When Our “Best” Isn’t Good Enough: Asleep Paralyzed Fiberoptic Intubation After a Failed Awake Fiberoptic at an Outside Hospital
James Chen, Benjamin D Brakke, Timon J Higgins, Bradly J Narr

TL;DR
A 72-year-old woman required a complex intubation after previous attempts failed, leading to successful asleep, paralyzed intubation.
Contribution
Presents a novel approach using asleep, paralyzed intubation after failed awake attempts in a high-risk patient.
Findings
Awake fiberoptic intubation failed multiple times at an outside hospital.
Asleep, paralyzed intubation using a combined video laryngoscope and fiberoptic method was successfully performed.
The case highlights effective risk mitigation and decision-making in difficult airway management.
Abstract
A 72-year-old, 127-cm, 53-kg female presented to our hospital after her surgery was canceled at an outside hospital due to multiple failed awake fiberoptic intubation attempts. She required a total abdominal hysterectomy, bilateral salpingectomy, and pelvic lymph node dissection for endometrial cancer. Given the prior failed awake attempts, we performed an asleep, paralyzed, combined video laryngoscope and fiberoptic oral intubation. The decision-making, actions, and risk mitigation provide an interesting case for discussion.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
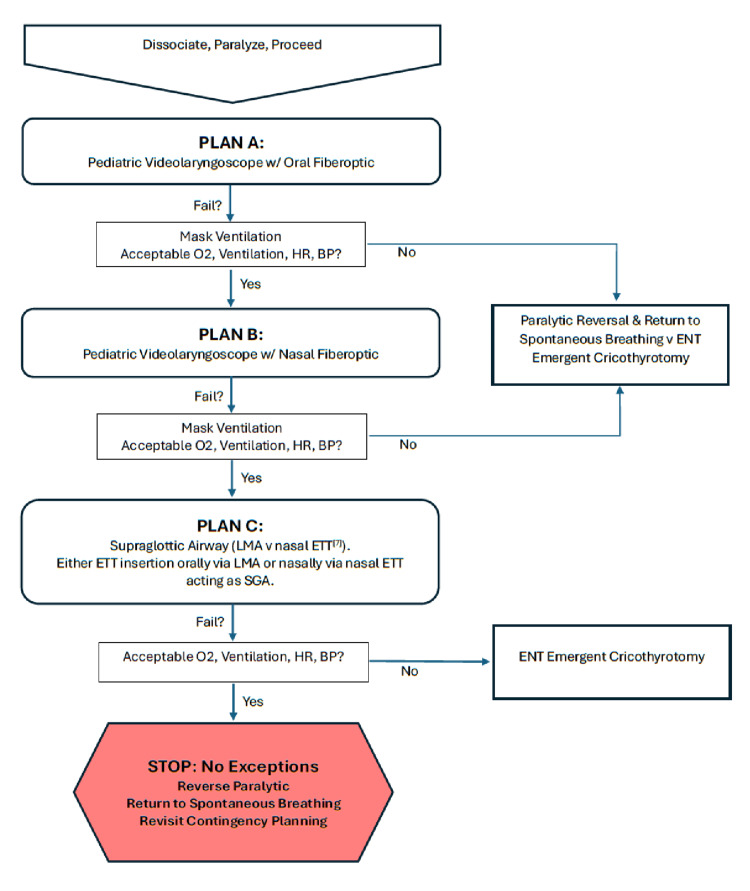 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Cardiac Arrest and Resuscitation · Restraint-Related Deaths