
- 6Gopie J.P. Vasen H.F. Tibben A. Surveillance for hereditary cancer: Does the benefit outweigh the psychological burden?—A systematic review Crit. Rev. Oncol./Hematol.20128332934010.1016/j.critrevonc.2012.01.00422366115 · doi ↗ · pubmed ↗
- 7Overby C.L. Tarczy-Hornoch P. Personalized medicine: Challenges and opportunities for translational bioinformatics Pers. Med.20131045346210.2217/pme.13.3024039624 PMC 3770190 · doi ↗ · pubmed ↗
- 8Lammens C.R. Aaronson N.K. Wagner A. Sijmons R.H. Ausems M.G. Vriends A.H. Ruijs M.W. van Os T.A. Spruijt L. Gomez Garcia E.B. Genetic testing in Li-Fraumeni syndrome: Uptake and psychosocial consequences J. Clin. Oncol.2010283008301410.1200/JCO.2009.27.211220479422 · doi ↗ · pubmed ↗