Pericardial Effusion as an Early Manifestation of Myeloperoxidase (MPO)-Positive Antineutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis With Eosinophilia
Amol Karkhanis, Moemen Hasaballah, Mohamed Elsayed, Hassan Rizwan, Anees S Butt, Mohamed Abdulmajeed

TL;DR
A rare autoimmune disease presented with heart fluid and kidney issues, and was successfully treated with steroids and rituximab.
Contribution
This case highlights pericardial effusion as an early sign of MPO-positive AAV with eosinophilia.
Findings
Pericardial effusion was an early manifestation of MPO-positive AAV with eosinophilia.
Treatment with corticosteroids and rituximab resolved the effusion and improved kidney function.
Early recognition of cardiac symptoms can lead to timely treatment of systemic vasculitis.
Abstract
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a rare but life-threatening autoimmune disease that primarily targets the kidneys and lungs. Cardiac involvement is far less common, and when it does occur, it is often overlooked until late in the disease course. We describe an elderly man who presented with acute breathlessness, pericardial effusion, eosinophilia, and worsening renal function. Initial management of pneumonia proved ineffective, and further investigation revealed strongly positive myeloperoxidase (MPO)-ANCA antibodies. The diagnosis of MPO-positive AAV with eosinophilia was established. Following treatment with corticosteroids and rituximab, the patient showed complete resolution of the effusion and significant recovery of renal function. This case highlights the diagnostic challenge of pericardial effusion as an early clue to systemic vasculitis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
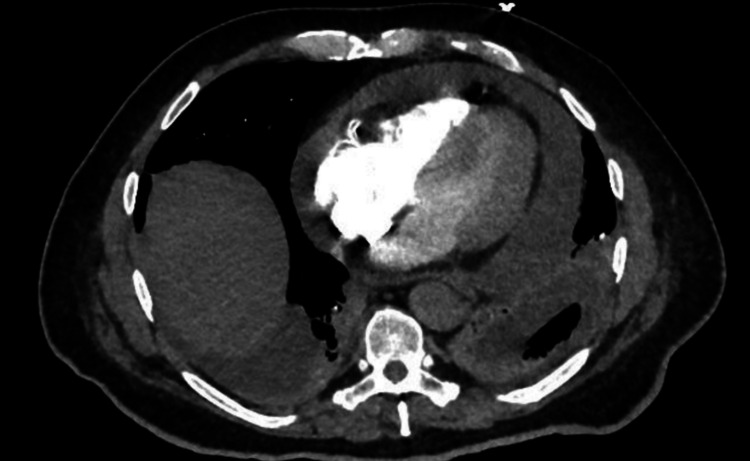 Figure 1
Figure 1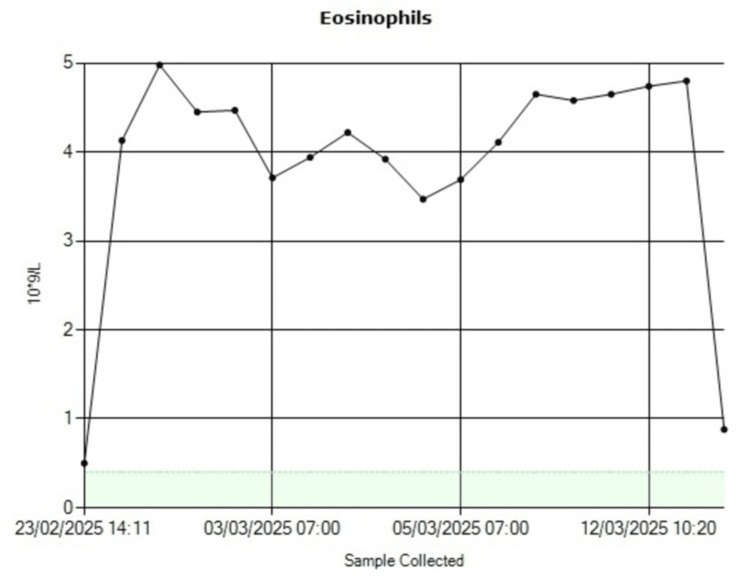 Figure 2
Figure 2| Parameter | Result | Reference range |
| Hemoglobin | 131 g/L | 130-170 g/L |
| WBC count | 15.2 ×10⁹/L | 4-11 ×10⁹/L |
| Neutrophils | 12.5 ×10⁹/L | 2-7.5 ×10⁹/L |
| Eosinophils | 0.5 ×10⁹/L | 0.0-0.4 ×10⁹/L |
| CRP | 81 mg/L | <5 mg/L |
| Creatinine | 140 µmol/L (baseline ~95) | 60-110 µmol/L |
| Urea | 7.7 mmol/L | 2.5-7.8 mmol/L |
| Parameter | Result | Reference range |
| Hemoglobin | 133 g/L | 130-170 g/L |
| WBC count | 15.0 ×10⁹/L | 4-11 ×10⁹/L |
| Neutrophils | 8.6 ×10⁹/L | 2-7.5 ×10⁹/L |
| Eosinophils | 5.0 ×10⁹/L | 0.0-0.4 ×10⁹/L |
| CRP | 99 mg/L | <5 mg/L |
| Creatinine | 383 µmol/L | 60-110 µmol/L |
| Urea | 18.6 mmol/L | 2.5-7.8 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Eosinophilic Disorders and Syndromes · Sarcoidosis and Beryllium Toxicity Research
Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) represents a group of uncommon but severe systemic vasculitides, characterized by inflammation and necrosis of small- to medium-sized blood vessels [1]. The disease spectrum encompasses microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA), and eosinophilic GPA (EGPA), each with distinct but sometimes overlapping clinical features [2].
For orientation, GPA is typically characterized by necrotizing granulomatous inflammation affecting the upper and lower respiratory tracts; MPA often presents with rapidly progressive glomerulonephritis and pulmonary capillaritis without granulomatous inflammation; and EGPA classically features asthma, eosinophilia, and systemic vasculitis.
While kidneys and lungs are the principal organs involved in AAV, the heart can also be affected, though this is less frequently reported [3]. Cardiac involvement has been reported in approximately 6-20% of patients with AAV, most commonly manifesting as myocarditis, pericarditis, or conduction abnormalities [4]. Cardiac manifestations range from conduction disturbances and myocarditis to pericarditis and pericardial effusion [4]. Such presentations are clinically important because they carry significant prognostic implications and can complicate an already challenging diagnostic landscape [5]. The presence of eosinophilia, as in our case, adds another layer of complexity. Eosinophilia may point toward EGPA but can also occur in myeloperoxidase (MPO)-positive vasculitis without classical features of EGPA [6]. This overlap can create diagnostic ambiguity, particularly when patients lack hallmark respiratory features such as asthma or chronic rhinosinusitis. Here, we present a case in which a pericardial effusion was the earliest clue to an underlying systemic vasculitis. The narrative illustrates how diagnostic reasoning evolved and how timely immunosuppressive therapy averted irreversible organ damage.
Case presentation
A 73-year-old man presented with one week of worsening shortness of breath and a productive cough. His medical history was notable for type 2 diabetes mellitus, atrial fibrillation, bronchiectasis, obstructive sleep apnea, prior myopericarditis, and left nephrectomy. The prior episode of myopericarditis occurred three years earlier and was treated conservatively with complete clinical and echocardiographic resolution. There was no evidence of residual pericardial effusion on follow-up imaging, making a chronic effusion unlikely in the current presentation. On admission, he was tachypneic and required 8 L/min of oxygen to maintain oxygen saturation at 93%. His blood pressure was 106/68 mmHg, heart rate 86 bpm, respiratory rate 24/min, and temperature 37.1°C. Physical examination revealed coarse crackles over both lung bases and mild pedal edema, but no jugular venous distension.
Initial laboratory investigations showed raised inflammatory markers, neutrophilia, mild eosinophilia, and acute kidney injury (creatinine 140 µmol/L with a baseline around 95 µmol/L) (Table 1). CT pulmonary angiography excluded pulmonary embolism but demonstrated bilateral consolidation and a large pericardial effusion (Figure 1). Transthoracic echocardiography confirmed a moderate-to-large effusion without signs of tamponade. Cardiac biomarkers, including troponin T (14 ng/L; reference <15 ng/L) and CK-MB (16 U/L; reference <25 U/L), were within normal limits, and there was no serial rise. ECG demonstrated nonspecific T-wave flattening without classical pericarditic ST-segment elevation or PR depression. A chest X-ray showed an enlarged cardiac silhouette consistent with a large pericardial effusion but no pulmonary congestion. These findings supported isolated pericardial involvement rather than myocarditis.
CT chest demonstrating large pericardial effusionCT: computed tomography
The patient was initially managed with broad-spectrum antibiotics for presumed pneumonia, but his clinical and biochemical parameters failed to improve. Blood, urine, and sputum cultures remained sterile, and viral panels were negative. Given the ongoing fever, rising creatinine, and progressive eosinophilia (Table 2), an autoimmune cause was suspected.
Serology revealed strongly positive MPO-ANCA (>130 U/mL) with negative PR3-ANCA. Bronchoscopy with mucosal biopsy showed inflammatory changes with tissue eosinophilia but no evidence of malignancy. Collectively, these findings established a diagnosis of MPO-positive AAV with eosinophilia.
He was treated with high-dose intravenous methylprednisolone (500 mg daily for three days) followed by an oral prednisolone taper over 12 weeks, in addition to rituximab administered as two 1 g infusions given two weeks apart, following the RAVE protocol.
Following the induction phase, the patient was transitioned to oral prednisolone, which was gradually tapered from 60 mg daily to 5 mg daily over 12 weeks. Rituximab was administered as two 1 g infusions given two weeks apart, with good tolerance and no infusion reactions. He also received adjunctive Pneumocystis jirovecii prophylaxis with co-trimoxazole (480 mg once daily) and gastric protection with a proton pump inhibitor. Blood pressure and glucose were closely monitored throughout steroid therapy. Renal function improved progressively (creatinine decreased from 383 µmol/L to 128 µmol/L), and inflammatory markers normalized by the sixth week. The patient remained stable during follow-up, with no recurrence of effusion on repeat echocardiography at three months.
The patient’s renal function improved, and inflammatory markers normalized, with eosinophil levels declining progressively to normal values (Figure 2). Echocardiography demonstrated complete resolution of the pericardial effusion. He was discharged home in good condition with outpatient follow-up.
Eosinophils level down trend
Discussion
This case highlights the diagnostic challenge posed by atypical presentations of AAV. While renal and pulmonary features dominate most case series [2], cardiac manifestations, particularly pericardial effusion, are rare but important [3,7]. The prevalence of cardiac involvement in AAV ranges from 6% to 20%, with myocarditis and pericarditis being the most common manifestations [3,7]. Pericardial effusion is less common and, when it occurs, is often mistaken for infection, malignancy, or heart failure [4]. Previous reports have documented cases progressing to tamponade, underscoring the seriousness of this complication [5]. In our patient, the effusion was large but hemodynamically stable, providing a vital clue before catastrophic deterioration occurred. The marked eosinophilia initially led the differential toward a diagnosis of EGPA. However, EGPA is typically characterized by asthma, sinus disease, and pulmonary infiltrates [6]. The absence of these features, coupled with high MPO-ANCA titers, favored MPO-positive AAV with eosinophilia rather than classical EGPA [8]. This overlap demonstrates the limitations of rigid disease classification and reminds clinicians to interpret laboratory findings within the broader clinical context. This case illustrates how physicians must balance probabilities. The patient’s presentation with fever, consolidation, and effusion strongly suggested infection, and empiric antibiotics were appropriate. Yet persistence of inflammation, renal dysfunction, and rising eosinophils warranted reconsideration. The eventual pivot to autoimmune testing demonstrates the iterative nature of diagnostic reasoning in real-world practice.
Standard induction therapy for AAV involves corticosteroids combined with either cyclophosphamide or rituximab [8]. The pivotal RAVE trial demonstrated that rituximab is non-inferior to cyclophosphamide and may be more effective in relapsing disease [9]. Our patient’s favorable response to steroids followed by rituximab aligns with this evidence. Beyond acute management, relapse prevention remains a significant challenge, with long-term maintenance using rituximab or azathioprine shown to reduce recurrence [10,11]. Long-term survival in AAV has improved substantially with modern immunosuppression, but mortality remains higher than in the general population [10]. Renal involvement is the strongest predictor of poor outcome, while cardiac manifestations add further risk [12]. Early recognition, therefore, is crucial, not only to reverse acute pathology but also to alter long-term prognosis.
This case reinforces the importance of maintaining diagnostic flexibility. When faced with a patient whose course does not follow the expected trajectory, clinicians must be prepared to step back, reconsider, and broaden their differential diagnosis. In retrospect, the pericardial effusion represented the earliest manifestation of the underlying vasculitic process, preceding the development of overt renal and hematologic features. Recognizing that eosinophilia was not solely attributable to infection but could also signal vasculitis was pivotal.
Conclusions
Pericardial effusion can rarely represent the initial presentation of MPO-positive AAV with eosinophilia. Its occurrence in the context of systemic inflammation, eosinophilia, and acute kidney injury should prompt consideration of vasculitis, particularly when infection is excluded. Timely initiation of immunosuppressive therapy is essential to prevent irreversible organ damage. This case illustrates how careful observation, diagnostic adaptability, and early multidisciplinary intervention can dramatically alter the patient’s outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Small-vessel vasculitis N Engl J Med Jennette JC Falk RJ 151215233371997936658410.1056/NEJM 199711203372106 · doi ↗ · pubmed ↗
- 2Classification, epidemiology and clinical subgrouping of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis Nephrol Dial Transplant Watts RA Mahr A Mohammad AJ Gatenby P Basu N Flores-Suárez LF 142230201510.1093/ndt/gfv 02225805746 · doi ↗ · pubmed ↗
- 3Standard and feature tracking magnetic resonance evidence of myocardial involvement in Churg-Strauss syndrome and granulomatosis with polyangiitis (Wegener's) in patients with normal electrocardiograms and transthoracic echocardiography Int J Cardiovasc Imaging Miszalski-Jamka T Szczeklik W Sokołowska B 8438532920132321227410.1007/s 10554-012-0158-6PMC 3644401 · doi ↗ · pubmed ↗
- 4Pleuritis and pericarditis in antineutrophil cytoplasmic autoantibody-associated vasculitis Chest Thompson GE Bourne MH Jr Casal Moura M 57258116020213366749210.1016/j.chest.2021.02.049 · doi ↗ · pubmed ↗
- 5Risk of cardiovascular disease and venous thromboembolism among patients with incident ANCA-associated vasculitis: a 20-year population-based cohort study Mayo Clin Proc Berti A Matteson EL Crowson CS Specks U Cornec D 5976069320182958807910.1016/j.mayocp.2018.02.010PMC 6057792 · doi ↗ · pubmed ↗
- 6Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort Arthritis Rheum Comarmond C Pagnoux C Khellaf M 2702816520132304470810.1002/art.37721 · doi ↗ · pubmed ↗
- 7The epidemiology of antineutrophil cytoplasmic autoantibody-associated vasculitis in Olmsted County, Minnesota: a twenty-year US population-based study Arthritis Rheumatol Berti A Cornec D Crowson CS Specks U Matteson EL 233823506920172888144610.1002/art.40313 PMC 5711593 · doi ↗ · pubmed ↗
- 8EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis Ann Rheum Dis Yates M Watts RA Bajema IM 158315947520162733877610.1136/annrheumdis-2016-209133 · doi ↗ · pubmed ↗