COVID‐19 Infection Before or After Colorectal Cancer Diagnosis Is an Independent Predictor of Mortality and Treatment Delays Compared to Patients Who Never Tested Positive
Imran Qureshi, Steven Rella, Aasma Shaukat

TL;DR
Having COVID-19 before or after a colorectal cancer diagnosis is linked to higher mortality and treatment delays, with socioeconomic factors playing a role.
Contribution
This study identifies that timing of COVID-19 infection relative to colorectal cancer diagnosis independently affects mortality and treatment delays.
Findings
Patients with a history of COVID-19 had higher mortality rates compared to those who never tested positive.
Socioeconomic factors like race, insurance, and income influenced outcomes depending on the timing of the COVID-19 infection.
The findings suggest that CRC patients with a history of COVID-19 may need closer monitoring during treatment.
Abstract
Given COVID‐19's emergence as a new entity and colorectal cancer's (CRC) rising incidence in certain populations, we conducted this retrospective cohort study to determine the link between COVID‐19 and the mortality of those with CRC and how socioeconomic factors influence it. Using the National Cancer Database (NCDB), we used logistic regression to get the odds ratio (OR) for delayed treatment and Cox proportional hazards modeling for each stage to get the adjusted hazard ratios (HR) of mortality. COVID‐19 positivity was associated with higher mortality and delayed treatment. The association of race, ethnicity, insurance, urbanization, comorbidity burden, education levels, and income varied by when the patient tested positive relative to colorectal cancer diagnosis. This implies that vaccinations may be a part of management and that CRC patients who develop COVID‐19 infection may…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
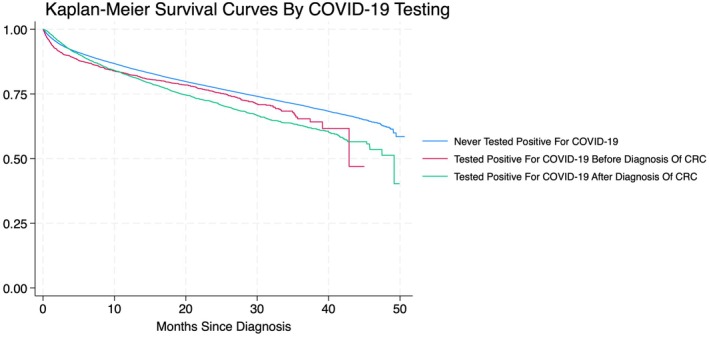 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · COVID-19 Clinical Research Studies · SARS-CoV-2 and COVID-19 Research
COVID‐19 has dramatically transformed the landscape of medicine. According to the World Health Organization (WHO), COVID‐19 was responsible for over 1.8 million deaths worldwide in 2020, a number that newer estimates reveal may be even higher [1]. Although the acute phase of the pandemic has passed, COVID‐19 remains a significant disease that continues to impact individuals globally. Increasing evidence of its long‐term effects, commonly referred to as “long COVID,” suggests that people suffer from health issues even after recovering from the initial infection [2]. Both acute and post‐acute phases of COVID‐19 are linked to complications. Despite vaccination efforts and infection control protocols, all‐cause mortality due to COVID‐19 remains high even after the pandemic [3]. Colorectal cancer (CRC) is the fourth most common cancer in the U.S. [4]. Existing literature reveals how the pandemic disrupted CRC screening, leading to missed or delayed diagnoses and treatment [5, 6]. However, there is a lack of research on how COVID‐19 infection affects the incidence and progression of CRC. There is growing evidence of the oncogenic properties of COVID‐19. Mechanisms, such as inflammation, immune dysregulation, and viral genome integration, are being investigated as potential pathways through which COVID‐19 could influence tumorigenesis [7]. There is also evidence to suggest that cancer care for racial and ethnic minorities was disproportionately affected during the pandemic [8]. We conducted this retrospective cohort study to evaluate the association of COVID‐19 and its temporality to CRC diagnosis on treatment delays, mortality, and disparities in individuals over 18 affected by CRC compared to those who never tested positive.
We queried the National Cancer Database (NCDB) from 2020 and 2021 for patients with CRC, as it contained data regarding COVID‐19 testing based on preadmission or hospital testing from the site that reported the case. NCDB annually reports approximately 70% of newly diagnosed cancer cases from Commission on Cancer–accredited facilities in the U.S. [9]. Patients aged less than 18, not tested for COVID‐19, or who had unknown COVID‐19 test results were excluded. We divided our data into three categories: patients who never tested positive for COVID‐19, patients who tested positive for COVID‐19 for the first time before diagnosis of CRC, and patients who tested positive for COVID‐19 for the first time after diagnosis of CRC. We assessed sociodemographic factors at the time of CRC diagnosis and reported their frequencies. We used univariate and multivariate logistic regression to get the unadjusted and adjusted OR, respectively, along with a 95% confidence interval (CI) and p‐value for delayed treatment initiation, defined as > 6 weeks from diagnosis to initiation of any treatment modality. We fit a Cox proportional hazards model for each stage to get the univariate and multivariate HR of all‐cause mortality, with a 95% CI and p‐value, using patients who never tested positive for COVID‐19 as a reference. For multivariate regression analysis, we used sex, race, ethnicity, insurance status, setting, Charlson‐Deyo Comorbidity score, adults without a high‐school diploma in the patient's ZIP code, and median household income as covariates. Additionally, we assessed the effects of these factors on overall mortality for each of the two groups with COVID‐19 positivity using univariate and multivariate Cox regression. Our model met the proportional hazard assumption, which was tested using the Schoenfeld Residuals Test. We assessed overall survival using the Kaplan–Meier methods and their comparisons using the log‐rank test. An alpha level of 0.05 was considered significant. Statistical analysis was done using StataNow/MP 18.5 for Mac (StataCorp LLC, Texas, USA).
There were a total of 112,731 patients in our dataset, of which 103,913 (92.18%) never tested positive for COVID‐19, 2668 (2.37%) tested positive for COVID‐19 before diagnosis of CRC, and 6150 (5.46%) tested positive for COVID‐19 after diagnosis of CRC (Table 1). The median ages in our cohorts were 66 years (Q1–Q3: 55–76 years), 65 years (Q1–Q3: 53–76 years), and 63 years (Q1–Q3: 52–74 years), respectively. Those with COVID‐19 before diagnosis of CRC were diagnosed a median of 80 days prior (Q1–Q3: 20–203 days), whereas those with COVID‐19 after diagnosis were diagnosed a median of 118 days after (Q1–Q3: 44–241 days). We observed that those with COVID‐19 before diagnosis did not have a significant delay in receiving treatment for their malignancy (OR = 0.94, 95% CI = 0.84–1.05, p = 0.266), whereas those with COVID‐19 after diagnosis did (OR = 1.52, 95% CI = 1.43–1.63, p < 0.001) compared to those that never tested positive for COVID‐19. Both patients with COVID‐19 before and after diagnosis demonstrated an increase in all‐cause mortality (HR = 1.10, 95% CI = 1.00–1.20, p = 0.046 and HR = 1.18, 95% CI = 1.12–1.25, p < 0.001, respectively) compared to those that never tested positive for COVID‐19 (Figure 1). However, when stratified by stage of CRC, those with COVID‐19 after diagnosis of stage 1 (HR = 1.26, 95% CI = 1.01–1.56, p = 0.039), stage 2 (HR = 1.40, 95% CI = 1.21–1.61, p < 0.001), and stage 3 CRC (HR = 1.16, 95% CI = 1.04–1.30, p < 0.001) had increased mortality. No significant differences in mortality were noted in stage 4 CRC, regardless of COVID‐19 infection or in patients with COVID‐19 before diagnosis by stage of CRC.
Among those who had COVID‐19 before diagnosis, there was no significant difference in mortality by sex or by setting compared to a metropolitan setting. American Indians with COVID‐19 before diagnosis had higher mortality than their white counterparts (HR = 2.32, 95% CI = 1.19–4.55, p = 0.014). Hispanic patients who had COVID‐19 before diagnosis had reduced mortality (HR = 0.67, 95% CI = 0.48–0.94, p = 0.020) compared to non‐Hispanics. There was also increased mortality among uninsured (HR = 1.62, 95% CI = 1.00–2.63, p = 0.050), Medicaid (HR = 1.44, 95% CI = 1.02–2.02, p = 0.036), and Medicare patients (HR = 1.41, 95% CI = 1.08–1.84, p = 0.012) compared to patients with private insurance. Patients with a Charlson‐Deyo comorbidity index of ≥ 3 had significantly increased mortality (HR = 1.91, 95% CI = 1.52–2.40, p < 0.001). Areas with 5.0%–9.0% high school non‐graduates had lower mortality (HR = 0.75, 95% CI = 0.58–0.96, p = 0.021) than areas with < 5.0% non‐graduates. Furthermore, patients with a median household income < 74,063. The log‐rank test for Kaplan–Meier methods and their comparisons showed a p‐value of 0.001, demonstrating a significant difference in overall survival among our three cohorts.
We also assessed predictors of higher mortality in those who tested positive for COVID‐19 after being diagnosed with CRC. Like those with COVID‐19 before diagnosis, there was no significant difference in mortality between sexes. For race, only black patients had higher mortality when compared to whites (HR = 1.30, 95% CI = 1.12–1.51, p < 0.001). Unlike our other group, there was also no difference in mortality in Hispanics compared to non‐Hispanics (HR = 0.86, 95% CI = 0.70–1.05, p = 0.146). However, similar to our other group, there was increased mortality among uninsured (HR = 1.57, 95% CI = 1.16–2.12, p = 0.003), those with Medicaid (HR = 1.75, 95% CI = 1.46–2.10, p < 0.001), and Medicare patients (HR = 1.29, 95% CI = 1.11–1.51, p = 0.001). Residing in an urban setting was associated with lower mortality (HR = 0.86, 95% CI = 0.74–0.99, p = 0.044) than residing in metropolitan areas. There was a significant increase in mortality for Charlson‐Deyo comorbidity index of 2 (HR = 1.35, 95% CI = 1.14–1.60, p < 0.001) and ≥ 3 (HR = 1.45, 95% CI = 1.24–1.69, p < 0.001). Unlike those with COVID‐19 before CRC diagnosis, this group had increased mortality in patients from areas with ≥ 15.3% non‐graduates (HR = 1.27, 95% CI = 1.04–1.55, p = 0.019). We also observed decreased mortality in patients in the median household income bracket of 74,062 (HR = 0.86, 95% CI = 0.74–0.99, p = 0.038).
Our findings suggest that CRC patients with COVID‐19 have worse outcomes than those who have never tested positive for it. Even though both patients with COVID‐19 before diagnosis and after diagnosis of CRC had higher overall mortality, when stratified by stage, only those with COVID‐19 after diagnosis of stage 1, 2, or 3 CRC had a higher mortality. There was no significant difference in mortality for stage 4 disease, likely because these patients had a poor prognosis independent of the COVID‐19 infection. Those who tested positive with COVID‐19 after CRC also experienced treatment delays consistent with what is known about the effect of COVID‐19 infection on cancer care [10]. Violante et al. reported that patients in the “post‐COVID” era presented with advanced‐stage CRC and noted significant staging inequities [11]. We noted in our study that race, ethnicity, setting, education status, and income had a variable association with mortality depending on when patients tested positive. Interestingly, Hispanic patients with COVID‐19 before CRC had decreased mortality even though they had decreased CRC screening rates during this time [12]. This can be explained by selection bias or lack of power, but may need further exploration. What was consistent between both groups was that patients who were uninsured, had Medicare, or had Medicaid had higher mortality than their counterparts with private insurance. This aligns with a study looking at gynecological cancer by Lara et al. [13]. Another consistent finding was that patients with a higher comorbidity burden had higher mortality. Patients with a higher comorbidity burden have higher mortality anyway, but this may also be due to COVID‐19 exacerbating chronic conditions in addition to possibly its intrinsic effects on CRC [14].
Our study is unique in that it looks at outcomes and predictors for COVID‐19 exclusively in the “post‐COVID” era and only includes patients who were tested and had known results. Our study was limited in that it looked over a relatively short timeframe, 2 years. There is also a possibility of misclassification bias, as patients may have tested positive previously and later tested negative at the facility reporting the case, as well as immortal time bias in patients who died shortly after diagnosis. Furthermore, accessibility to healthcare could be dependent on the wave of COVID‐19, which may be a potential confounder that cannot be quantified with our dataset. It is unclear whether COVID‐19 is a causal agent for this worse prognosis or if COVID‐19 infection indicates poor health outcomes, as patients who get this infection tend to have poorer outcomes anyway [15]. These findings imply that vaccinations may be part of the recommended treatment guidelines. Further, patients with CRC who develop COVID‐19 infection may warrant closer follow‐up during treatment. Future research needs to explore the interaction of COVID‐19 infection and treatment efficacy and toxicity, and other factors on the causal pathway to poor outcomes.
Author Contributions
Imran Qureshi: conceptualization, investigation, writing – original draft, methodology, visualization, writing – review and editing, software, formal analysis, data curation. Steven Rella: writing – original draft, writing – review and editing, visualization. Aasma Shaukat: supervision, writing – review and editing, methodology, writing – original draft, conceptualization.
Funding
The authors have nothing to report.
Ethics Statement
Institutional review board was exempted for this study as it does not directly involve humans.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO , “The True Death Toll of COVID‐19: Estimating Global Excess Mortality,” https://www.who.int/data/stories/the‐true‐death‐toll‐of‐covid‐19‐estimating‐global‐excess‐mortality.
- 2A. V. Raveendran , R. Jayadevan , and S. Sashidharan , “Long COVID: An Overview,” Diabetes & Metabolic Syndrome 15, no. 3 (2021): 869–875, 10.1016/j.dsx.2021.04.007.33892403 PMC 8056514 · doi ↗ · pubmed ↗
- 3M. Saskia , H. Marcel , H. Minke , and K. Gertjan , “Excess Mortality Across Countries in the Western World Since the COVID‐19 Pandemic: ‘Our World in Data’ Estimates of January 2020 to December 2022,” BMJ Public Health 2, no. 1 (2024): e 000282, 10.1136/bmjph-2023-000282. · doi ↗
- 4R. L. Siegel , A. N. Giaquinto , and A. Jemal “Cancer statistics, 2024,” CA: A Cancer Journal for Clinicians 74, no. 1 (2024): 12–49, 10.3322/caac.21820.38230766 · doi ↗ · pubmed ↗
- 5R. van den Puttelaar , I. Lansdorp‐Vogelaar , A. I. Hahn , et al., “Impact and Recovery From COVID‐19–Related Disruptions in Colorectal Cancer Screening and Care in the US: A Scenario Analysis,” Cancer Epidemiology, Biomarkers & Prevention 32, no. 1 (2023): 22–29, 10.1158/1055-9965.Epi-22-0544.PMC 982710936215205 · doi ↗ · pubmed ↗
- 6A. Mazidimoradi , F. Hadavandsiri , Z. Momenimovahed , and H. Salehiniya , “Impact of the COVID‐19 Pandemic on Colorectal Cancer Diagnosis and Treatment: A Systematic Review,” Journal of Gastrointestinal Cancer 54, no. 1 (2023): 171–187, 10.1007/s 12029-021-00752-5.34843058 PMC 8628028 · doi ↗ · pubmed ↗
- 7N. Ogarek , P. Oboza , M. Olszanecka‐Glinianowicz , and P. Kocelak , “SARS‐Co V‐2 Infection as a Potential Risk Factor for the Development of Cancer,” Frontiers in Molecular Biosciences 10 (2023): 1260776, 10.3389/fmolb.2023.1260776.37753372 PMC 10518417 · doi ↗ · pubmed ↗
- 8M. I. Patel , J. M. Ferguson , E. Castro , et al., “Racial and Ethnic Disparities in Cancer Care During the COVID‐19 Pandemic,” JAMA Network Open 5, no. 7 (2022): e 2222009, 10.1001/jamanetworkopen.2022.22009.35834248 PMC 9284331 · doi ↗ · pubmed ↗