Measuring the disinfection efficacy of the Tru-D iQ and Tru-D Legacy systems in acute patient care hospital rooms: a randomized experimental study
Bobby G. Warren, Guerbine Fils-Aime, Amanda M. Graves, Aaron Barrett, Nicholas A. Turner, Deverick J. Anderson

TL;DR
This study compares two UV-C systems for disinfecting hospital rooms and finds both effective, with one being faster.
Contribution
The study provides empirical evidence on the efficacy and efficiency of two UV-C disinfection systems in real hospital settings.
Findings
Both Tru-D iQ and Legacy systems significantly reduced environmental contamination in hospital rooms.
Tru-D iQ achieved comparable disinfection efficacy with significantly shorter cycle times than the Legacy system.
Abstract
In this randomized experimental study, Tru-D iQ and Legacy UV-C systems both reduced environmental contamination in hospital rooms. Both systems significantly reduced contamination, with the Tru-D iQ achieving comparable efficacy overall and significantly shorter cycle times.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
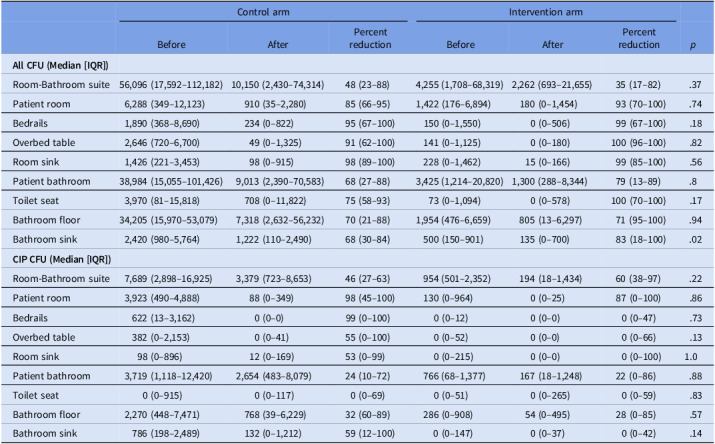 Figure 1
Figure 1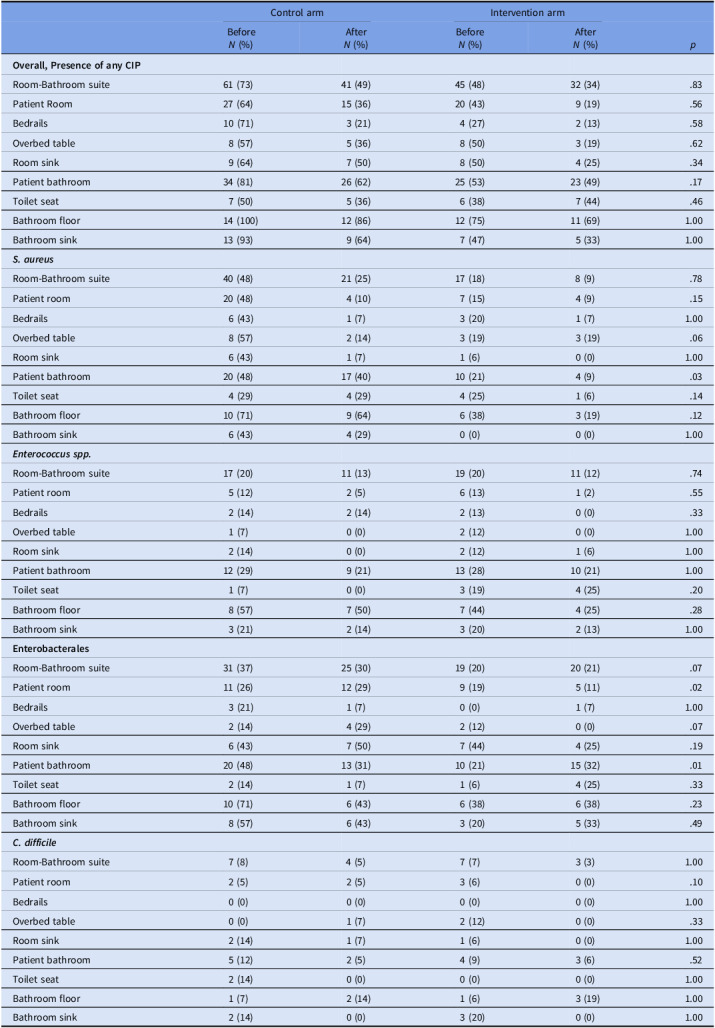 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control in Healthcare · Medical Device Sterilization and Disinfection · Infection Control and Ventilation
Introduction
Over 700,000 healthcare-associated infections (HAIs) and 99,000 related deaths occur annually in the United States.^ 1,2 ^ The healthcare environment is a key contributor to HAI transmission.^ 3–5 ^ Therefore, effective environmental disinfection is critical, yet standard chemical disinfection is limited by compliance and contact time; thus, enhanced disinfection strategies are needed.^ 6–8 ^
Previously, the Tru-D UV-C system (PDI Healthcare) demonstrated effectiveness in decreasing the incidence of MRSA and VRE in high-risk hospital rooms and hospitalwide incidence of Clostridioides difficile and VRE when used for terminal disinfection without concurrent chlorine-based disinfectants.^ 9,10 ^ Bathrooms received only indirect UV-C, and run times often exceeded 45 minutes, limiting feasibility.
An improved UV-C delivery system (Tru-D iQ) was developed to improve direct UV-C coverage and reduced disinfection run times. We completed a randomized experimental study to assess whether the Tru-D iQ demonstrated superior disinfection efficacy and operational performance compared with the Tru-D Legacy system after patient discharge.
Methods
Study setting and design
We performed this study in inpatient rooms at Duke University Hospital, a 1 048-bed tertiary care hospital in Durham, North Carolina.
Rooms were randomized 1:1 to intervention (Tru-D iQ) or control (Tru-D Legacy). Randomization was stratified by room size so that once a room of a particular size category was assigned to one device, the next room of that size was assigned to the alternate device to maintain size balance across arms. Both Tru-D iQ and Tru-D Legacy systems use real-time sensors to end cycles once the target fluence is reached, with duration adjusting automatically to room size and reflectivity. Each system employs preset cycles specific to vegetative or spore-forming bacteria. The iQ includes a compact secondary emitter for direct bathroom exposure, while the Legacy uses a single-unit emitter for the main room only. Clinical, laboratory, and statistical staff were blinded to randomization; device operators were not.
Six areas in each study room, three in the main room (bed rails, overbed table, and in-room sink) and three in the patient bathroom (toilet seat, bathroom floor around the base of the toilet, and the bathroom sink) were split in half by left and right sides and randomized to pre and postdisinfection sampling.
Additionally, 10 x 10 cm formica sheets were inoculated with 1 x 10^4^ CFU of USA300 Methicillin-resistant Staphylococcus aureus (vegetative disinfection cycles) or Ribotype 027 C. difficile (spore cycles) and placed in three predetermined locations: medical prep area, computer keyboard, and toilet seat.
Study protocol
Rooms were enrolled immediately following the discharge of a patient on contact precautions and prior to any physical cleaning or chemical disinfection. Each room was randomized to the intervention or control study arm, and sample areas were further randomized by pre and postdisinfection sampling as described above. Any item obstructing sampling, such as linens, were removed. The disinfection cycle was selected according to the pathogen that had required contact precautions for the discharged patient. Inoculated formica sheets were placed at predetermined locations, and the assigned UV-C system was used to disinfect the room. Following disinfection, samples were collected from postdisinfection surfaces and formica sheets.
Microbiological methods
All environmental cultures were obtained using the sponge–stomacher technique as previously described, with homogenates plated onto routine and selective media for clinically important pathogens (CIPs), defined as S. aureus, Enterococcus spp., Enterobacterales, and C. difficile. Species were confirmed via 16S rRNA sequencing.^ 5,8 ^
Outcomes
The primary outcome was the percent reduction in total contamination, measured in colony-forming units (CFUs), from pre to postdisinfection on environmental surfaces. Results from the intervention arm were compared against results from the control arm. Total room CFUs were determined separately for pre and postdisinfection samples by summing the CFUs from all six sampled surfaces on a given side (eg, all right-side surfaces or all left-side surfaces). For analysis, these six sites together were defined as the “room–bathroom suite,“ while the three main room sites (bedrails, overbed table, and room sink) were grouped as “room“ and the three-bathroom sites (toilet seat, bathroom floor, and bathroom sink) were grouped as “bathroom.“ Secondary outcomes were the percent reduction in CFU counts for CIPs, percent reduction in surfaces positive for CIPs, elimination of inoculated pathogens on formica sheets, and device run time.
Statistical analysis
The Wilcoxon signed-rank test was used to compare overall and CIP CFU percent reduction between study arms, device run time, and the Fisher’s exact test was used to compare proportions of sample areas with CIPs and pathogen elimination on formica sheets. P < .05 was considered to be significant. All statistical tests were two-tailed and performed using SAS, version 9.4M7 (SAS Institute Inc). This study was reviewed by the Duke University Health System Institutional Review Board and received an “exempt” status.
Results
Thirty rooms were enrolled: 16 intervention and 14 control. Of those, 18 received the vegetative cycle (10 intervention, 8 control), and 12 received the spore cycle (6 per group). Overall, 396 samples were collected. In general, predisinfection CFU counts were substantial: 23,845 (IQR 1,958–75,360) in suites, with the bathroom (13,407; IQR 1,353–57,538) and bathroom floor (11,701; IQR 1,079–45,225) most contaminated.
Overall, both arms showed bioburden reduction at the suite, room, bathroom, and surface levels (Table 1). Median percent reduction was generally greater in rooms treated with the Tru-D iQ system compared to the Tru-D Legacy system, though most differences were not statistically significant. Notably, bathroom sinks demonstrated a significantly greater reduction with iQ [83% (IQR 18–100)] compared to Legacy [68% (IQR 30–84); P = .02]. For CIPs, both arms showed reductions, with iQ often greater but not significant. Species-level analysis reported as proportion of positive samples demonstrated variable reductions, with no consistent differences between devices (Table 2).
Table 1.Median (IQR) CFU counts before and after UV-C disinfection by surface type and deviceControl armIntervention armBeforeAfterPercent reductionBeforeAfterPercent reduction p
All CFU (Median [IQR]) Room-Bathroom suite56,096 (17,592–112,182)10,150 (2,430–74,314)48 (23–88)4,255 (1,708–68,319)2,262 (693–21,655)35 (17–82).37Patient room6,288 (349–12,123)910 (35–2,280)85 (66–95)1,422 (176–6,894)180 (0–1,454)93 (70–100).74Bedrails1,890 (368–8,690)234 (0–822)95 (67–100)150 (0–1,550)0 (0–506)99 (67–100).18Overbed table2,646 (720–6,700)49 (0–1,325)91 (62–100)141 (0–1,125)0 (0–180)100 (96–100).82Room sink1,426 (221–3,453)98 (0–915)98 (89–100)228 (0–1,462)15 (0–166)99 (85–100).56Patient bathroom38,984 (15,055–101,426)9,013 (2,390–70,583)68 (27–88)3,425 (1,214–20,820)1,300 (288–8,344)79 (13–89).8Toilet seat3,970 (81–15,818)708 (0–11,822)75 (58–93)73 (0–1,094)0 (0–578)100 (70–100).17Bathroom floor34,205 (15,970–53,079)7,318 (2,632–56,232)70 (21–88)1,954 (476–6,659)805 (13–6,297)71 (95–100).94Bathroom sink2,420 (980–5,764)1,222 (110–2,490)68 (30–84)500 (150–901)135 (0–700)83 (18–100).02 CIP CFU (Median [IQR]) Room-Bathroom suite7,689 (2,898–16,925)3,379 (723–8,653)46 (27–63)954 (501–2,352)194 (18–1,434)60 (38–97).22Patient room3,923 (490–4,888)88 (0–349)98 (45–100)130 (0–964)0 (0–25)87 (0–100).86Bedrails622 (13–3,162)0 (0–0)99 (0–100)0 (0–12)0 (0–0)0 (0–47).73Overbed table382 (0–2,153)0 (0–41)55 (0–100)0 (0–52)0 (0–0)0 (0–66).13Room sink98 (0–896)12 (0–169)53 (0–99)0 (0–215)0 (0–0)0 (0–100)1.0Patient bathroom3,719 (1,118–12,420)2,654 (483–8,079)24 (10–72)766 (68–1,377)167 (18–1,248)22 (0–86).88Toilet seat0 (0–915)0 (0–117)0 (0–69)0 (0–51)0 (0–265)0 (0–59).83Bathroom floor2,270 (448–7,471)768 (39–6,229)32 (60–89)286 (0–908)54 (0–495)28 (0–85).57Bathroom sink786 (198–2,489)132 (0–1,212)59 (12–100)0 (0–147)0 (0–37)0 (0–42).14
Table 2.Proportion of surfaces positive for clinically important pathogens before and after UV-C disinfection by surface type, device, and speciesControl armIntervention armBefore N (%)After N (%)Before N (%)After N (%) p
Overall, Presence of any CIP Room-Bathroom suite61 (73)41 (49)45 (48)32 (34).83Patient Room27 (64)15 (36)20 (43)9 (19).56Bedrails10 (71)3 (21)4 (27)2 (13).58Overbed table8 (57)5 (36)8 (50)3 (19).62Room sink9 (64)7 (50)8 (50)4 (25).34Patient bathroom34 (81)26 (62)25 (53)23 (49).17Toilet seat7 (50)5 (36)6 (38)7 (44).46Bathroom floor14 (100)12 (86)12 (75)11 (69)1.00Bathroom sink13 (93)9 (64)7 (47)5 (33)1.00 ** S. aureus ** Room-Bathroom suite40 (48)21 (25)17 (18)8 (9).78Patient room20 (48)4 (10)7 (15)4 (9).15Bedrails6 (43)1 (7)3 (20)1 (7)1.00Overbed table8 (57)2 (14)3 (19)3 (19).06Room sink6 (43)1 (7)1 (6)0 (0)1.00Patient bathroom20 (48)17 (40)10 (21)4 (9).03Toilet seat4 (29)4 (29)4 (25)1 (6).14Bathroom floor10 (71)9 (64)6 (38)3 (19).12Bathroom sink6 (43)4 (29)0 (0)0 (0)1.00 ** Enterococcus spp. ** Room-Bathroom suite17 (20)11 (13)19 (20)11 (12).74Patient room5 (12)2 (5)6 (13)1 (2).55Bedrails2 (14)2 (14)2 (13)0 (0).33Overbed table1 (7)0 (0)2 (12)0 (0)1.00Room sink2 (14)0 (0)2 (12)1 (6)1.00Patient bathroom12 (29)9 (21)13 (28)10 (21)1.00Toilet seat1 (7)0 (0)3 (19)4 (25).20Bathroom floor8 (57)7 (50)7 (44)4 (25).28Bathroom sink3 (21)2 (14)3 (20)2 (13)1.00 Enterobacterales Room-Bathroom suite31 (37)25 (30)19 (20)20 (21).07Patient room11 (26)12 (29)9 (19)5 (11).02Bedrails3 (21)1 (7)0 (0)1 (7)1.00Overbed table2 (14)4 (29)2 (12)0 (0).07Room sink6 (43)7 (50)7 (44)4 (25).19Patient bathroom20 (48)13 (31)10 (21)15 (32).01Toilet seat2 (14)1 (7)1 (6)4 (25).33Bathroom floor10 (71)6 (43)6 (38)6 (38).23Bathroom sink8 (57)6 (43)3 (20)5 (33).49 ** C. difficile ** Room-Bathroom suite7 (8)4 (5)7 (7)3 (3)1.00Patient room2 (5)2 (5)3 (6)0 (0).10Bedrails0 (0)0 (0)0 (0)0 (0)1.00Overbed table0 (0)1 (7)2 (12)0 (0).33Room sink2 (14)1 (7)1 (6)0 (0)1.00Patient bathroom5 (12)2 (5)4 (9)3 (6).52Toilet seat2 (14)0 (0)0 (0)0 (0)1.00Bathroom floor1 (7)2 (14)1 (6)3 (19)1.00Bathroom sink2 (14)0 (0)3 (20)0 (0)1.00
Inocula were 1.1 × 10^4^ CFU for MRSA and 5.0 × 10 ^ 3 CFU for C. difficile. On average, Legacy reduced MRSA by 8.6 × 10^4^ CFU (96%) compared with 1.09 × 10^4^ CFU (99%) for iQ (p = <.01), while Legacy reduced C. difficile by 1.6 × 10^2^ CFU (3%) compared with 2.0 × 10^3^ CFU (40%) for iQ (P = .02). Additionally, elimination of inoculated pathogens from formica surfaces was more frequent in the intervention arm overall (52% vs 81%; P < .01), and by disinfection cycle; 81% vs 97% (P = .03) for vegetative cycles and 13% vs 44% (P = .03) for spore cycles.
Run times were significantly shorter in the intervention arm overall (42 mins vs 22 mins; P < .01), and by disinfection cycle; 33 minutes vs 16 minutes (P < .01) for vegetative cycles and 54 minutes vs 35 minutes (P < .01) for spore cycles.
Discussion
In this randomized experimental study, both the Tru-D iQ and Tru-D Legacy UV-C systems reduced environmental contamination on high-touch surfaces following patient discharge. The Tru-D iQ system generally achieved greater percent reduction at most sites, significantly so at bathroom sinks, but otherwise showed equivalent reductions. The Tru-D iQ also achieved higher elimination of inoculated pathogens across vegetative and spore cycles, suggesting enhanced performance under controlled conditions. Importantly, the iQ system completed disinfection approximately 20 minutes faster, on average.
Limitations include modest sample size, single-center design, and split-surface sampling, which may not fully represent whole-room efficacy.
In conclusion, the Tru-D iQ UV-C system demonstrated key improvements over the Legacy Tru-D Legacy system. Our findings suggest that the iQ system maintains the Legacy’s efficacy while overcoming prior limitations of bathroom coverage and cycle duration, making next-generation UV-C systems more feasible for routine adoption in acute care settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morgan DJ , Lomotan LL , Agnes K , Mc Grail L , Roghmann MC. et al. Characteristics of healthcare-associated infections contributing to unexpected in-hospital deaths. Infect Control Hosp Epidemiol Off J Soc Hosp Epidemiol Am. 2010;31:864–866. doi:10.1086/655018 PMC 352817820569114 · doi ↗ · pubmed ↗
- 2Magill, SS , Edwards, JR , Bamberg, W , et al. Multistate point-prevalence survey of health care–associated infections. N Engl J Med. 2014;370:1198–1208. doi:10.1056/NEJ Moa 1306801.24670166 PMC 4648343 · doi ↗ · pubmed ↗
- 3Weber DJ , Anderson D , Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis. 2013;26:338–344. doi:10.1097/QCO.0b 013e 3283630 f 04.23743816 · doi ↗ · pubmed ↗
- 4Anderson DJ , Addison R , Lokhnygina Y , et al. The antimicrobial scrub contamination and transmission (ASCOT) trial: a three-arm, blinded, randomized controlled trial with crossover design to determine the efficacy of antimicrobial-impregnated scrubs in preventing healthcare provider contamination. Infect Control Hosp Epidemiol. 2017;38:1147–1154. doi:10.1017/ice.2017.181 28847326 · doi ↗ · pubmed ↗
- 5Warren BG , Turner NA , Addison R , et al. The impact of infection versus colonization on clostridioides difficile environmental contamination in hospitalized patients with diarrhea. Open Forum Infect Dis. 2022;9:ofac 069. doi:10.1093/ofid/ofac 069 35265730 PMC 8900930 · doi ↗ · pubmed ↗
- 6Rock C , Small BA , Hsu YJ , et al. Evaluating accuracy of sampling strategies for fluorescent gel monitoring of patient room cleaning. Infect Control Hosp Epidemiol. 2019;40:794–797. doi:10.1017/ice.2019.102 31172902 PMC 6619417 · doi ↗ · pubmed ↗
- 7Rock C , Cosgrove SE , Keller SC , et al. Using a human factors engineering approach to improve patient room cleaning and disinfection. Infect Control Hosp Epidemiol. 2016;37:1502–1506. doi:10.1017/ice.2016.219 27666398 PMC 6579608 · doi ↗ · pubmed ↗
- 8Warren BG , Barrett A , Graves A , King C , Turner NA , Anderson DJ. An enhanced strategy for daily disinfection in acute care hospital rooms: a randomized clinical trial. JAMA Netw Open. 2022;5:e 2242131. doi:10.1001/jamanetworkopen.2022.42131 36378308 PMC 9667331 · doi ↗ · pubmed ↗