The Preoperative Prognosticators of Surgical Margins (R0 vs. R1) in Pelvic Exenteration—A 14-Year Retrospective Study from a Tertiary Referral Centre
Sabina Ioana Nistor, Roman Mykula, Richard Bell, William Gietzmann, Mahmoud Awaly, Alaa Elzarka, Jennifer Thorne, Jacopo Conforti, Federico Ferrari, Nicholas Symons, Hooman Soleymani majd

TL;DR
This study identifies factors that help predict successful cancer removal during a complex pelvic surgery for gynaecological cancers.
Contribution
The study provides new insights into preoperative predictors of achieving R0 resection in pelvic exenteration after radiotherapy.
Findings
R0 resection was achieved in 77.8% of patients undergoing pelvic exenteration.
Younger age, cervical cancer origin, and smaller tumor size were associated with better resection outcomes.
Intraoperative and postoperative complications occurred in nearly one-third and one-fifth of cases, respectively.
Abstract
Pelvic exenteration is one of the most extensive operations performed for gynaecological cancers that return or persist after radiotherapy. It involves removing the cancer along with nearby pelvic organs, followed by reconstructive surgery. The main aim is to achieve “R0 resection,” meaning all visible and microscopic cancer is removed, which offers the best chance of long-term survival. We looked at 27 women who had surgery at Oxford University Hospitals between 2011 and 2024, after radiotherapy. Their cancers started in the cervix, uterus, vagina, or vulva. The average age was 63. Surgeons achieved complete removal in almost 80% of cases. Complications happened during surgery in about one in three women, and serious post-surgery problems in about one in five. Younger patients, with smaller tumour size, and those with cervical cancer and reduced blood loss during surgery were more…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
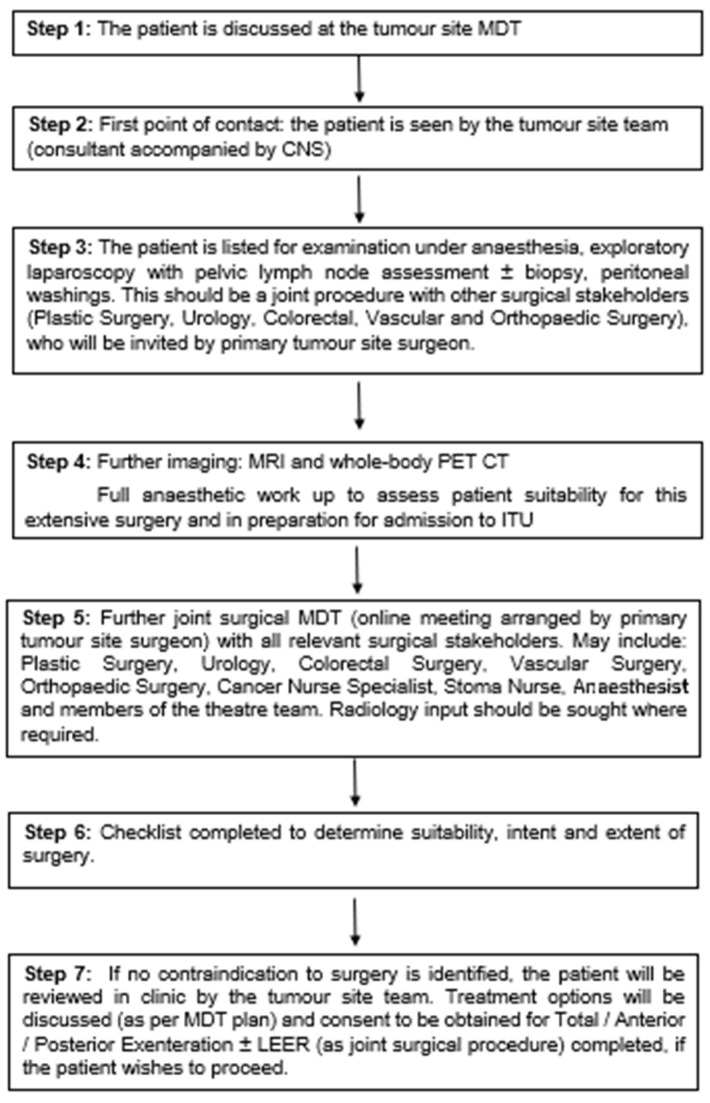 Figure 1
Figure 1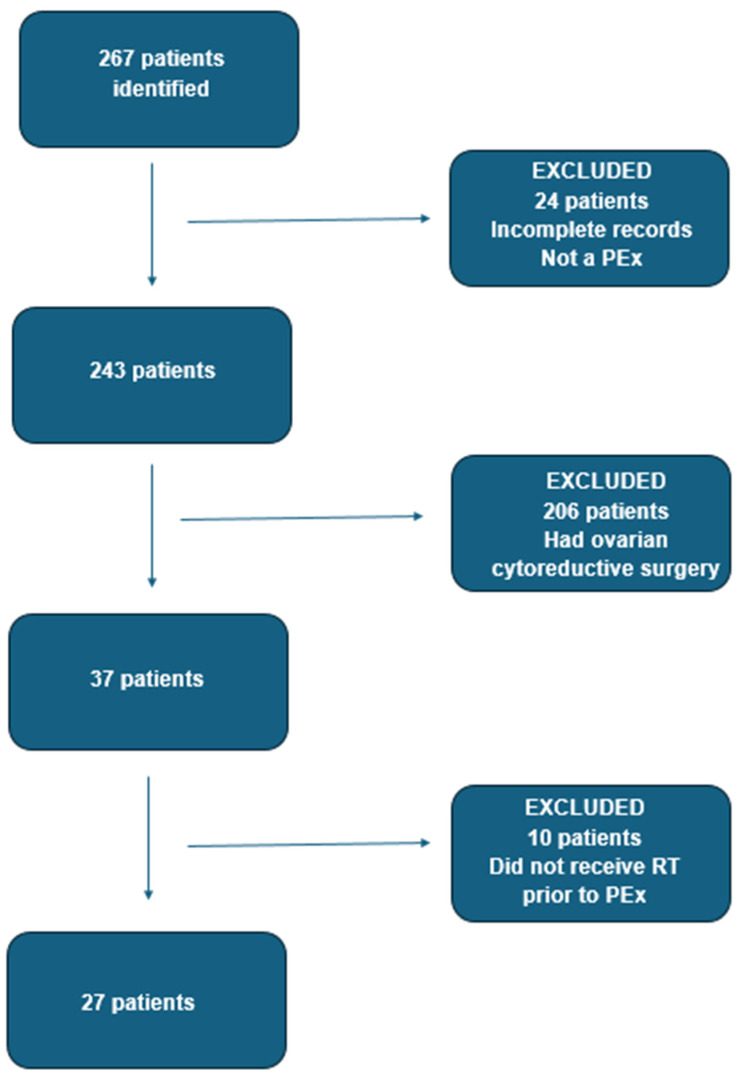 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Colorectal and Anal Carcinomas · Reconstructive Surgery and Microvascular Techniques
1. Introduction
Pelvic exenteration (PEx) is a complex surgery considered for locally advanced or recurrent pelvic malignancies, entailing a radical en-block resection of multiple adjacent pelvic organs, followed by reconstructive surgery.
It was first described by Alexander Brunschwig in 1948 as a palliative procedure for recurrent cervical cancer [1]. Mortality rates of PEx have reduced from 23% in Brunschwig’s series to 1.7% in modern series [2], while the reported 5-year overall survival range is 32–70% for gynaecological malignancies [3,4,5], making these procedures “curative” and acceptable for well-selected patients.
Modifications of the surgical technique have extended the en-block resection to include, in addition to pelvic organs, adjacent structures such as pelvic sidewall muscles, nerves and major vessels [6,7,8], or bony structures (composite exenterations) [9,10,11], in an attempt to obtain complete resection with negative margins (achieve R0).
Compelling evidence supports the importance of achieving R0 resection, the Achilles heel of pelvic exenteration, which is associated with improved disease-free survival [12,13,14,15,16,17] and overall survival [4,12,14,15,16,17,18].
A retrospective cohort including 1293 patients from 22 centres undergoing PEx for non-colorectal malignancies, 523 of them gynaecological, demonstrated that R0 resection was the main factor associated with long-term survival in multivariate analysis. The 3-year overall survival rates for patients having R0 resection for advanced or recurrent endometrial, ovarian, cervical, or vaginal malignancy were 48%, 40.6%, 49.4%, and 43.8%, respectively, while R1 and R2 resections had significantly lower overall survival: 22.2%, 30.3%, 37%, and 12.5%, respectively [2].
Palliative exenteration remains a controversial practice, given the high rates of associated morbidity in patients with a limited overall survival [19], as well as a doubtful palliation benefit [14]. Quyn et al. report that, following palliative PEx, patients experienced a sustained decline in QoL after surgery until death [20]. Therefore, all efforts should be made in the preoperative period to select those patients who are likely to have a true survival benefit following this marathon surgery [21].
The objective of our study was to identify factors influencing R0 resection in an irradiated field, including patient and tumour characteristics or surgical aspects, in order to facilitate optimal patient selection and define a surgical roadmap for performing exenterative surgery.
2. Materials and Methods
Our retrospective observational cohort included consecutive patients who underwent pelvic exenteration for gynaecological malignancies at Oxford University Hospitals between 1 January 2011 and 31 December 2024. Oxford is the tertiary referral centre for the Thames Valley Cancer Alliance Network, which includes five recruiting sites and serves a catchment area of 2.3 million.
The primary outcome was margin status. Secondary outcomes were intraoperative and postoperative complications.
Data was collected from paper and electronic patient records. This service evaluation protocol was registered in accordance with the Oxford University Hospitals Trust requirements (registration number 8912). The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The data collected were anonymised. Informed consent was obtained from all patients as part of standard clinical practice to allow for data collection and analysis for research purposes. No remuneration was offered to the patients enrolled in this study.
Definitions
We have defined PEx as follows:
An anterior exenteration involved en-block excision of the gynaecological organs and the urinary bladder. A posterior exenteration included the en-block excision of the gynaecological organs and the rectosigmoid with or without the anus and anal sphincters. A total exenteration comprised of the en-block excision of the urinary bladder, gynaecological organs, and recto-sigmoid ± anus.
We have used the cranio-caudal subclassification of PEx proposed by Magrina et al. (1990) [22] to facilitate a clear understanding of the extent of resection and anatomical changes associated with each type of surgery. A type I PEx is supralevator. A type II PEx is infralevator, with the dissection extending inferiorly to include the levator ani muscles and urogenital diaphragm. A type III PEx includes vulvectomy ± excision of perineal tissues [22].
With regards to margin status, we have defined R0 resection as clear histopathological margins, with tumour > 1 mm from margin, while R1 resection entailed the presence of microscopic residual disease < 1 mm from margin. R2 resection was defined as the presence of macroscopic residual disease at the time of surgery.
A number of patient characteristics were collected from patient notes. Demographic data included age and body mass index (BMI). Medical comorbidities were assessed using the Karnofski Performance Status (PS), the American Society of Anaesthesiologists (ASA) Physical Status classification system, and the Charlson Comorbidity Index (CCI).
All patients followed the Oxford pathway for pelvic exenterations/laterally extended endopelvic resections (LEER) (Figure 1).
Prior to surgery, the Oxford checklist was completed to ensure all relevant preoperative steps have been undertaken (Table 1).
The following surgical details were collected from the operation notes: type of exenteration (anterior/posterior/total and type I/II/III), estimated blood loss (ELB), whether laterally extended endopelvic resection (LEER) was performed, type of urinary diversion, bowel surgery and plastic surgery reconstruction, and intraoperative complications.
From the histopathology reports, we collected the histology diagnosis (squamous cell carcinoma, adenocarcinoma, other), the tumour size, and the margin status (R0/R1/R2).
Postoperative complications within 30 days from the date of surgery were defined using the Clavien–Dindo classification. Data regarding postoperative complications and length of stay (LOS) was collected from patient records.
Statistical analysis was performed using SPSS v. 30.0. Baseline demographic and clinical characteristics were summarised by continuous and categorical variables. Categorical variables were compared with the Chi-square test. When the assumptions required for Chi-square test were not met, Fisher’s exact test was employed. Differences between continuous variables were analysed with the Independent Student’s t-test. Ordinal variables were analysed using the Kruskall–Wallis non-parametric test. A value of p < 0.05 was considered statistically significant. Univariable and multivariable logistic regression was performed using margin status as the dependent variable.
3. Results
We have identified a total of 267 cases. We have excluded 24 patients who either had incomplete records or were not found to have had true exenterations after review of the notes. Out of the remaining 243 cases, we excluded 206 patients for which en-block resection performed during ovarian cytoreductive surgery was coded as “posterior exenteration”—this coding captured only a portion of the cytoreductive surgeries for advanced ovarian cancer performed in our centre. Thirty-seven patients underwent pelvic exenteration for vulval, vaginal, cervical, or uterine malignancies. From these 37 patients, we have excluded 10 cases who did not receive radiotherapy (RT) prior to the pelvic exenteration (Figure 2).
We identified 27 patients with previous radiotherapy treatment, who had a pelvic exenteration for non-ovarian gynaecological malignancies. We only included patients who underwent PEx after RT, as performing major surgery in a previously irradiated field presents additional critical surgical challenges.
3.1. Patient and Tumour Characteristics
The median age was 63 years (range, 41–81) and median body mass index (BMI) was 27 (range, 17–45). Most patients had a performance status (PS) of 0 or 1, as follows: 18 (66.7%) had a PS of 0, 8 (29.6%) had a PS of 1, and 2 (3.7%) had a PS of 2. The American Society of Anaesthesiologists (ASA) score was 1 for 18 patients (66.7%), 2 for 7 patients (27.9%), and 3 for 2 patients (7.4%). The median Charlson Comorbidity Index was 2 (range 0–5) (Table 2).
With regards to the primary tumour site, 3 (11.1%) patients had vulvar cancer, 4 (14.8%) had vaginal cancer, 11 (40.7%) had cervical cancer, and 9 (33.3%) patients had uterine cancer.
The histological diagnosis was squamous cell carcinoma (SCC) for 15 (55.5%) patients, adenocarcinoma (ADK) for 9 (33.3%) patients, carcinosarcoma for 2 (7.4%) patients, and serous carcinoma for one (3.7%) patient.
The majority of our patients (14, 51.9%) had International Federation of Gynaecology and Obstetrics (FIGO) stage 1 disease at diagnosis, 6 (22.2%) had stage 2 disease, 4 (14.8%) had stage 3, and 3 (11.1%) had stage 4 disease.
The primary treatment type was chemoradiotherapy only for 12 (44.4%) patients, surgery and radiotherapy for 8 (29.6%) patients, and all three treatment types (chemotherapy, radiotherapy, and surgery) for 7 (25.9%) patients.
At the time of exenteration, 18 (66.7%) patients had recurrent disease, 6 (22.2%) patients had persistent disease, and 3 (11.1%) patients had a new type of malignancy.
The median time to recurrence was 33 months (range, 8–348). The median pre-operative tumour size was 4.1 cm (range, 0.9–6.7 cm) (Table 2).
3.2. Surgical Technique and Morbidity
The median estimated blood loss (EBL) for our patients was 800 mL (range, 150–2500), and the median LOS was 23 days (range, 5–116).
Seventeen (63%) patients had a total exenteration, eight (29.6%) patients had a posterior exenteration, and two (7.4%) patients had an anterior exenteration. Using the classification proposed by Magrina et al. (1990) [22], 11 (40.7%) patients had a type III, 1 (3.7%) patient had a type II, and 15 (55.6%) had a type I exenteration. Four (14.8%) patients had LEER.
A urinary diversion was required in 19 (70.4%) patients, following cystectomy. All urinary diversions were incontinent conduits. Ten (37%) patients had an ileal conduit, seven (25.9%) of which had a Wallace ileal conduit and three (11.1%) had a Bricker ileal conduit. Nine (33.3%) patients had a colonic conduit; two (7.4%) had a Wallace colonic conduit, and (25.9%) had a Bricker colonic conduit.
Twenty-five (92.6%) of patients underwent colorectal surgery. The most common colorectal procedure performed was Hartmann’s procedure with end colostomy 16 (59.3%). Three patients (11.1%) required abdomino-perineal resection (APR) and end colostomy. Six (22.2%) patients underwent other colorectal procedures.
Nine (33.3%) patients required plastic surgery, and the most common procedure was a vertical rectus abdominis myocutaneous (VRAM) flap, performed for 6 (22.2%) patients. Two (7.4%) patients had and antero-lateral thigh (ALT) flap. One (3.7%) patient had bilateral gracilis flaps, following intraoperative VRAM flap failure due to compromised blood supply. (Table 3)
Eight patients (29.6%) experienced intraoperative complications. Three of them sustained an iliac vein injury, with documented EBLs of 1.5 L, 2 L, and 2.5 L, respectively. Two patients had cystotomies, which were identified and repaired intraoperatively with no postoperative issues. Two patients had enterotomies, one of them requiring small bowel resection and primary anastomosis. One patient had an ischaemic VRAM flap, due to ligation of the inferior epigastric artery during the surgical excision. Perineal reconstruction was performed using bilateral gracilis flaps instead. Finally, one patient had an ischaemic Wallace ileal conduit, which was removed and replaced with a Wallace sigmoid conduit.
Six (22.2%) of our patients had significant postoperative complications (Clavien–Dindo grade III or IV), in the first 30 days post-surgery. Two patients had Clavien–Dindo grade IIIA complications: one developed a para-colic collection, which was drained under ultrasound-guidance, and the second one required a nephrostomy on a single kidney.
Four (14.8%) patients had Clavien–Dindo grade IIIB complications. One of them was found to have a congested VRAM flap on day 2 post surgery. She was taken back to theatre and 50% of the flap was thought to be compromised. The compromised tissue was debrided, and the perineum was reconstructed using a left gracilis flap and a right superior gluteal artery perforator (SGAP) rotational flap and Z-plasty. She later developed a perineal wound dehiscence, which was managed conservatively with a Vacuum-Assisted Closure (VAC) dressing and antibiotics. She also received treatment for urosepsis during admission.
A second patient developed sepsis and a deterioration in kidney function on day 9 post surgery. Computerised tomography (CT) was performed, which identified an entero-vaginal fistula and a fistula between the ileal conduit and the small bowel. She was taken to theatre on day 12 post surgery, with the intention to repair the fistulae. On entry to the abdomen, the small bowel entered a pelvic inflammatory phlegmon which was not thought safe to remove due to risk of multiple enterotomies. A defunctioning proximal loop ileostomy was created. The urine was diverted using bilateral nephrostomies. She was discharged home on day 20.
Another patient developed an ischaemic right leg on day 1 post surgery, and she returned to theatre for embolectomy of an external iliac artery and superficial femoral artery thrombus. The embolectomy unfortunately failed and the patient experienced recurrent ischaemia secondary to compartment syndrome. She was transferred to theatre a second time for a femoral–femoral cross-over graft and right lower leg fasciotomy. She also experienced a pelvic collection, which was managed conservatively.
Finally, a fourth patient developed dehiscence of the vaginal and anal stumps and a recto-vaginal fistula, which was managed conservatively using endo-sponge therapy (Table 4).
3.3. Margin Status
Twenty-one (77.8%) of our patients had resection of all microscopic and macroscopic disease (R0 was achieved); four (14.8%) had no residual tumour, while seventeen (63%) had residual carcinoma in the specimen, with microscopically-clear margins.
Of the six (22.2%) patients with microscopically-involved margins, four (14.8%) had one margin involved, one (3.7%) had two margins involved, and one (3.7%) had three margins involved. None of the patients had macroscopic residual disease (R2) (Table 5).
3.4. Lymph Node Status
With regards to lymph node status, none of our patients had macroscopically-involved lymph nodes. Microscopic lymph node involvement was identified in two cases. The first case, a 74-year-old patient undergoing pelvic exenteration for uterine carcino-sarcoma, with a history of anal squamous cell carcinoma treated with chemoradiotherapy, was found to have microscopic involvement of para-aortic lymph nodes by metastatic anal squamous cell carcinoma. This patient had clear margins (R0). The second patient, a 63-year-old undergoing posterior exenteration for recurrent vulval squamous cell carcinoma, was found to have a microscopically involved left femoral lymph node. This patient had a tumour measuring 8.9 cm on histology, and the margins were microscopically involved (R1). We did not include the lymph node status in our statistical analysis as we only had two cases with lymph node involvement, one by a different tumour.
3.5. Statistical Analysis
Univariable analysis was performed to identify associations between a number of variables and R0 status (Table 6).
Our paper found a statistically significant association between the patient’s age and R0 status (p value 0.035, Independent t-test), with a median age of 61 in the R0 group versus 70 in the R1 group.
There was a significant association between tumour size and R0 status. This applied to both estimated pre-operative tumour size based on imaging (p value 0.014 Independent t-test) and actual tumour size on the histopathology specimen (p value 0.006 Independent t-test). The mean tumour size was 3.4 cm in the R0 group, both on pre-operative and on histopathological assessment. In the R1 group, the mean tumour size was 5 cm on imaging and 6 cm on histopathological examination.
The mean estimated blood loss was 653 mL in the R0 group, versus 1267 mL in the R1 group, with a p value of 0.06, just above significance level (Independent t-test).
Univariable logistic regression was performed to assess the effect of multiple factors on the likelihood of achieving R0, and the results are presented in Table 7.
Tumour size on imaging, tumour size on histology, and EBL were found to be statistically significant in predicting the likelihood of achieving R0.
Multivariable logistic regression was performed, using margins status as dependent variable and age, EBL and tumour size on histology as independent variables (Table 8). None of these three variables remained significant, likely due to limited number of events (6 patients with R1) and a small sample size with only 27 patients.
4. Discussion
Multiple studies have demonstrated a negative association between larger tumour size on preoperative assessment and both progression-free and overall survival following exenterative surgery [2,18,23,24], and various tumour size thresholds have been suggested as criteria for offering PEx: 3 cm [4,25,26], 4 cm [16,17], and 5 cm [27].
This association is likely a result of lower R0 resection rates in patients with larger tumours.
Our study identified a significant association between tumour size and R0 resection, both on univariable analysis (Independent t-test) and on univariable logistic regression. The mean tumour size on histopathological examination was 3.4 cm in the R0 group vs. 6 cm in the R1 group.
These results are in keeping with existing literature. In a retrospective study including 151 patients with gynaecological, colorectal, and urological malignancies undergoing pelvic exenteration, Smith et al. (2017) [28] found that there was an 11% increase in the risk of positive margins for every 1 cm increase in size of tumour (OR 1.11; 95%CI 1.02–1.22). They also found that tumours > 4 cm in size were more likely to recur (65%) compared to tumours ≤ 4 cm (42%) and cases with no residual tumour on final pathology (20%), p = 0.016 [28].
One of the most daunting tasks for the multidisciplinary team pre- and intraoperatively is to distinguish between the tumour tissue and radiation-induced fibrosis or local inflammation [29]. Pre-operatively, an MRI of the pelvis can assess the relationship between the tumour and various adjacent anatomical structures such as ureters, nerves, and iliac vessels [30], while Diffusion Weighted Imaging sequences add functional information and can help distinguish fibrosis from tumour [31]. PET CTs, generally used for detecting lymph node metastases and extra-pelvic disease [31], also aid in defining tumour extent and differentiating fibrosis from metabolically active malignant tissue [32]. However, preoperative tumour size assessment remains a challenge in the post-radiotherapy field. We found a mean difference of 1.4 cm (range 0–4.9 cm) between tumour size on imaging and tumour size on histology. For this reason, while there is no general consensus globally, we recommend obtaining a generous margin of 2–3 cm of healthy tissue at the time of exenteration, when anatomically possible, keeping in mind that, following paraffin fixation, there is linear tissue shrinking by approx. 15% and a 30–40% loss in tissue volume.
Our paper found a statistically significant association between the patient’s age and R0 status (p value 0.035, Independent t-test), with a median age of 61 in the R0 group versus 70 in the R1 group. We believe this association may be justified by the presence of more advanced fibrosis in older patients, making intraoperative assessment of margins problematic. While advancements in technology have enabled clinical oncologists to target tissue with higher precision, collateral damage to normal tissue remains an unavoidable consequence of radiotherapy. Chronic inflammatory and fibrotic changes typically occur up to one year after completing treatment and worsen over time. Changes include progressive tissue induration, rigid stromal encasement of capillaries and sinusoids that become distorted and dilated, entrapment of neurological structures, dryness, and atrophy [33]. Trauma or infection may lead to further vascular compromise and result in ulceration or necrosis [33]. Furthermore, older age at time of radiotherapy has been identified as a strong independent risk factor for developing radiation-induced toxicity [34], likely due to a reduced ability to repair damaged tissues at a more advanced age. Comorbidities affecting the microcirculation such as diabetes, cardiovascular disease, and immobility may further accelerate fibrotic progression. We found that intraoperative EBL was statistically significant in predicting the likelihood of achieving R0, with a mean EBL of 653 mL in the R0 group, versus 1267 mL in the R1 group. This is not surprising, given the deleterious effect of bleeding on the surgical field, reducing visibility and making tissue planes demarcation more challenging. Bleeding also increases the pace of surgery and heightens the stress levels of the surgical team, therefore making surgical errors more likely. It is our routine practice to start any PEx procedure by opening the pelvic sidewalls, exposing the pararectal, para-vesical and Latzko spaces and achieving devascularisation of the pelvis by ligating the anterior branch of the internal iliac artery 3 cm distal to the common iliac artery bifurcation. Higher blood loss could also represent a surrogate marker for more advanced disease increasing the difficulty of surgery.
We identified a statistically significant association between primary tumour site and R0 resection (p = 0.036). While all cervical cases achieved negative margins, only 50% of non-cervical tumour types did.
The observed differences likely reflect the distinct biological behaviours and treatment sensitivities among gynaecological malignancies. Cervical cancer is generally both radio- and chemosensitive, particularly in squamous histology, and tends to recur centrally, making it more amenable to complete surgical clearance. In contrast, endometrial cancers are often less radiosensitive and more prone to distant dissemination, reducing the likelihood of durable local control. Vulval cancers, while predominantly squamous, comprise two biologically distinct subtypes: HPV-associated (p16-positive) tumours, which are typically more radiosensitive and occur in younger patients, and p53-mutated (HPV-independent) tumours, which are more common in older women, often arise in the setting of chronic dermatoses, and are less responsive to radiotherapy. Vaginal cancers, though rare and often managed similarly to cervical cancer, may exhibit variable responses to radiation due to anatomical proximity to radiosensitive organs and reduced vascular perfusion in some segments of the vaginal wall, both of which limit the radiation dose that can be safely delivered and affect tissue tolerance. These differences underscore the importance of tailoring exenterative surgery to tumour biology, histological subtype, and recurrence pattern when selecting candidates for this complex and highly morbid procedure and support pelvic exenteration as being most effective in the management of centrally recurrent cervical cancer.
Our study is the first specifically looking at R0 and complication rates in previously irradiated patients undergoing a pelvic exenteration for a non-ovarian gynaecological malignancy. In Table 9, we have summarised the findings of 14 retrospective studies on pelvic exenteration published in the last 10 years (2015–2025), demonstrating data gaps, particularly in relation to reporting R0 rates—the main factor associated with survival—and post-radiotherapy status. Our study compares favourably with existing literature in terms of an R0 resection rate of 77.8% (54.2–81.6%) and a 30-days severe complications rate (Clavien–Dindo grade 3 and 4) of 23.2% (21.2–74%).
This study has several limitations that should be acknowledged. Firstly, its retrospective observational design is inherently subject to selection and information bias, as data were collected from existing medical records with variable completeness and accuracy. The small sample size (n = 27) limited the statistical power of the analyses and likely contributed to the fact that, although multivariable analysis was performed, none of the variables retained statistical significance. This limits the ability to draw firm conclusions regarding independent predictors of R0 resection. Pelvic exenteration is a rare procedure, reserved for a very limited number of patients, which inevitably results in a paucity of data. We believe it was important to restrict inclusion criteria to post-radiotherapy cases only, as achieving R0 resection in a previously irradiated field poses specific challenges. In gynaecological malignancies, radiotherapy typically delivers higher biologically effective doses, often exceeding 80 Gy EQD2 when combining external beam and brachytherapy to central pelvic tissues, resulting in extensive fibrosis and obliteration of normal tissue planes. In contrast, colorectal and urological cancers usually receive lower or more conformally delivered doses—approximately 45–50 Gy for rectal cancer and 64–80 Gy for bladder cancer—targeting smaller volumes and sparing much of the surrounding soft tissue. Consequently, surgery after gynaecological radiotherapy is uniquely demanding, with increased risks of vascular and ureteric injury and difficulty distinguishing tumour from post-treatment fibrosis. Furthermore, we excluded ovarian cases, as en-bloc resections performed during ovarian cytoreductive surgery are typically supralevator and undertaken in non-irradiated fields, representing a distinct disease biology, treatment paradigm, and survival outlook. We also excluded pelvic exenterations performed for non-gynaecological malignancies, and patients who underwent LEER only without PEx. Our sample size is comparable to other single-centre publications from major referral centres when accounting for these stricter inclusion criteria (Table 9). We believe that a future prospective, multicentre collaboration would be highly valuable to validate and build upon our findings. Positive pelvic, para-aortic [44], and inguino-femoral [45] nodal involvement is known to be a key predictor of reduced overall survival. Our study only identified one patient with an unexpected microscopic involvement of para-aortic lymph nodes by a different tumour (anal squamous cell carcinoma), and one patient with microscopic involvement of a femoral lymph node; therefore, we were not able to include lymph node status in the statistical analysis. Finally, we do not present long-term oncological data in this study, but we will endeavour to report this once our patient cohort has completed follow-up.
5. Conclusions
From a clinical standpoint, our findings emphasise the importance of meticulous preoperative evaluation, multidisciplinary planning, and judicious patient selection. The patients most likely to benefit from pelvic exenteration in a post-radiotherapy field are younger individuals with smaller, centrally recurrent tumours—particularly of cervical origin—where complete (R0) resection is achievable. Intraoperatively, careful control of blood loss, achieved through early devascularisation of the pelvis, is essential to optimising surgical precision and outcomes.
In summary, preoperative tumour size, primary tumour site, and patient age should be key considerations in selecting suitable candidates for pelvic exenteration following radiotherapy, while minimising intraoperative blood loss remains critical to maximising the likelihood of achieving R0 resection—the single most important determinant of survival in this complex procedure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brunschwig A. Complete excision of pelvic viscera for advanced carcinoma: A one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy Obstet. Gynecol. Surv.1949443043110.1097/00006254-194906000-0006718875031 · doi ↗ · pubmed ↗
- 2Kelly M.E. Ryan E.J. Aalbers A.G.J. Abdul A.N. Abraham-Nordling M. Alberda W. Antoniou A. Austin K.K. Baker R. Bali M. Pelvic Exenteration for Advanced Nonrectal Pelvic Malignancy Pelv Ex Collaborative Ann. Surg.20192708999053163418410.1097/SLA.0000000000003533 · doi ↗ · pubmed ↗
- 3Ubinha A.C.F. Pedrão P.G. Tadini A.C. Schmidt R.L. Santos M.H.D. Andrade C.E.M.D.C. Longatto Filho A. Reis R.D. The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature Cancers 20241681710.3390/cancers 1604081738398208 PMC 10886894 · doi ↗ · pubmed ↗
- 4Maggioni A. Roviglione G. Landoni F. Zanagnolo V. Peiretti M. Colombo N. Bocciolone L. Biffi R. Minig L. Morrow C.P. Pelvic exenteration: Ten-year experience at the European Institute of Oncology in Milan Gynecol. Oncol.2009114646810.1016/j.ygyno.2009.03.02919411097 · doi ↗ · pubmed ↗
- 5Jäger L. Nilsson P.J. Rådestad A.F. Pelvic exenteration for recurrent gynecologic malignancy: A study of 28 consecutive pa–tients at a single institution Int. J. Gynecol. Cancer 20132375576210.1097/IGC.0b 013e 318287 a 87423407096 · doi ↗ · pubmed ↗
- 6Höckel M. Laterally extended endopelvic resection: Surgical treatment of infrailiac pelvic wall recurrences of gynecologic malignancies Am. J. Obstet. Gynecol.199918030631210.1016/S 0002-9378(99)70204-89988791 · doi ↗ · pubmed ↗
- 7Höckel M. Laterally extended endopelvic resection. Novel surgical treatment of locally recurrent cervical carcinoma involving the pelvic side wall Gynecol. Oncol.20039136937710.1016/S 0090-8258(03)00502-X 14599868 · doi ↗ · pubmed ↗
- 8Solomon M.J. Brown K.G.M. Koh C. Lee P. Austin K.K.S. Masya L. Lateral pelvic compartment excision during pelvic exenteration Br. J. Surg.20151021710171710.1002/bjs.991526694992 · doi ↗ · pubmed ↗