Association Between MMR Status and Prognostic Pathological Factors in Endometrioid Endometrial Cancer—A Single-Center Retrospective Study
Cezary Miedziarek, Hubert Bochyński, Katarzyna Bociańska, Michał Potograbski, Piotr Tyburski, Mikołaj Piotr Zaborowski, Ewa Nowak-Markwitz

TL;DR
This study explores how mismatch repair status affects the prognosis of endometrioid endometrial cancer, finding that dMMR tumors are more likely to have advanced disease and lymphovascular invasion.
Contribution
The study provides new evidence on the association between dMMR status and adverse prognostic features in endometrioid endometrial cancer.
Findings
dMMR tumors were more likely to present with advanced FIGO stage III/IV disease.
dMMR tumors showed a higher prevalence of lymphovascular space invasion.
No significant differences were found in tumor grade or receptor positivity between dMMR and pMMR groups.
Abstract
Clinical and pathological heterogeneity of endometrial carcinoma is not fully investigated, particularly in relation to mismatch repair (MMR) status. In practice, tumor profiles combining dMMR with adverse features may support therapy escalation, whereas favorable features support de-escalation. Identifying dMMR tumors has therapeutic relevance, guiding the consideration of immune checkpoint inhibitors. Previous studies have reported various findings regarding the impact of MMR deficiency, especially with respect to clinical progression of the disease, tumor grade, and the presence of adverse histopathological features such as lymphovascular space invasion (LVSI). By investigating these associations in our retrospective patient cohort, we aim to clarify the impact of MMR status on disease aggressiveness and to contribute evidence that may guide clinical decision-making. This study is…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
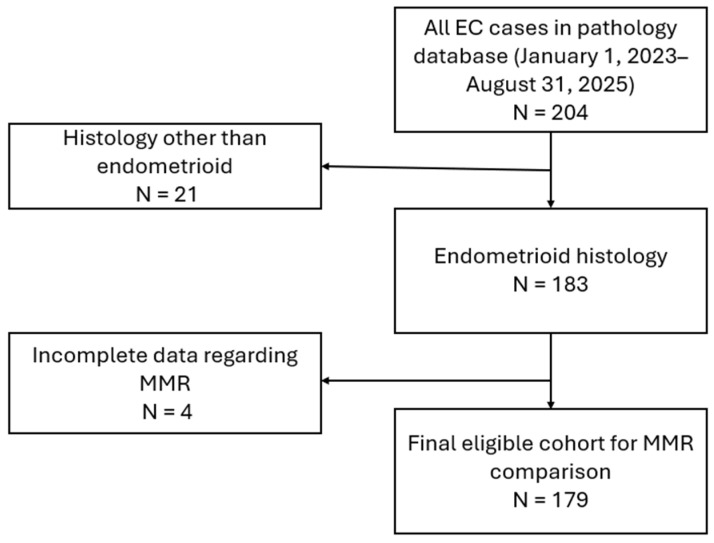 Figure 1
Figure 1- —Polish Minister of Science and Higher Education
- —PUMS doctoral students for 2025
- —Poznan University of Medical Sciences
- —Council of Scientific Colleges (Rada Kolegiów Nauk) of the Poznan University of Medical Sciences in Poznań
- —Development Foundation (Fundacja Rozwoju) of the Poznan University of Medical Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Gynecological conditions and treatments · Endometriosis Research and Treatment
1. Introduction
Endometrial cancer (EC) is a malignancy with a favorable prognosis. Considering all patients, the 5-year survival rate for this cancer is approximately 81% [1]. Prognostic assessment in EC depends on multiple clinical and pathological factors. The most important prognostic factors include histological tumor type, clinical stage of the disease, tumor grade, presence of lymphovascular space invasion (LVSI), and the presence of P53 gene mutations. Estrogen receptors (ER) and progesterone receptors (PR) positivity generally tracks with favorable biology and disease course, whereas receptor loss often coexists with adverse features [2,3].
The outcome of recent research on EC has been the identification of molecular subtypes of the disease, with practical implications. Based on The Cancer Genome Atlas (TCGA) analysis, EC has been molecularly classified into four subtypes: POLE ultramutated, microsatellite instability-high (MSI-H), copy-number low (CN-L), and copy-number high (CN-H) [4]. Accordingly, major guidelines incorporate molecular subtype into postoperative risk stratification and adjuvant therapy decisions (e.g., potential de-escalation for POLE ultramutated and escalation for TP53-mutated) [5]. Microsatellites are short repeats composed of a few nucleotides that are distributed throughout the genome. During DNA replication, errors can occur within these repeats. In normal cells, such errors are corrected by the DNA mismatch repair (MMR) system. When MMR is intact (pMMR), microsatellite length is preserved. When MMR is deficient (dMMR), errors accumulate, leading to microsatellite instability (MSI). In EC, tumors are therefore commonly classified as pMMR or dMMR, a distinction with important clinical implications, as dMMR/MSI-high tumors are particularly responsive to immune checkpoint inhibition [6,7,8]. Current guidelines endorse universal tumor testing for MMR deficiency in endometrial cancer, typically by MMR immunohistochemistry (IHC) with MSI testing (PCR or NGS) as an alternative or confirmatory approach [9]. On IHC, loss of MSH2, MSH6, or isolated PMS2 strongly suggests Lynch syndrome (LS) and directs germline testing toward the corresponding MMR gene, whereas MLH1 may also suggest sporadic MLH promoter hypermethylation (MLH1-PHM) with transcriptional silencing. Rare LS-like cases due to constitutional MLH1 methylation have been reported, but with limited need for genetic counseling, because they are not associated with heritable (germline) alterations [10]. Evidence linking MMR status to histopathologic aggressiveness in EC, including FIGO stage, LVSI, grade, and depth of invasion, remains inconsistent across studies. This knowledge gap motivates the comparison of pMMR and dMMR tumors using routinely reported pathologic features.
MMR status is a recognized predictor of response to immunotherapy in EC [6]. Consequently, scientific studies increasingly consider dMMR and pMMR populations as two distinct entities, requiring separate investigations due to their differences in treatment response. We hypothesized that dMMR tumors exhibit more aggressive pathological features, as they entail high mutational burden and a dysregulated immune microenvironment, alongside genomic instability [1,2,5]. The aim of the present study is to compare dMMR and pMMR EC patients with respect to the prevalence of pathological prognostic factors.
2. Materials and Methods
This retrospective study included patients treated for EC over a two-year period (1 January 2023–31 August 2025) at the authors’ affiliated institution. We enrolled patients consecutively, applying prespecified exclusions (non-endometrioid histology, missing core variables). The study was conducted at the Department of Gynecologic Oncology, Poznan University of Medical Sciences. The Bioethics Committee of Poznan University of Medical Sciences confirmed that, due to the retrospective nature of the study, no additional approval was required (Confirmation KB-655/25). The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Details of patient selection are presented in the flow chart (Figure 1).
The study included patients who were diagnosed with EC. Among these, only those with an endometrioid histopathological subtype (EEC) were analyzed. Histopathological diagnoses based on biopsy and postoperative specimens, surgical descriptions, and imaging studies were reviewed. Patients were divided into two main groups according to their MMR status, determined by immunohistochemical testing for the loss of expression of the MLH1, PMS2, MSH2, and MSH6 proteins: pMMR (proficient MMR) and dMMR (deficient MMR). Focal MMR loss was considered noninterpretable. We relied on unequivocally stained regions and repeated IHC as needed. Reproducible focal loss suggestive of clonal deficiency was flagged as suspicious for dMMR, prompted genetic testing [11], and revealed MSI-high in all such cases (n = 8). Patient data regarding tumor stage according to FIGO were collected, and for analysis purposes, patients were categorized into two groups: those with stage I and II disease and those with stage III and IV disease. Independently, patients with deep (≥50%) and superficial (<50%) myometrial invasion were identified. Tumors were also classified by grade into low-grade (G1 and G2) and high-grade (G3). LVSI status was considered positive if it was substantial or focal, and negative if it was absent. ER and PR status were defined according to the Allred score, where scores 0–2 were considered negative and scores 3–8 were considered positive [12]. Wild-type P53 (P53-wt) was defined as heterogeneous or variable nuclear staining with an internal control present. Aberrant (P53-abn) was defined by diffuse strong nuclear overexpression, complete absence of nuclear staining (null) with intact internal controls, or cytoplasmic staining with absent nuclear staining [13,14]. Mutation analysis of the POLE and TP53 genes was not performed using molecular methods, as these tests were not yet implemented in routine practice at the whole time of data collection. Additionally, in our center, immunohistochemical results for P53 generally correlate well with genetic mutation analysis. Antibodies used for ICH are presented in Table 1.
MSI assays were not available for all dMMR cases, particularly those from the early data collection period. However, in the tested cases (n = 34), all tumors were found to be MSI-high. Non-standard immunohistochemical patterns (e.g., isolated loss of a single MMR protein) prompted expedited referral for genetic counseling and evaluation for Lynch syndrome, as per institutional practice. These data are not included in the present study, which focuses on histopathologic determinants. It has to be noted that, as MSI assays were not available for all tumors and MMR status was determined by IHC, this approach can misclassify a minority of cases, e.g., those with non-standard immunohistochemical patterns.
Statistical analysis, including both descriptive and comparative methods, was conducted using Microsoft Excel and RStudio 2024.12.1. Group comparisons for categorical variables used chi-square or Fisher’s exact tests, as appropriate. For 2 × 2 tables, we additionally reported odds ratios (OR) with 95% confidence intervals calculated by Fisher’s exact method. Continuous variables were compared using the Mann–Whitney test and are summarized as median (IQR) with Hodges–Lehmann differences and 95% CI. Observations with missing data were excluded from bivariate analyses. We performed multivariable analyses for FIGO and LVSI (multivariable logistic regression with Wald tests). For the FIGO analysis, we excluded depth of myometrial invasion and LVSI, as these are elements of the staging definition. ER and PR status were also excluded due to substantial missing data and a significantly different proportion of missing values between the dMMR and pMMR groups (p = 0.0287, chi-square). For the LVSI analysis, we excluded FIGO (the FIGO classification incorporates LVSI) and ER and PR status due to the high proportion of missing data. We prespecified covariates and did not use stepwise selection. Complete case analysis, ORs with 95% CIs, and AUC are reported.
Missing data were handled by complete-case analysis for all inferential tests and models. ‘Unknown’ values were used only for descriptive summaries. We prespecified this approach to avoid ad hoc imputation and because of high rate of missingness for ER/PR data.
3. Results
The study group consists of 179 female patients (mean age 63.76 ± 10.43) with EC of the endometrioid histological subtype treated at our clinic. Selected epidemiologic factors—age, body weight and BMI—are summarized in Table 2. A total of 127 (70.95%) were classified as pMMR and 52 (29.05%) as dMMR. A detailed comparison of the two groups with respect to the analyzed parameters is presented in Table 3. The category “Unknown” is included for descriptive purposes only. For the analysis, we employed complete-case analysis, excluding observations with missing values in any variable included in a given model.
In bivariate tests, patients in the dMMR group were significantly more likely to be LVSI-positive compared with the pMMR group. Patients with dMMR tumors more frequently presented with FIGO stage III–IV disease. The groups did not differ significantly in histological grade, P53 status, estrogen receptor positivity, progesterone receptor positivity, and the prevalence of deep myometrial invasion. The groups were also comparable in terms of age, body weight, and BMI.
In a multivariable model (outcome: dMMR vs. pMMR) including FIGO, LVSI, grade, P53, and myoinvasion, FIGO III/IV was not significant: aOR = [1.95] (95% CI [0.72–5.25], p = 0.187). LVSI remained significant: aOR = [2.96] (95% CI [1.25–7.04], p = 0.014). It has to be noted, that the model showed modest discrimination (AUC = [0.646], 95% CI [0.546–0.735]) (Table 4).
In multivariate analysis, the presence of LVSI was independently associated with dMMR status (aOR [3.38], 95% CI [1.46–7.81]; p = 0.004). Additionally, it was associated with deep myometrial invasion (aOR [12.45], 95% CI [5.15–30.11]; p = <0.001, model discrimination: AUC = [0.807] (95% CI [0.743–0.867]). Advanced stage (FIGO III/IV) was independently associated with dMMR status (aOR [2.68], 95% CI [1.11–6.47]; p = 0.028). Additionally, it was associated with high histological grade (aOR [3.85], 95% CI [1.45–10.19]; p = [0.007]). Model discrimination: AUC = [0.709] (95% CI [0.604–0.811]) (Table 5 and Table 6).
An additional analysis was performed to evaluate the combinations of mismatch repair protein loss associated with dMMR. The most common pattern of absent expression on immunohistochemistry was combined loss of MLH1 and PMS2, which occurred in 78.8% of cases (Table 7).
4. Discussion
The dMMR population accounted for 29.05% of patients, which is consistent with previous reports indicating that this alteration occurs in approximately 25–30% of ECs [15,16]. It is worth noting that these analyses encompass all histopathological subtypes of EC. Nevertheless, the endometrioid subtype remains the most prevalent.
Data regarding the impact of MMR status on the clinical and pathological characteristics of EC remain inconclusive [17]. In our studied population, patients with EC and dMMR status were significantly more likely to present with a higher FIGO clinical stage and exhibited LVSI more frequently. It has to be noted that our results are associations and do not imply causation. Several studies have demonstrated an association between MMR status and the clinical stage of EC at diagnosis, where dMMR endometrial carcinomas are considered to exhibit a more aggressive clinical course [18]. In these studies, patients with dMMR EC are considered more likely to present with FIGO stage III or IV disease [19,20,21]. Moreover, they tend to have larger tumor size and a higher incidence of lymph node involvement, both of which are associated with advanced FIGO classification [19]. Reports also indicate a significantly lower prevalence of FIGO stage I disease among dMMR EC compared with pMMR tumors, with a relative shift toward stages II–IV [22]. On the other hand, several large studies have suggested that dMMR EC is more often present at lower tumor stages compared with MMR-proficient cases. Nonetheless, these reports consistently highlight that the dMMR subgroup more frequently exhibits metastatic parameters such as LVSI [17,23,24]. Given that dMMR cancers are more often associated with adverse clinicopathologic features, the implementation of immunotherapy is particularly valuable, especially in patients with advanced disease, as this subgroup derives the most significant benefit from immune checkpoint inhibition [18,25,26]. It is worth noting that differences in FIGO stage across studies may reflect heterogeneity in patient selection and IHC protocols, as well as variations in reporting schemes (e.g., stage I reported separately vs. pooling I + II as ‘early’ and III + IV as ‘advanced’). Differences in ethnic composition across referenced studies and the monoethnic nature of our cohort are also relevant to between-population comparisons.
LVSI is defined as the presence of malignant cells within lymphatic and/or vascular spaces. It represents an adverse prognostic factor in EC, being associated with lymph node metastasis, an increased risk of pelvic recurrence, and reduced overall survival. The impact is significant for both 3-year and 5-year survival rates, with the latter decreasing by 13–25% in LVSI-positive disease [27]. Women with dMMR tumors were more likely to have higher-grade cancers and more frequent LVSI [28], the latter consistent with our results.
Available analyses provide conflicting evidence regarding the association between tumor grade and MMR status. Some studies have demonstrated that high-grade tumors occur more frequently in the dMMR population, whereas others report them to be less common or similarly distributed, as observed in our cohort [28,29,30]. This inconsistency highlights the need for additional population-based studies in this area, particularly since tumor grade continues to be a key factor influencing therapeutic decision-making in early-stage disease [31].
Studies emphasize that in the majority of EEC, including dMMR tumors, estrogen and progesterone receptors are expressed, and P53 displays a wild-type pattern [32,33]. This is consistent with the findings of our analysis. Positive expression of estrogen and progesterone receptors, as well as the absence of TP53 mutations, represent favorable prognostic factors [34,35]. High-grade tumors constitute approximately 15–20% of endometrial cancers when a binary grading scheme is used. They are associated with worse clinical outcomes and more frequent adverse molecular alterations, including TP53 mutations [2]. The relationship between grade and the prevalence of ER/PR positivity remains controversial and varies across studies [34].
Additional analysis of immunohistochemistry patterns in dMMR EC cells reveals that the most prevalent phenotype is the loss of expression of both MLH1 and PMS2 proteins, accounting for approximately 70–80% of cases, which is in agreement with the outcomes from our own cohort. This reflects the instability of the PMS2 protein in the absence of its MLH1 partner [36,37]. The MSH2 and MSH6 co-loss is the second most common combination (15–20%), typically indicative of MSH2 mutations [26]. Less frequently, isolated MSH6 or PMS2 losses occur (5–10%), corresponding to mutations in the respective genes [38,39]. Interestingly, in our patient population, the second most common finding was isolated loss of single proteins, namely MSH6, MLH1, or MSH2, not MSH2 and MSH6 co-loss, which is considered a less common situation [27].
5. Limitations
A limitation of our study is the lack of genetic testing for POLE and TP53 mutations. The presence of POLE mutation represents an independent favorable prognostic factor in patients with endometrial carcinoma [40]. Genetic testing for TP53 mutations was also not included, as genetic assays were introduced into clinical practice after the initiation of data collection for this study. Furthermore, immunohistochemistry has been shown to correlate well with genetic testing for TP53 [41,42,43]. Therefore, it is unlikely that the omission of these analyses would have significantly affected our results.
However, in clinical practice, without POLE and TP53 sequencing, residual TCGA misclassification is possible. Favorable POLE-mutant and poor-prognosis TP53-aberrant tumors may be grouped solely based on clinical and pathological factors. While this analysis relied on IHC surrogates to show histologic features, full molecular profiling, including POLE and TP53 genetic testing, will be undertaken for any patient for whom it is expected to change clinical decision-making. This is important because POLE-ultramutated tumors (even with adverse histology such as LVSI or deep invasion) generally have an excellent prognosis and may warrant de-escalation of adjuvant therapy, whereas TP53-mutated tumors carry an unfavorable prognosis and often justify treatment escalation.
Although MMR IHC generally aligns well with MSI-high status in endometrial cancer, numerous studies have documented discordant cases. Therefore, the absence of MSI testing in every case should be regarded as a limitation.
As a single-center study, our cohort may reflect referral bias due to the case mix specific to our institution. It is limited by sample size, which may reduce precision and the generalizability of estimates. The benefit of a single-center design is histopathological consistency and uniform IHC.
6. Conclusions
EECs differ in their clinical and histopathological phenotypes depending on MMR status. Our findings are in line with reports indicating that dMMR tumors are characterized by a more aggressive clinical course and a higher prevalence of adverse histopathological features. In our cohort, this was reflected by a greater frequency of advanced FIGO stage and more common occurrence of LVSI in the dMMR group. These observations underscore the importance of adjuvant treatment, particularly immunotherapy, which has proven to be especially effective in this subset of patients. Future multicenter studies should integrate MMR status with comprehensive molecular profiling (POLE and TP53) to refine risk stratification and guide adjuvant therapy. Clinically, dMMR is a validated predictive biomarker for response to immune checkpoint inhibition, while LVSI is an established adverse prognostic feature. Together, these variables could support risk-adapted enrichment in immunotherapy trials, e.g., prioritizing dMMR tumors and considering dMMR with LVSI as a high-risk disease. Such strategies may increase event rates and therapeutic signal detection while aligning with routine pathology workflows. Prospective, biomarker-driven trials with standardized staging and pathology review are needed to confirm their benefits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tejerizo-GarcíaÁ. Jiménez-López J.S. Muñoz-González J.L. Bartolomé-Sotillos S. Marqueta-Marqués L. López-González G. Gómez J.F.P.-R. Overall Survival and Disease-Free Survival in Endometrial Cancer: Prognostic Factors in 276 Patients Onco Targets Ther.201361305131310.2147/ott.s 5153224092993 PMC 3787927 · doi ↗ · pubmed ↗
- 2Coll-de la Rubia E. Martinez-Garcia E. Dittmar G. Gil-Moreno A. Cabrera S. Colas E. Prognostic Biomarkers in Endometrial Cancer: A Systematic Review and Meta-Analysis J. Clin. Med.20209190010.3390/jcm 906190032560580 PMC 7356541 · doi ↗ · pubmed ↗
- 3Wang X. Aziz A.u.R. Wang D. Wang Y. Liu M. Yu X. Wang D. Prognostic Factors and Survival Outcomes of Immunohistochemically Detection Based-Molecular Subtypes of Endometrial Cancer–Analysis of 576 Clinical Cases Diagn. Pathol.20241916210.1186/s 13000-024-01584-039707379 PMC 11660601 · doi ↗ · pubmed ↗
- 4Cancer Genome Atlas Research Network Kandoth C. Schultz N. Cherniack A.D. Akbani R. Liu Y. Shen H. Robertson A.G. Pashtan I. Shen R. Integrated Genomic Characterization of Endometrial Carcinoma Nature 2013497677310.1038/nature 1211323636398 PMC 3704730 · doi ↗ · pubmed ↗
- 5Galant N. Krawczyk P. Monist M. Obara A. GajekŁ. Grenda A. NicośM. Kalinka E. Milanowski J. Molecular Classification of Endometrial Cancer and Its Impact on Therapy Selection Int. J. Mol. Sci.202425589310.3390/ijms 2511589338892080 PMC 11172295 · doi ↗ · pubmed ↗
- 6Corr B. Cosgrove C. Spinosa D. Guntupalli S. Endometrial Cancer: Molecular Classification and Future Treatments BMJ Med.20221 e 00015210.1136/bmjmed-2022-000152 PMC 997876336936577 · doi ↗ · pubmed ↗
- 7Adorisio R. Troncone G. Barberis M. Pepe F. Molecular Profiling of H-MSI/d MMR/for Endometrial Cancer Patients: “New Challenges in Diagnostic Routine Practice”J. Mol. Pathol.2024518719810.3390/jmp 5020012 · doi ↗
- 8Paranjpe R. Chen C. Sun Y. Hong J. Prabhu V.S. Ojha J. Meng R. Duska L.R. Molecular Heterogeneity in d MMR/MSI-H Endometrial Cancer in the USJ. Clin. Oncol.202543 e 1764310.1200/JCO.2025.43.16_suppl.e 17643 · doi ↗