Prognosis Prediction Model After Upfront Surgery for Resectable Pancreatic Ductal Adenocarcinoma: A Multicenter Study (OS-HBP-2)
Kosei Takagi, Ryuichi Yoshida, Kazuya Yasui, Masayoshi Hioki, Takehiro Okabayashi, Toru Kojima, Yoshikatsu Endo, Daisuke Nobuoka, Kenta Sui, Masaru Inagaki, Susumu Shinoura, Masashi Kimura, Tatsuo Matsuda, Hideki Aoki, Toshiyoshi Fujiwara

TL;DR
This study developed a model to predict survival after surgery for resectable pancreatic cancer, validated using data from 603 patients across multiple centers.
Contribution
A novel internally validated prognosis prediction model for overall survival after surgery in resectable pancreatic ductal adenocarcinoma patients.
Findings
The 1-, 3-, and 5-year overall survival rates were 83.7%, 48.2%, and 37.5%, respectively.
Key predictors of survival included tumor size, vascular contact, CA19-9 levels, and the modified Glasgow Prognostic Score.
The model showed an area under the curve of 0.68 and a concordance index of 0.63.
Abstract
Although several prognostic nomograms have been developed to estimate the prognosis of patients with pancreatic ductal adenocarcinoma (PDAC), further investigation is re-quired to optimize the prognostic assessment tools for patients with resectable PDAC. This multicenter study (n = 603) aimed to investigate the prognostic factors for survival and develop a prognosis prediction model after upfront surgery in patients with resectable PDAC. Using the results of the multivariate analyses, a prognosis prediction model for overall survival was constructed. This study suggests that our model may be useful and can be internally validated for predicting overall survival following upfront surgery in patients with resectable PDAC. Background/Objectives: Upfront surgery (UFS) remains the standard treatment for patients with resectable pancreatic ductal adenocarcinoma (PDAC). We aimed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
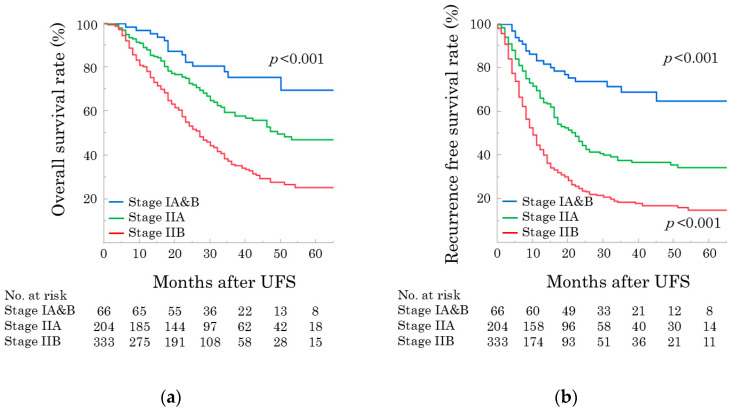 Figure 1
Figure 1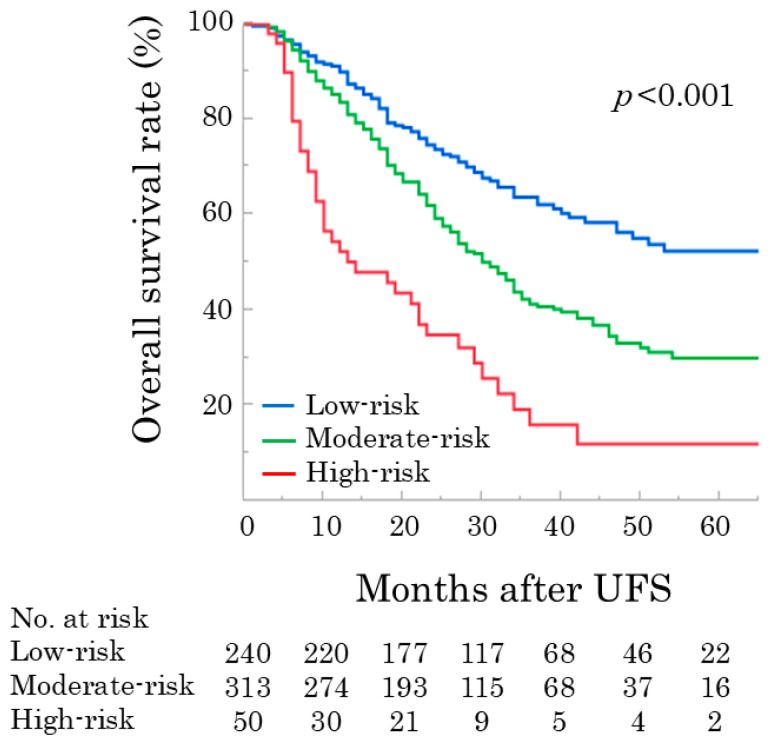 Figure 2
Figure 2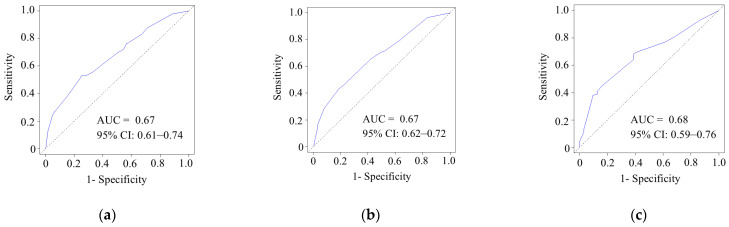 Figure 3
Figure 3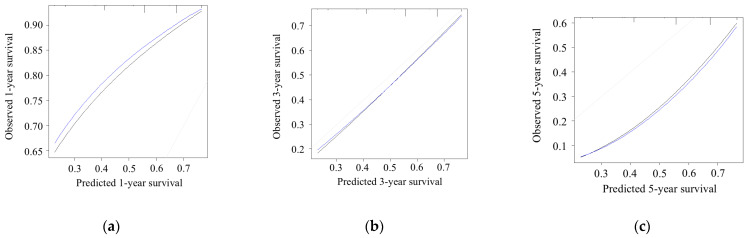 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cholangiocarcinoma and Gallbladder Cancer Studies · Esophageal Cancer Research and Treatment
1. Introduction
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most lethal malignancies with a poor survival rate [1,2]. Currently, the importance of resectability is emphasized when determining the treatment strategies for PDAC [3]. The National Comprehensive Cancer Network guidelines categorize resectability status as resectable, borderline resectable, or unresectable, and propose appropriate workups and treatment options based on patient presentation, cancer type, and disease stage [4]. Upfront surgery (UFS) is recommended for patients with resectable PDAC without high-risk features such as large primary tumors, enlarged regional lymph nodes, and markedly elevated carbohydrate antigen 19-9 (CA 19-9) levels [4]. However, despite recent developments in multidisciplinary treatments for PDAC, prognosis after resection remains poor [5].
Numerous efforts have been made to identify prognostic factors and estimate the prognosis of patients with PDAC [6]. Several prognostic nomograms have been developed and incorporate patient characteristics, tumor factors, and tumor markers [7,8,9]. Moreover, the impact of various nutritional and inflammatory assessment tools, including the modified Glasgow Prognostic Score (mGPS) and prognostic nutritional index, on PDAC has been investigated [10]. However, because the resectability status is evaluated based on radiologic anatomical findings [4], varying degrees of malignancy can be categorized within the same resectability group. Therefore, resectability-specific risk factors should be investigated to optimize prognostic assessment tools for PDAC. Models for predicting early recurrence and preoperative lymph node metastasis have been developed for resectable PDAC [11,12,13]. However, few studies have developed prognostic prediction models for the survival of patients with resectable PDAC.
This multicenter study investigated long-term outcomes and prognostic factors for survival after UFS in patients with resectable PDAC. In addition, a prognostic prediction model was developed. This study was conducted as part of the Okayama Study Group for Hepato-Biliary-Pancreatic Surgery (OS-HBP-2).
2. Materials and Methods
2.1. Study Cohort
This was a multicenter retrospective study, including 647 patients who underwent UFS for resectable PDAC between January 2013 and December 2017. Clinical data were collected from the OS-HBP [14]. The study was approved by the Ethics Committee of our institution (approval no. 2211-039) and conducted in accordance with the principles outlined in the Declaration of Helsinki. Due to the retrospective nature of this study, the requirement for informed consent was waived.
2.2. Clinical Data
Using the anonymous database, we extracted the following data: age, sex, body mass index, biliary drainage, laboratory values including tumor markers, mGPS [15], preoperative radiological findings (tumor location, tumor size, venous involvement, and lymph node metastasis), preoperative clinical findings were classified according to the Unio Internationalis Contra Cancrum (UICC)/American Joint Committee on Cancer (AJCC) seventh edition [16,17], type of procedure (pancreaticoduodenectomy, distal pancreatectomy, or total pancreatectomy), operative factors, pathological factors, including R0 and R1 classification [18]) evaluated by the UICC/AJCC seventh edition [16,17], major complications (Clavien–Dindo classification; ≥grade 3 [19]), postoperative pancreatic fistula (≥grade B [20]), adjuvant chemotherapy, and long-term outcomes (recurrence and status at last follow-up [survival or death]).
Preoperative radiological findings and the initial resectability status were evaluated using computed tomography scans at a multidisciplinary conference. The following criteria for resectable PDAC, based on the National Comprehensive Cancer Network criteria, were used: no tumor contact with major arterial structures (celiac artery, superior mesenteric artery, and/or common hepatic artery) and no tumor contact with the portal vein (PV) or superior mesenteric vein (SMV), with ≤180° contact without vein contour irregularity [4]. Venous involvement was categorized as no tumor contact with the PV or SMV or tumor contact with the PV or SMV of ≤180° in this study [21]. Using C-reactive protein and serum albumin levels, patients were classified as having an mGPS of zero, one, or two [15]. The following cutoff values of CA 19-9 were used: 40 U/mL, normal range; and 500 U/mL, biologically borderline resectable [22]. As CA19-9 levels can be significantly influenced by biliary obstruction, we selected preoperative CA19-9 levels recorded after biliary drainage for this study. Pathological stages were defined using the criteria of the AJCC seventh edition criteria [17]. The definition of R0 resection in this study included the margin edge being free based on the closest margin among all resection margins. Adjuvant chemotherapy included either S-1 or gemcitabine administered 6 months after surgery [23].
2.3. Statistical Analysis
All statistical analyses were performed using EZR software (version 1.65; Saitama Medical Center, Jichi Medical University, Saitama, Japan) and the JMP (version 11; SAS Institute, Cary, NC, USA). Categorical variables were presented as proportions, and continuous variables were presented as medians with interquartile ranges (IQRs). Differences between groups were assessed using either Fisher’s exact test or the chi-square test for categorical variables and the Mann–Whitney U test for continuous variables. All reported p-values were two-tailed, with an alpha level of 0.05 considered statistically significant.
The overall survival (OS) and recurrence-free survival (RFS) were calculated using the Kaplan–Meier method. Overall survival (OS) was defined as the time interval between surgery and death from any cause, whereas RFS was defined as the time from surgery to recurrence or death from any cause. Univariate and multivariate analyses were performed using the Cox proportional hazards model to identify the prognostic factors for OS. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated.
A simple scoring model was developed based on multivariate analyses, with one point assigned to each prognostic factor, demonstrating a similar HR. Thereafter, patients were divided into several groups according to the identified prognostic factors. Another prognostic prediction model was developed to predict the OS using multivariate analysis. Using the area under the receiver operating characteristic curve (AUC), the performance of the model was evaluated. Subsequently, the bootstrap method was used for internal validation to assess the discriminative performance of the model [24]. The predictive validity of the model was evaluated by analyzing the calibration curve and concordance index (C-index).
3. Results
3.1. Cohort
Among the 647 patients, 603 were included after excluding 44 patients who were Lewis-negative (n = 41) and those with postoperative in-hospital mortality (n = 3). The characteristics of 603 patients are shown in Table 1. Of 603 patients, 210 (34.8%) underwent biliary drainage. Median CA19-9 level was 111 U/mL (IQR 30–392 U/mL), and preoperative total bilirubin was within the normal range of 0.8 mg/dL (IQR 0.6–1.3 mg/dL).
Tumor locations were the pancreatic head (n = 393, 65.2%) and pancreatic body and tail (n = 210, 34.8%), with a median tumor size of 2.3 cm (IQR 1.8–3.0 cm). Tumor contact with a PV or SMV of ≤180° was confirmed in 174 (28.9%) patients. The procedures included pancreaticoduodenectomy (n = 387, 64.2%), distal pancreatectomy (n = 198, 32.8%), and total pancreatectomy (n = 18, 3.0%). Regarding pathological findings, 331 (54.9%) patients had lymph node metastases. R0 resection was achieved in 532 (88.2%) patients.
During the follow-up period of 25 months (IQR, 15–38 months), 381 (63.2%) patients experienced recurrence. The median OS and RFS after UFS were 34 months and 15 months, respectively. The 1-, 3-, and 5-year OS rates were 83.7%, 48.2%, and 37.5%, respectively. The 1-, 3-, and 5-year RFS rates were 55.1%, 30.7%, and 27.1%, respectively. The Kaplan–Meier curves for OS and RFS stratified by pathological stage are shown in Figure 1. The 5-year OS rates were 69.7%, 47.1%, and 25.4% for pStages IA and IB and pStage IIA and pStage IIB, respectively (Figure 1a). The 5-year RFS rates were 64.9%, 34.5%, and 15.1% for pStages IA and IB and pStage IIA and pStage IIB, respectively (Figure 1b).
3.2. Prognostic Factors Associated with OS
The results of the univariate and multivariate analyses are presented in Table 2. Multivariate analyses identified four independent predictors associated with OS: tumor size > 2 cm (hazard ratio [HR] 1.50, p = 0.001), tumor contact with the PV and SMV of ≤180° (HR 1.47, p = 0.003), CA 19-9 40–500 U/mL (HR 1.59, p = 0.002) and ≥500 U/mL (HR 2.16, p < 0.001), and mGPS of two (HR 1.56, p = 0.038).
3.3. Simple Scoring Model for OS Following UFS
A simple scoring model was developed for all patients, with one or two points assigned to each independent predictor: tumor size > 2 cm (one point), tumor contact with the PV and SMV (one point), CA 19-9 40–500 U/mL (one point) and >500 U/mL (two points), and mGPS of two (one point). The patients were categorized into three groups based on these scores: low risk (0–1 point; n = 240), moderate risk (2–3 points; n = 313), and high risk (4–5 points; n = 50). The clinicopathological characteristics stratified by risk group are shown in Table 3. The high-risk group exhibited the most advanced tumor characteristics. However, no significant differences were observed between the groups in terms of R status, incidence of major complications, or use of adjuvant chemotherapy. The incidence of postoperative recurrence in the low-, moderate-, and high-risk groups was 47.9%, 71.6%, and 84.0%, respectively (p < 0.001).
The OS curves for these groups showed overall 3- and 5-year survival rates of 63.8% and 52.4% in the low-risk group, 41.4% and 30.1% in the moderate-risk group, and 16.1% and 12.1% in the high-risk group (log-rank p < 0.001) (Figure 2). The OS curves for these groups showed overall 3- and 5-year survival rates of 63.8% and 52.4% in the low-risk group, 41.4% and 30.1% in the moderate-risk group, and 16.1% and 12.1% in the high-risk group, respectively (log-rank p < 0.001) (Figure 2).
3.4. Prognosis Prediction Model for OS Following UFS
Using the results of multivariate analyses, the predictive probability of the model for OS was constructed (Equation (1); available in Supplementary Digital Content S1):
3.5. Model Performance and Calibration
Calibration plots of the predictive model for 1-, 3-, and 5-year OS are shown in Figure 3. The AUCs for 1-, 3-, and 5-year OS were 0.67 (95% CI, 0.61–0.74), 0.67 (95% CI, 0.62–0.72), and 0.68 (95% CI, 0.59–0.76), respectively.
The predicted probability of OS was moderately correlated with the actual likelihood, with a C-index of 0.63 (Figure 4).
3.6. A Literature Review
A PubMed literature search was conducted to identify articles that developed nomograms to predict postoperative survival after surgery in patients with PDAC. Table 4 summarizes the 10 relevant articles, including our study [7,8,9,25,26,27,28,29,30]. The study designs included single-center (n = 5), multicenter (n = 2), and database (n = 3) studies. Previously published nomograms targeted PDAC resection. The C-index ranged from 0.63 0.79.
4. Discussion
Although UFS has been recognized as the standard of care for patients with resectable PDAC [4], the prognosis remains poor, even in resectable PDAC, probably because of incomplete resection and early postoperative recurrence [31]. In this multicenter retrospective study, we investigated long-term outcomes and preoperative prognostic factors associated with OS after UFS in 603 patients with resectable PDAC. Multivariate analyses identified tumor size, tumor contact with the PV and SMV of ≤180°, CA 19-9 level, and mGPS as independent predictors of OS. Moreover, a prognostic prediction model was developed to estimate OS following UFS for patients with resectable PDAC, and its performance was evaluated using internal validation. To the best of our knowledge, this is the first multicenter study to demonstrate a prognostic prediction model for OS after UFS in patients with resectable PDAC.
Long-term outcomes after UFS in this study, including median OS and RFS of 34 months and 15 months, were relatively better compared with those of previous reports, which reported median OS and RFS of 18.8 (95% CI 12.4–20.6) months and 9 (95% CI 1.6–12.5) months [32]. This improvement might be due to the higher R0 resection and induction rates of adjuvant chemotherapy in this study [32]. However, approximately 60% of patients experienced recurrences. Therefore, further efforts are required to improve the long-term outcomes based on potential risk factors.
Several preoperative factors, including tumor size, tumor contact with the PV and SMV of ≤180°, CA 19-9 level, and mGPS, were identified as prognostic factors associated with OS in this study. Previous studies reporting prognostic nomograms found that tumor size is a predictive parameter for prognosis [7,33]. Our novel finding is that preoperative radiological venous involvement, tumor contact with the PV&SMV of ≤180°, is a prognostic factor for OS. Since venous involvement can be divided into no tumor contact and tumor contact with the PV or SMV [21], we found that no tumor contact and tumor contact with the PV or SMV represented distinctly different risk factors for survival in patients with resectable PDAC. Portomesenteric venous tumor contact is reportedly associated with poor OS, high rates of R1 resection, and lymph node metastasis in patients with resectable PDAC following UFS [34]. CA 19-9 is regarded as an effective predictor of OS, nodal involvement, and margin status after surgery in patients with resectable PDAC [35,36]. A meta-analysis demonstrated that mGPS, a promising inflammatory prognostic indicator, is closely associated with PDAC [37].
Prognostic prediction models for OS were constructed using the results of multivariate analyses. In the simple scoring model, survival curves were stratified according to the risk scores (Figure 2). The postoperative survival probability (%) was calculated using a prognosis prediction model (Equation (1)). Regarding model performance and internal validity, the model’s performance, with an AUC of 0.67 to 0.68, was satisfactory. The calibration plots demonstrated relatively good agreement, with a C-index of 0.63. Because preoperative factors were selected to establish these prognostic prediction systems, we could estimate patient survival preoperatively. Therefore, the potential clinical implications of this model include the survival risk stratification of patients with resectable PDAC.
As shown in Table 3 and Figure 2, the OS and recurrence rates in the moderate- and high-risk groups were significantly lower than those in the low-risk group. Our results suggest that resectable PDAC should not be categorized solely by resectability status but rather subcategorized using various clinical factors, and appropriate multidisciplinary treatments, including neoadjuvant and adjuvant chemotherapy, should be provided. Although the role of neoadjuvant chemotherapy in resectable PDAC remains controversial, our prognostic prediction models may be useful for identifying high-risk groups that may benefit from intensified multidisciplinary care. Considering the growing evidence for neoadjuvant treatments for resectable PDAC, neoadjuvant chemotherapy may improve oncological outcomes and survival, especially in patients with high-risk features of resectable PDAC [38,39,40]. Moreover, evidence for adjuvant therapy for PDAC is well established [23,41,42,43]. The primary rationale behind the use of neoadjuvant and adjuvant therapies in pancreatic cancer is to target and destroy occult micrometastatic disease, which is believed to be the leading cause of early and frequent disease recurrence after curative surgery [44]. Accordingly, a perfect clinical course, including neoadjuvant chemotherapy, surgery, and adjuvant therapy, may be the ultimate protocol for improving outcomes, especially in moderate- and high-risk groups [40].
Several novel findings of our model compared to previous nomograms are summarized in Table 4. As previous models targeted resected PDAC, our model focused only on patients with resectable PDAC. The prognostic factors for survival differ depending on the resectability status. Therefore, the resectability-specific prediction model was reasonable. Moreover, existing nomograms include postoperative parameters such as pathological findings that cannot be assessed preoperatively. In contrast, our model included only preoperative factors. Therefore, we could estimate patient survival preoperatively and construct treatment strategies depending on the risk categories.
The present study had several limitations. Although this was a multicenter study with a relatively large sample size, its retrospective nature may have introduced a potential selection bias in surgical decision-making across centers and limited the causality of the findings. Using multivariate analysis, we identified independent preoperative predictors associated with OS. However, other confounding or residual confounding factors may exist. The discriminative performance of the prognostic prediction model was investigated using internal validation. However, the moderate performance of the prediction model may be a limitation. Moreover, an external validation was not performed to verify the reliability and generalizability of the model. Because external validation is crucial to ensure the model’s applicability in different populations, the lack of external validation of the prediction model is a significant limitation. Future studies should conduct external validations to confirm the applicability of this model.
5. Conclusions
The present study demonstrated long-term outcomes and identified preoperative prognostic factors of survival, including tumor size, tumor contact with the PV and SMV of ≤180°, CA 19-9 level, and mGPS, in patients who underwent UFS for resectable PDAC. Moreover, we developed a prognostic prediction model to estimate the OS after UFS for resectable PDAC. Our model may be useful and internally validated for predicting OS after UFS. Intensive multidisciplinary treatment may be required in high-risk patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li T. Lin C. Wang W. Global, regional, and national burden of pancreatic cancer from 1990 to 2021, its attributable risk factors, and projections to 2050: A systematic analysis of the global burden of disease study 2021 BMC Cancer 20252518910.1186/s 12885-025-13597-z 39901108 PMC 11789343 · doi ↗ · pubmed ↗
- 2Siegel R.L. Kratzer T.B. Giaquinto A.N. Sung H. Jemal A. Cancer statistics, 2025 CA Cancer J. Clin.202575104510.3322/caac.2187139817679 PMC 11745215 · doi ↗ · pubmed ↗
- 3Sarma G. Bora H. Medhi P.P. Optimizing neoadjuvant chemoradiation in resectable and borderline resectable pancreatic cancer: Evidence-based insights World J. Clin. Oncol.20251610610710.5306/wjco.v 16.i 7.10610740741196 PMC 12305107 · doi ↗ · pubmed ↗
- 4National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma (Version 2.2025)National Comprehensive Cancer Network Plymouth Meeting, PA, USA 2025
- 5Yoon S.J. Shin S.H. Yoon S.K. Jung J.H. You Y. Han I.W. Choi D.W. Heo J.S. Appraisal of 5-year recurrence-free survival after surgery in pancreatic ductal adenocarcinoma J. Hepato-Biliary-Pancreat. Sci.20212828729610.1002/jhbp.81532790012 · doi ↗ · pubmed ↗
- 6Allen P.J. Kuk D. Castillo C.F. Basturk O. Wolfgang C.L. Cameron J.L. Lillemoe K.D. Ferrone C.R. Morales-Oyarvide V. He J. Multi-institutional Validation Study of the American Joint Commission on Cancer (8th Edition) Changes for T and N Staging in Patients With Pancreatic Adenocarcinoma Ann. Surg.201726518519110.1097/SLA.000000000000176327163957 PMC 5611666 · doi ↗ · pubmed ↗
- 7Yoon S.J. Park B. Kwon J. Lim C.S. Shin Y.C. Jung W. Shin S.H. Heo J.S. Han I.W. Development of Nomograms for Predicting Prognosis of Pancreatic Cancer after Pancreatectomy: A Multicenter Study Biomedicines 202210134110.3390/biomedicines 1006134135740364 PMC 9220008 · doi ↗ · pubmed ↗
- 8Zhuang H. Zhou Z. Ma Z. Huang S. Gong Y. Li Z. Liu C. Wang S. Chen B. Zhang C. Prognostic Nomogram for Patients With Pancreatic Ductal Adenocarcinoma of Pancreatic Head After Pancreaticoduodenectomy Clin. Med. Insights Oncol.2021151179554921102414910.1177/1179554921102414934211308 PMC 8216341 · doi ↗ · pubmed ↗