Renal Sarcoidosis With Increased 1,25(OH)2D3 Production via CYP27B1-Expressing Epithelioid Granuloma: A Case Report and Review
Shinya Harada, Makoto Abe, Yuko Ono, Kazuyuki Ishida, Akihiro Tojo

TL;DR
A case of kidney sarcoidosis showed increased vitamin D production by granulomas, which may help monitor treatment.
Contribution
This case report identifies CYP27B1-expressing granulomas as a source of 1,25(OH)2D3 in renal sarcoidosis.
Findings
Renal sarcoidosis was associated with elevated 1,25(OH)2D3 levels due to CYP27B1-expressing granulomas.
Glucocorticoid treatment reduced 1,25(OH)2D3 levels but they fluctuated with treatment tapering.
Plasma 1,25(OH)2D3 may serve as a treatment indicator for renal sarcoidosis.
Abstract
Sarcoidosis can cause acute kidney injury (AKI) through hypercalcemia and granulomatous interstitial nephritis. However, the detailed mechanisms linking intra-renal granuloma activity and AKI are not fully elucidated. A 69-year-old woman presented with AKI associated with elevated 1,25(OH)2D3 levels. A renal biopsy revealed tubulointerstitial nephritis with the presence of epithelioid granulomas and multinucleated giant cells. Immunohistochemistry showed that these cells expressed 25-hydroxyvitamin D-1 alpha hydroxylase (CYP27B1). Glucocorticoid therapy rapidly improved 1,25(OH)2D3 levels at initiation, but these levels fluctuated in relation to renal function during glucocorticoid tapering. Plasma 1,25(OH)2D3 may be produced by CYP27B1 expressed in renal granulomas and serves as an indicator for the treatment of renal sarcoidosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
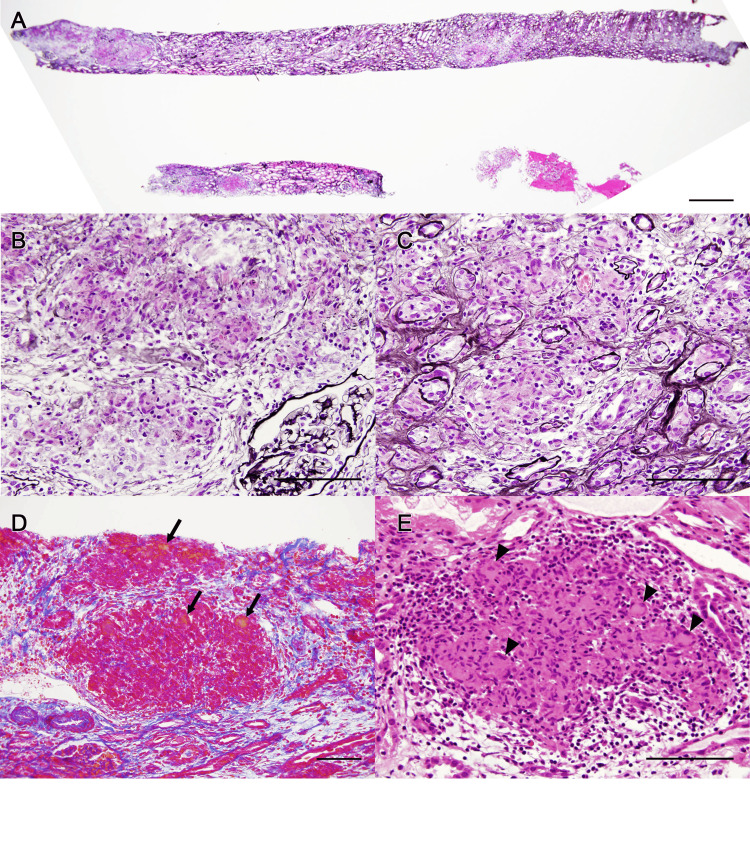 Figure 1
Figure 1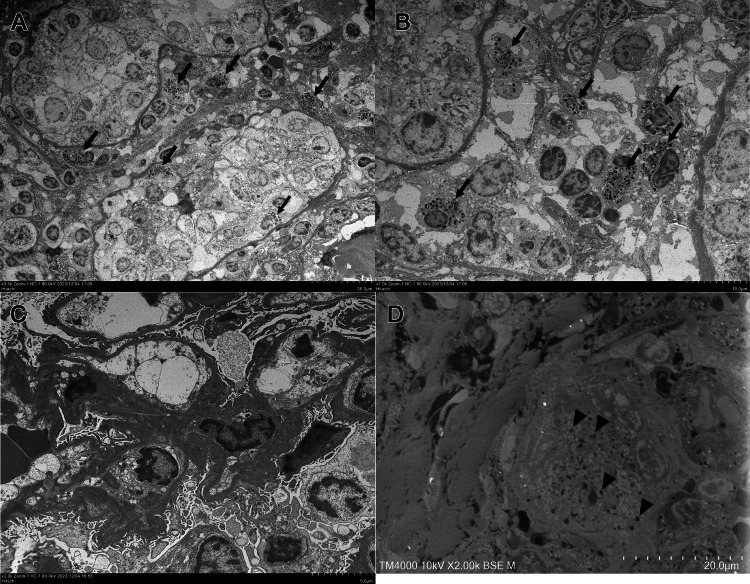 Figure 2
Figure 2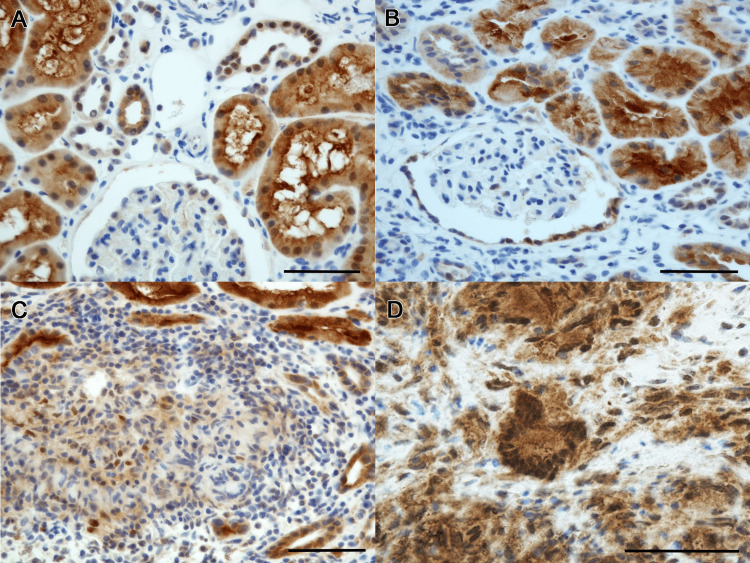 Figure 3
Figure 3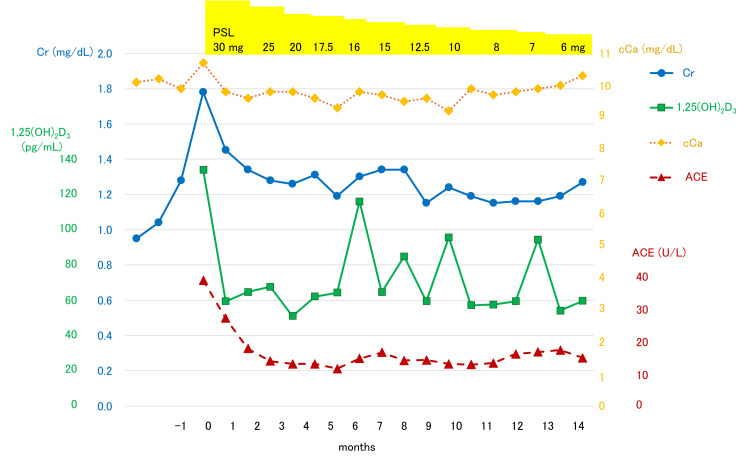 Figure 4
Figure 4| Investigation | Patient value | Normal range |
| Complete blood count | ||
| WBC (×109/L) | 7.00 | 3.30-8.60 |
| RBC (×1012/L) | 3.50 | 3.86-4.92 |
| Hb (g/dL) | 10.8 | 11.6-14.8 |
| Plt (×109/L) | 318 | 158-348 |
| Serum biochemistry | ||
| Albumin (g/dL) | 3.9 | 4.1-5.1 |
| BUN (mg/dL) | 38.1 | 8-20 |
| Cr (mg/dL) | 1.86 | 0.46-0.79 |
| eGFR (mL/min/1.73m2) | 22.6 | >60 |
| Uric acid (mg/dL) | 6.9 | 2.6-7.0 |
| Na (mmol/L) | 137 | 138-145 |
| K (mmol/L) | 4.5 | 3.6-4.8 |
| Cl (mmol/L) | 102 | 101-108 |
| cCa (mg/dL) | 10.7 | 8.8-10.1 |
| IP (mg/dL) | 4.5 | 2.7-4.6 |
| 1,25(OH)2D3 (pg/mL) | 134 | 20-60 |
| iPTH (pg/mL) | 12.0 | 10-65 |
| PTHrP (pmol/L) | <1.0 | <1.3 |
| Lysozyme (µg/mL) | 30.0 | 4.3-11.5 |
| sIL-2R (U/mL) | 3,564 | 220-530 |
| ACE (IU/L) | 39.2 | 8.3-21.4 |
| Urinalysis | ||
| Specific gravity | 1.009 | 1.010-1.030 |
| Urinary protein excretion (g/gCr) | 0.10 | <0.15 |
| Urinary red blood cells (/HPF) | <1 | <5 |
| Urinary white blood cells (/HPF) | 1-4 | <5 |
| NAG (IU/L) | 3.6 | <8.0 |
| Urinary β2-MG (µg/L) | 5,350 | <230 |
| Author | Age, sex | Cr (mg/dL) | eGFR (mL/min/1.73m2) | Ca (mg/dL) | 1,25(OH)2D3 (pg/mL) | Therapy | Post Cr (mg/dL) | Post eGFR (mL/min/1.73m2) | Post Ca (mg/dL) | Post 1,25(0H)2D3 (pg/mL) |
| Manjunath et al. (2013) [ | 43, male | 2.7 | - | 11.2 | 75 | PSL 40 mg | 1.9 | - | - | - |
| Unsal et al. (2013) [ | 30, male | 2.2 | - | 11.5 | 34 | PSL 1 mg/kg, chloroquine 250 mg | 1.3 | - | 11.3 | 37 |
| Toriu et al. (2019) [ | 54, female | - | 67.4 | 9.3 | 68.2 | PSL 20-40 mg | - | 67.1 | 9.3 | 47.5 |
| 46, male | - | 44.7 | 9.1 | 58.0 | PSL 20-40 mg | - | 45.6 | 8.9 | 39.0 | |
| 72, male | - | 31.8 | 10.3 | 41.1 | PSL 20-40 mg | - | 32.1 | 10.0 | 28.0 | |
| 20, male | - | 34.2 | 10.4 | 79.3 | PSL 20-40 mg | - | 28.7 | 9.5 | 48.3 | |
| 82, male | - | 4.2 | 9.6 | 49.4 | PSL 20-40 mg | - | 4.3 | 8.4 | 23.2 | |
| 36, male | - | 62.5 | 10.0 | 42.1 | PSL 20-40 mg | - | 52.5 | 9.4 | 52.8 | |
| 75, female | - | 10.2 | 12.5 | 34.6 | PSL 20-40 mg | - | 24.9 | 9.8 | 23.7 | |
| 76, male | - | 5.5 | 9.7 | 33.0 | PSL 20-40 mg | - | 9.0 | 9.2 | 18.0 | |
| 74, female | - | 46.8 | 9.7 | 30.0 | PSL 20-40 mg | - | 56.8 | 9.4 | 18.9 | |
| Iwazu et al. (2021) [ | 42, male | 1.82 | - | 12.0 | 112 | PSL 35 mg | 1.1 | - | 9.9 | 60 |
| Mio et al. (2022) [ | 62, male | 2.27 | 24.2 | 13.2 | 158 | PSL 25 mg | 1.5 | - | 10.1 | 32.0 |
| Present case | 69, female | 1.78 | 22.6 | 10.7 | 134 | PSL 30 mg | 1.27 | 32.6 | 10.3 | 59.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · S100 Proteins and Annexins
Introduction
Sarcoidosis is a systemic inflammatory disease of unknown etiology. In 90% of cases, the disease presents with non-caseating granulomas in the lungs and mediastinal lymph nodes; however, it is known to affect any organ in the body [1,2]. In particular, hypercalcemia is observed in 10% of patients with sarcoidosis and has been shown to cause acute kidney injury (AKI) [1,3]. This is thought to be due to an increase in 1,25(OH)2_D_3; however, the cause and pathological significance remain unclear [4]. As demonstrated in a previous study that highlighted how microscopic analysis can uncover systemic mechanisms of organ injury across diverse disease contexts [5], histopathological examination plays a pivotal role in elucidating the pathophysiological mechanisms underlying sarcoidosis and its organ-specific manifestations. Detailed tissue evaluation not only confirms granulomatous inflammation but also clarifies associated metabolic or immune-mediated alterations contributing to renal dysfunction. We report a case of renal sarcoidosis in which expression of 25-hydroxyvitamin D-1 alpha hydroxylase (CYP27B1) in epithelioid granulomas and multinucleated giant cells led to 1,25(OH)2_D_3 elevation, resulting in AKI.
Case presentation
A 69-year-old woman visited our hospital complaining of edema in her eyelids and legs. She had been in good health, except for surgeries for cholelithiasis and appendicitis seven years prior. She had normal renal function and no family history of kidney disease. Her blood pressure was 120/70 mmHg, heart rate was 74/min, body temperature was 36.7°C, and oxygen saturation (SpO_2_) was 98% (on room air). There was mild edema in her legs, but heart and lung sounds were normal, and there was no obvious cervical lymph node swelling or goiter. Urinalysis revealed a low specific gravity of 1.009, consistent with hyposthenuria, and no proteinuria or hematuria was observed. Urinary N-acetyl-β-D-glucosaminidase (NAG) was normal at 3.6 IU/L, but urinary β_2_-microglobulin (β_2_-MG) was elevated at 5,350 µg/L. Renal function was declining, with a serum creatinine (Cr) of 1.78 mg/dL and an estimated glomerular filtration rate (eGFR) of 22.6 mL/min/1.73 m^2^, calculated using the Japanese Society of Nephrology (JSN) equation for females (eGFR = 194 × Cr^-1.094 ^× Age^-0.287^ × 0.739). The corrected serum calcium (cCa) level was slightly elevated at 10.7 mg/dL with inorganic phosphorus (IP) of 4.5 mg/dL associated with an elevated 1,25(OH)2_D_3 level of 134 pg/mL (normal range: 20-60 pg/mL). While the intact parathyroid hormone (iPTH) level was suppressed at 12.0 pg/mL, the parathyroid hormone-related peptide (PTHrP) was less than 1.0 pmol/L. Elevated levels of plasma lysozyme of 30.0 µg/mL (4.3-11.5 µg/mL), soluble interleukin-2 receptor (sIL-2R) of 3,564 U/mL (220-530 U/ml), and angiotensin-converting enzyme (ACE) of 39.2 IU/L (8.3-21.4 IU/L) were consistent with sarcoidosis. Table 1 presents the laboratory findings for this case.
Computed tomography scans of the chest and abdomen revealed significant swelling of the mediastinal and right hilar lymph nodes. A bronchoscopic lymph node biopsy showed non-caseating epithelioid cell granulomas, indicating a diagnosis of pulmonary sarcoidosis.
Because of progressive renal dysfunction, a history of pulmonary sarcoidosis, and elevated tubular injury markers, a renal biopsy was performed. The renal biopsy revealed tubulointerstitial nephritis associated with epithelioid granulomas and multinucleated giant cells. Six glomeruli were normal, with one showing global sclerosis (Figure 1). AZAN (azocarmine, aniline blue, and orange G) staining revealed an accumulation of orange-stained substance in the granulomatous areas (Figure 1D). Immunofluorescence staining was negative for IgG, IgA, IgM, and C3 in the glomeruli and lesions. Electron microscopy revealed no foot process effacement or electron-dense deposits (Figure 2C), and the epithelioid granulomas and multinucleated giant cells in the interstitium contained granular material 5-10 nm in size (Figures 2B, 2D). CYP27B1 renal expression was observed in the proximal tubules in thin basement membrane disease as a control (Figure 3A). In the present case, CYP27B1 expression was observed in both the epithelioid granuloma cells and the multinucleated giant cells (Figures 3B-3D).
Light microscopy of renal biopsy samples.(A-C) PAM staining shows cellular proliferation in the tubulointerstitium without changes in the glomerulus. (D) AZAN staining shows accumulation of orange substance (arrow). (E) HE staining shows epithelioid cell granulomas and multinucleated giant cells (arrowhead). Bars: A = 1 mm, B-E = 100 µm.PAM: periodic acid methenamine silver; AZAN: azocarmine, aniline blue, and orange G; HE: hematoxylin and eosin.
Electron microscopy of renal biopsy samples.(A, B) Transmission electron microscopy shows accumulation of granular material in interstitial infiltrating cells (arrow). (C) No electron-dense deposits in the glomerulus or disappearance of the foot process are observed. (D) Low-vacuum scanning electron microscopy shows similar granular material in multinucleated giant cells (arrowhead).
Immunohistochemistry for 25-hydroxyvitamin D-1 alpha hydroxylase (CYP27B1) using anti-human CYP27B1 antibody (Sigma-Aldrich, Merck KGaA, Darmstadt, Germany) with 1:400 dilution.Normal control staining in proximal tubules in thin basement membrane disease (A). In the present case (B-D), strong CYP27B1 expression is observed in epithelioid cell granulomas and multinucleated giant cells (C, D) in addition to proximal tubules (B). Bars: 100 µm.
The patient was diagnosed with granulomatous interstitial nephritis due to sarcoidosis and was treated with 30 mg of prednisolone. The changes in serum Cr, cCa, 1,25(OH)2_D_3, and ACE during treatment are summarized in Figure 4. Serum calcium concentrations quickly returned to normal and remained within the normal range, whereas fluctuations in serum 1,25(OH)2_D_3 concentrations correlated with fluctuations in serum creatinine concentrations during prednisolone tapering. Mild renal dysfunction remained with Cr at 1.27 mg/dL, but serum cCa and ACE normalized with 6 mg prednisolone.
Changes in serum Cr, cCa, 1,25(OH)2D3, and ACE during treatment with prednisolone.PSL: prednisolone; Cr: serum creatinine; cCa: corrected calcium; ACE: angiotensin-converting enzyme.
Discussion
In this case report, we have demonstrated enhanced expression of CYP27B1 in the granuloma cells and multinucleated giant cells of renal sarcoidosis, which is the most plausible mechanism for the observed increased 1,25(OH)2_D_3 production. Approximately 10% of sarcoidosis cases are associated with hypercalcemia via increased CYP27B1 [6]. Inactive form of vitamin D_3_ synthesized in the skin is metabolized in the liver to 25(OH)D_3_, which is then hydroxylated by CYP27B1 to the active form of 1,25(OH)2_D_3. It has been believed that increased extrarenal CYP27B1 leads to overproduction of 1,25(OH)2_D_3, causing hypercalcemia in sarcoidosis [7]. In the present case, we showed an increased expression of CYP27B1 in renal sarcoidosis.
Renal sarcoidosis is a rare form of sarcoidosis characterized by granulomatous inflammation confined to the renal cortex and accounts for 0.7-0.9% of sarcoidosis cases [8]. The degree of renal dysfunction varies in sarcoidosis treated with glucocorticoid therapy [7]. The causes of kidney damage include not only granulomatous tubulointerstitial nephritis, but also dehydration or renal stones due to hypercalcemia [8,9].
CYP27B1 is primarily expressed in the proximal tubules of the kidney, and in the placenta during pregnancy [10,11]. It is also expressed in granulomatous conditions, in which macrophages activate vitamin D_3_ by producing CYP27B1 outside the kidney [12]. Cases of renal sarcoidosis with increased 1,25(OH)2_D_3 and AKI are summarized in Table 2. In some of these cases, the serum calcium concentration was not high enough to cause dehydration [13-17]. Additionally, glucocorticoid treatment reduced the serum calcium to the normal level, but renal function was not restored to the normal level in some cases, including the present case [15-17]. Thus, the persistence of renal dysfunction after the normalization of serum calcium suggests that AKI in renal sarcoidosis cannot be attributed solely to hypercalcemia and is likely also due to direct granulomatous inflammation. We revealed increased CYP27B1 expression in epithelioid granulomas and multinucleated giant cells (Figures 3C, 3D) with secretory granules (Figures 2B, 2D), which may release 1,25(OH)2_D_3. Glucocorticoid therapy inhibits granuloma formation and reduces CYP27B1 expression in granulomatous areas of cutaneous sarcoidosis [18]. Therefore, we believe that serum 1,25(OH)2_D_3 can indicate granuloma formation and renal sarcoidosis disease activity. Sustained elevation of 1,25(OH)2_D_3 requires chronic treatment [19], and renal damage increases when 1,25(OH)2_D_3 is 30 pg/mL or higher [20]. In fact, a re-elevation of 1,25(OH)2_D_3 was observed during the gradual prednisolone tapering in the present case. Therefore, we propose that serum 1,25(OH)2_D_3 levels can be an important indicator for the treatment of renal sarcoidosis.
Conclusions
In this case, renal dysfunction persisted even after serum calcium levels were normalized. Plasma 1,25(OH)2_D_3 concentrations increased during the course of prednisolone tapering. We directly demonstrated CYP27B1 expression within renal granulomas, providing a pathological basis for the elevated 1,25(OH)2_D_3. Monitoring 1,25(OH)2_D_3 levels may therefore serve as a valuable indicator of granulomatous disease activity to guide treatment in renal sarcoidosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcoidosis N Engl J Med Iannuzzi MC Rybicki BA Teirstein AS 2153216535720071803276510.1056/NEJ Mra 071714 · doi ↗ · pubmed ↗
- 2Sarcoidosis: a general overview Adv Rheumatol Neves FS Pereira IA Sztajnbok F Neto NS 576420243913519010.1186/s 42358-024-00381-z · doi ↗ · pubmed ↗
- 3Sarcoidosis: the nephrologist's perspective Am J Kidney Dis Berliner AR Haas M Choi MJ 8568704820061706000910.1053/j.ajkd.2006.07.022 · doi ↗ · pubmed ↗
- 4HLA-DRB 1 alleles associate with hypercalcemia in sarcoidosis Respir Med Werner J Rivera N Grunewald J Eklund A Iseda T Darlington P Kullberg S 10653718720213432522710.1016/j.rmed.2021.106537 · doi ↗ · pubmed ↗
- 5Histopathological changes in the human tissues in various types of poisoning: a cross-sectional autopsy study Toxicol Rep Kanani J Sheikh MI Jain S Mesuriya S 1017711320243946909910.1016/j.toxrep.2024.101771 PMC 11513817 · doi ↗ · pubmed ↗
- 6Vitamin D, calcium, and sarcoidosis Chest Sharma OP 5355391091996862073210.1378/chest.109.2.535 · doi ↗ · pubmed ↗
- 7Renal sarcoidosis: clinical, laboratory, and histologic presentation and outcome in 47 patients Medicine (Baltimore) Mahévas M Lescure FX Boffa JJ 981068820091928270010.1097/MD.0b 013e 31819 de 50f · doi ↗ · pubmed ↗
- 8Renal sarcoidosis Nephrol Dial Transplant Mehta S Lightle A Judson MA 8038103820233586787410.1093/ndt/gfac 219 · doi ↗ · pubmed ↗