Chemotherapy-related hand–foot syndrome and hand–foot skin reaction: a review of management and possible approaches for Asian patients by the Japanese pharmacist-led oncodermatology study team
Yohei Iimura, Hirotoshi Iihara, Yoshitaka Saito, Hisanaga Nomura, Takuya Iwamoto, Mayumi Kotera, Yusuke Tsuchiya, Tatsuya Sumiya, Mariko Kono, Daisuke Hirate, Tomohiro Kurokawa, Toshinobu Hayashi, Hironobu Hashimoto, Junichi Higuchi, Ryuta Urakawa, Hiroyuki Saotome

TL;DR
This review addresses hand-foot syndrome in Asian cancer patients, offering tailored prevention and treatment strategies based on their unique skin characteristics.
Contribution
Provides evidence-based recommendations for managing hand-foot syndrome in Asian patients, considering their distinct skin type.
Findings
Topical diclofenac is suggested as a novel prevention strategy for capecitabine-induced hand-foot syndrome.
High-potency topical steroids and antiseptic solutions are not recommended for Asian patients.
Asian skin differences necessitate tailored treatment approaches compared to European and American guidelines.
Abstract
Hand–foot syndrome (HFS) and hand–foot skin reaction (HFSR) are adverse effects induced by cytotoxic chemotherapeutic agents, such as capecitabine, pegylated liposomal doxorubicin, and multi-kinase inhibitors. HFS/HFSR can significantly reduce patients’ quality of life and impact cancer treatment intensity due to severe pain in the hands and feet. Although several recommendations and guidelines have been published, most focus on European and American populations, with no management guidelines specifically addressing Asian patients. Given that Asian skin types differ from those of Europeans and Americans, treatment recommendations tailored to Asian populations are needed. A narrative review of published articles retrieved following a systematic search of PubMed, the Cochrane Library, Medical Online, and Ichushi-Web between January 2000 and March 2025 was conducted. The search strategy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
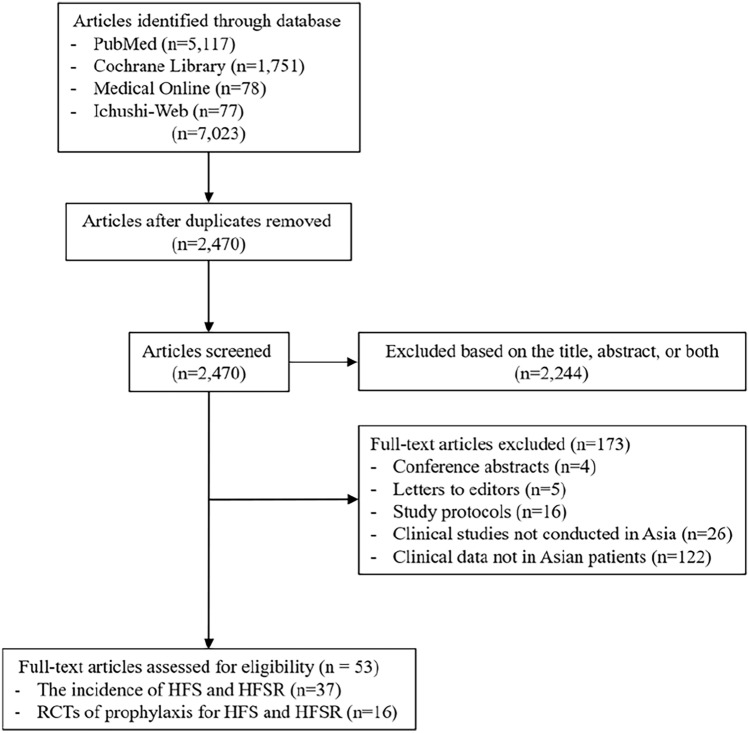 Figure 1
Figure 1- —Japan Agency for Medical Research
- —The University of Tokyo
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-related skin toxicity · Cancer Treatment and Pharmacology · Colorectal Cancer Treatments and Studies
Introduction
Hand–foot syndrome (HFS), also known as palmar–plantar erythrodysesthesia syndrome, is a cutaneous adverse event associated with cytotoxic agents (CTx) and BRAF inhibitors. HFS is characterized by pain, swelling, numbness, tingling, or hands and feet erythema, and was first described in association with mitotane administration [1]. Among chemotherapeutic agents, capecitabine and pegylated liposomal doxorubicin showed associations with a high severe skin toxicity incidence. Clinically significant HFS (grade ≥ 2), presenting with swelling, blistering, desquamation, or ulceration, can markedly impair patients’ quality of life (QOL) [2]. However, multi-kinase inhibitors (MKIs) are associated with hand–foot skin reaction (HFSR), a distinct but related dermatologic toxicity affecting the palms and/or soles [3]. Compared with HFS, HFSR typically presents earlier during treatment and is often of greater severity [4, 5].
The pathogenesis of HFS/HFSR differs. HFS is diffusely expressed in the palms and the soles, whereas HFSR is often localized in the areas of stress [6]. Additionally, by onset, HFSR may develop earlier than HFS. The mechanism involved HFS development differs from that of HFSR. Regarding HFS [6], (1) inhibition of proliferation of skin basal cells, (2) drug secretion from eccrine sweat glands, (3) involvement of drug degradation products, and (4) inflammatory response caused by interleukin (IL)−1α, IL-1β, IL-6, and reactive oxygen species have been suspected [7–10]. By contrast, HFSR is induced by the simultaneous inhibition of different receptors, which alters the structure of the microvasculature and causes abnormal endothelial and vascular repair mechanisms [11, 12]. Differential preventive and treatment strategies for HFS/HFSR are required because they are mutually exclusive. Because HFS has a disseminated onset, hands and feet should be cared for. In contrast, HFSR occurs in specific stressed or damaged areas, by any factor (traumatic or chemical stress). Therefore, intensive care is required in stress-prone areas.
Several evidenced-based clinical guidelines exist on patients in the United States and Europe [13, 14]. However, none are available for patients undergoing HFS or HFSR in Asia. Particularly, Asians are prone to developing HFS/HFSR caused by chemotherapeutic agents [15–17]. Therefore, Asian patients require suitable preventive and treatment strategies for HFS/HFSR. This study conducted an updated literature review and discussed possible management of HFS/HFSR.
Methods
In total, 7,023 articles published between January 2000 and March 2025 were identified through PubMed, the Cochrane Library, Medical Online, and Ichushi-Web searches. Only English language articles were included, and the selection was conducted by a single reviewer. The search strategy focused on clinical trials, using the following keywords: HFS, palmar-plantar erythrodysesthesia syndrome, HFSR, prevention, therapy, capecitabine, pegylated liposomal doxorubicin, doxorubicin, 5-fluorouracil, docetaxel, cytarabine, vemurafenib, dabrafenib, encorafenib, regorafenib, sorafenib, sunitinib, lenvatinib, cabozantinib, pazopanib, axitinib, and skin. After removing 2,470 duplicate records, 2,244 publications were excluded following the title and abstract screening, due to research topic irrelevance. A further 173 were excluded at full-text review, because they had no usable data. The literature screening process is summarized in Fig. 1. This review was narrative in nature, and study inclusion was determined primarily by relevance rather than strict methodological quality. The methodology and reporting of this review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. Quality assessment tools such as GRADE or the Cochrane risk-of-bias tool were not applied.Fig. 1. Diagram of study selection/screening process
Results
Of the 53 included studies, data from 37 articles on the incidence of HFS and HFSR were extracted, and are summarized in Table 1. Table 1. Incidence of HFS/HFSR according to cytotoxic agents in Asian patientsCytotoxic agentsIncidence (%)CTx inducing HFS Capecitabine73.4– ≥ 90% [18–20] Pegylated liposomal doxorubicin15–78.4% [21–23] Doxorubicin22–26%, data are unavailable specifically for Asia [24] 5-fluorouracil14–31% [25–27] Docetaxel6–41.2% [28, 29] Cytarabine14–33%, data are unavailable specifically for Asia [24]BRAF inhibitors inducing HFS Vemurafenib10–47.8% [33, 34] Dabrafenib42% [35], data are unavailable specifically for Asia Encorafenib5.1–27.3% [36, 37]MKIs inducing HFSR Regorafenib47–73% [38–40] Sorafenib4.5%–45% [41, 42] Sunitinib43–57.8% [43, 44] Lenvatinib27–40.5% [45, 46] Cabozantinib35.3–71.4% [47–50] Pazopanib3–14.8% [51, 52] Axitinib14.4–75% [53–57]HFS, hand–foot syndrome; CTx, cytotoxic agent; HFSR, hand–foot skin reaction; MKIs, multi-kinase inhibitors
Incidence of HFS according to cytotoxic agents
As Table 1 shows, CTx, that are capable of inducing HFS include capecitabine (73.4– ≥ 90% [18–20]), pegylated liposomal doxorubicin (15–78.4% [21–23]), doxorubicin (22–26%, data are unavailable specifically for Asia [24]), 5-fluorouracil (5-FU) (14–31% [25–27]), docetaxel (6–41.2% [28, 29]), and cytarabine (14–33%, data are unavailable specifically for Asia [24]). The incidence of grade ≥ 2 HFS (drug withdrawal should be considered) was reported to be up to 40% [18, 23, 30–32]. With regard to BRAF inhibitors, vemurafenib (10–47.8% [33, 34]), dabrafenib (42% [35], data are unavailable specifically for Asia), and encorafenib (5.1–27.3% [36, 37]) induce HFS.
Incidence of HFSR according to cytotoxic agents
Also in Table 1, MKIs, including regorafenib (47–73%[38–40]), sorafenib (4.5%–45% [41, 42]), sunitinib (43–57.8% [43, 44]), lenvatinib (27–40.5% [45, 46]), cabozantinib (35.3–71.4% [47–50]), pazopanib (3–14.8% [51, 52]), and axitinib (14.4–75% [53–57]) induced HFSR.
Randomized controlled trials (RCTs) of prophylaxis for HFS
Of the 53 included studies, data from 11 articles on RCTs of prophylaxis for preventing HFS/HFSR were extracted and are summarized in Table 2. Table 2. Randomized controlled trials of prophylaxis for HFSCountry, yearProphylaxisBlindingPopulation (N)ChemotherapyInterventionComparatorOutcomesChina 2010 [30]CelecoxibNoN = 101Stage II–III colorectal cancerCapecitabine-basedN = 51Celecoxib 200 mg BID daily with capecitabine-based chemotherapy (monotherapy or CAPOX)N = 50Without celecoxibCelecoxib reduced the incidence of grade > 2 HFS (11.76% vs. 30% P = 0.024)China 2012 [18]CelecoxibNoN = 150Stages II–III colorectal cancerCapecitabine-basedN = 68Celecoxib 200 mg BID daily with capecitabine-based chemotherapy (monotherapy or CAPOX)N = 71Without celecoxibCelecoxib reduced the incidence of grade 2 HFS (14.7% vs. 29.6% P = 0.035)Iran 2023 [64]Celecoxib topical hydrogelNoSelf-controlledN = 285-fluorouracil, capecitabine, docetaxel, and paclitaxelN = 28one-half to 1 teaspoon of the celecoxib hydrogel BID–No significant difference in all grade (P = 0.38)South Korea 2010 [88]PyridoxineYesN = 389Gastrointestinal tract cancersCapecitabineN = 180Pyridoxine 100 mg BIDN = 180PlaceboNo significant difference in all grade HFS (64% vs. 76.1% P = 0.13) in first three chemotherapyJapan 2014 [89]PyridoxineNoN = 60 Colorectal cancerCapecitabineN = 30Pyridoxine 60 mg/dayWithout pyridoxineNo significant difference in grade ≥ 2 HFS (60.0% vs. 60.0% P = 1.00)Singapore 2017 [90]PyridoxineYesN = 210 Breast and colorectal cancersCapecitabineN = 105Pyridoxine 200 mg/dayN = 105PlaceboNo significant difference in grade ≥ 2 HFS (31.4% vs. 37.1% P = 0.38)Japan 2018 [91]PyridoxineNoN = 133 Advanced or metastaticbreast cancerCapecitabineN = 66Pyridoxine 60 mg/dayN = 67Without pyridoxineNo significant difference in grade ≥ 2 HFS (28.8% vs. 31.3% P = 0.75)Japan 2020 [31]PyridoxineEppikajutsuto (Kampo medicine)NoN = 22 Colorectal cancerCapecitabine-basedN = 10Pyridoxine 20 mg TIDN = 12Eppikajutsuto (Kampo medicine)2500 mgNo significant difference in grade ≥ 2 HFS (40.0% in pyridoxine group, 50.0% in Eppikajutsuto group P = 0.22)China 2021 [58]Lithium contained topical and moisturizingYesN = 122Stages II-III colorectal cancerCapecitabineN = 51EVOSKIN® Palm and Solemoisturizing creamBIDN = 54Physiological saline BIDEVOSKIN® Palm and Solemoisturizing cream reduced the incidence of grade ≥ 1 and grade ≥ 3 HFS (56.8% vs. 75.9% P = 0.006, 6.0% vs. 18.5% P = 0.001, respectively)India 2024 [65]Diclofenac gelYesN = 311Breast and gastrointestinal cancerCapecitabineN = 130Diclofenac 1% gelup to four times per dayN = 133Placebo gelDiclofenac gel reduced the incidence of grade ≥ 2 HFS (3.8% vs 15.0% P = 0.003)India 2020 [32]Structured Teaching ModuleYesN = 280Colorectal cancerCapecitabine -basedN = 135Continuous structured teaching module by oncology nurseN = 134Routine clinical educationNo significant difference was found in the incidence of grade ≥ 2 HFS (33.3% vs. 32.8% P = 0.93)HFS, hand–foot syndrome; CAPOX, capecitabine combined with oxaliplatin; N.D., not detected
Clinical studies on the prevention of HFS
Moisturization
Only one RCT was found on HFS prevention by moisturization [58]. No other RCT examined the effects of moisturization alone.
Pyridoxine
Most RCTs on pyridoxine showed negative results, and multiple systematic reviews and meta-analyses have shown insufficient efficacy [59, 60].
Celecoxib
Two RCTs in China demonstrated preventive efficacy against HFS [18, 30]. However, an RCT in UK showed negative result [61]. Celecoxib is associated with a high risk of cardiovascular side effects [62, 63], gastrointestinal ulceration, and/or perforation, which may worsen with long-term prophylaxis. Efficacy of topical celecoxib hydrogels has not been demonstrated the efficacy in a self-controlled randomized study [64].
Topical diclofenac
The Diclofenac-topical for Reduction of capecitabine-related HFS (D-TORCH) study [65] suggested a preventive effect of diclofenac gel against capecitabine-induced HFS. However, in the D-TORCH study, the diclofenac gel was administered exclusively on the palms. Additionally, gels can induce skin dryness, leading to HFS and itchiness. Phase 3 RCTs evaluating the preventive effects of diclofenac cream on the palms and soles are ongoing in Japan [66].
Topical steroid
A phase 2 study evaluated hydrocortisone and reported its efficacy in capecitabine-induced HFS [67, 68]. However, no clinical recommendations exist regarding its prophylactic use as current evidence is insufficient to support the preventive effect of topical steroids on HFS. Regarding the recommended therapy, expert opinion suggests the use of high-potency topical steroids for patients with grade ≥2 HFS (Common Terminology Criteria for Adverse Events [CTCAE] v5.0) [69].
Topical antibiotics
Prophylactic evidence supporting the use of topical antibiotics, which are otherwise effective in treating symptoms associated with infections, is lacking. They may be considered for treating infections associated with HFS.
Cooling
Efficacy of cooling against HFS induced by pegylated liposomal doxorubicin has been demonstrated [70–72], but no designed trials exist. Oxaliplatin-induced peripheral neuropathy is exacerbated when cooling is performed in patients indicated for CAPOX therapy. Besides patients receiving oxaliplatin, cooling may be considered for preventing HFS.
Teaching program
Case–control and retrospective studies have revealed efficacy of teaching programs [73, 74]; however, RCT finding was negative [32].
Hydrocolloid dressing
Only one trial has been designed [75] and a phase 3 randomized self-controlled study is ongoing [76].
RCTs of prophylaxis for HFSR
Of the 53 included studies, data from five articles reporting RCT findings on prophylaxis for preventing HFSR were extracted and are summarized in Table 3. Table 3. Randomized controlled trials of prophylaxis for HFSRCountry, yearProphylaxisBlindingPopulation (N)ChemotherapyInterventionComparatorOutcomesChina 2020 [81]CelecoxibNoN = 116Advanced HCCSorafenibN = 58Celecoxib 200 mg BIDN = 58Without celecoxibCelecoxib reduced the incidence of grade ≥ 2 and grade 3 HFSR (29.3% vs. 63.8% P < 0.001, 3.4% vs. 19.0% P = 0.008, respectively)China 2015 [78]Urea creamNoN = 871Advanced HCCSorafenibN = 43910% urea cream TID + BSCN = 432BSC10% urea cream T + BSC reduced the incidence of grade ≥ 2 HFSR (20.7% vs. 29.2% P = 0.004)South Korea 2020 [79]Urea creamYesN = 288Advanced HCCSorafenibN = 13020% urea cream TIDN = 117PlaceboNo significant difference in grade ≥ 2 HFSR (50.8% vs. 59.8% P = 0.153)Taiwan 2022 [80]Urea creamYesN = 129Advanced HCCSorafenibN = 4210% urea cream + BSCN = 42BSCN = 41Moisturizing cream + BSCNo significant difference was found in the incidence density of HFSR in each groups (P > 0.05)Japan 2013 [75]Hydrocolloid dressingNoN = 33Advanced renal cell carcinomaSorafenibN = 14Hydrocolloid dressing containing ceramide with a low-friction external surface every 2–3 daysN = 1610% urea creamHydrocolloid dressing reduced the incidence of grade ≥ 2 HFSR (29% vs. 69% P = 0.03) on the soles of the feetHFSR, hand–foot skin reaction; HCC, hepatocellular carcinoma; BSC, best supportive care; N.D., not detected
Clinical studies for the prevention of HFSR
Moisturization
No study that has evaluated the preventive effect of moisturization for HFSR has been reported. However, poor adherence to moisturizer use affects the therapeutic efficacy of regorafenib [77].
Urea cream
Urea cream use has been evaluated for its prophylactic efficacy in sorafenib-related HFSR [78–80]. Topical urea is effective against keratinized skin because it improves skin keratinization. However, its effectiveness shows mixed results. Urea cream can also induce skin irritation. While exercising caution regarding skin irritation, urea cream should be considered for the prevention of HFSR.
Celecoxib
One RCT in China demonstrated preventive efficacy against HFSR [81]. However, an RCT in UK showed negative results [61]. Celecoxib is associated with a high risk of cardiovascular side effects [62, 63], gastrointestinal ulceration, and/or perforation, which may worsen with long-term prophylaxis.
Topical steroid
Prophylactic effect of clobetasol on regorafenib-induced HFSR was previously reported [82]. However, no clinical recommendations exist regarding its prophylactic use as current evidence is insufficient to support its preventive effect on HFSR. Regarding the recommended therapy, expert opinion suggests the use of high-potency topical steroids for patients with grade ≥1 HFSR (CTCAE v5.0) [69].
Topical antibiotics
Prophylactic evidence supporting the use of topical antibiotics, which are otherwise effective in treating symptoms associated with infections, is lacking. They may be considered for treating infections associated with HFSR.
Hydrocolloid dressing
Only one trial has been designed [75] and a phase 3 randomized self-controlled study is ongoing [76].
Therapeutic medication
To date, no clinical trial has evaluated the therapeutic effects of medications for managing HFS/HFSR. However, various guidelines recommend topical steroids for inflammation and pain, 10% urea cream for exfoliation, and topical antibiotics [13, 14]. These medications are essential for controlling symptoms in clinical practice. Therapeutic strategies should be considered following previous guidelines and recommendations.
Discussion
Possible management of HFS and/or HFSR.
HFS induced by CTx and BRAF inhibitors
High-level evidence exists for preventing capecitabine-related HFS using oral celecoxib and diclofenac. Oral celecoxib is associated with a high risk of cardiovascular side effects [62, 63], gastrointestinal ulceration, and/or perforation, which may worsen with long-term prophylactic use. Considering its safety, oral celecoxib has limitations as a preventive strategy. Limited prophylactic administration duration should be considered, and caution for adverse events. In contrast, topical diclofenac is relatively safe, and high-level evidence from the only large blinded RCT showed positive result [65]. However, in an RCT evaluating the preventive effect of diclofenac on capecitabine-related HFS (D-TORCH study) [65], HFS incidence in the placebo group was notably lower than for other Asian countries (Table 4). Differences in the frequency of all grades of HFS (> 30%) should be noted. Furthermore, diclofenac gel was administered only to the palms in the D-TORCH study, and its preventive effect on the soles remains unclear. To allay concerns about data reproducibility and effectiveness on soles, a phase 3 RCT evaluating the preventive effects of diclofenac cream on palms and soles is ongoing in Japan [83]. Regarding the prophylactic use of topical steroids, a subset analysis [84] showed no prophylactic efficacy in sorafenib-induced HFSR. However, results of a phase 2 trial currently investigating the prophylactic efficacy of topical hydrocortisone in capecitabine-induced HFS in Japan [67] are awaited. Stress avoidance and moisturization may be recommended because of their safety; however, no RCTs have evaluated their preventive effects. Instead, lithium-containing topical and moisturizing agents showed preventive effects against HFS in a well-designed study [58] although this study showed no preventive effect of moisturizers only; however, the study agent reduced incidence of grade ≥ 1 HFS. Regarding urea cream, preventive effect against grade ≥ 2 HFSR was shown [78]. Although urea cream irritates the skin in unfit patients, it can be therapeutically effective against HFSR, which is prone to keratinization. For grade ≥ 2 HFS/HFSR, topical steroid is essential to control skin discomfort and inflammation [13]. Since evidence is lacking, the therapeutic use of topical steroids should be limited at this stage. Various guidelines recommend high potent topical steroid therapy for grade ≥ 2 HFS/HFSR [13, 14], and such is used in clinical practice, although no RCTs have been conducted. If local infections are suspected, topical antibiotics are needed although their efficacy has not been evaluated in RCTs. Regarding teaching programs and hydrocolloid dressings, no recommendations exist introducing them clinically at this stage, and future trials are awaited. Table 4. Randomized controlled trials showing differences in the incidence of HFS induced by capecitabine in India (D-TORCH study) and other Asian countriesIncidence rate of HFS (any grade)Incidence rate of HFS (grade 2 or 3)Incidence rate of HFS (≥ grade 3)Number of patients%%%CountryInterventionControlInterventionControlInterventionControlInterventionControlChina 2010 [30]5150295211.76301.9610China 2012 [18]687157.474.614.729.62.98.5South Korea 2010 [88]1801806476.11215.43.35Singapore 2017 [90]1051056166323742Japan 2018 [91]66677769343444Japan 2020 [31]10127083.34050208.3China 2021 [58]515456.875.94.816.76.016.7India 2020 [32]13513464.462.533.332.85.26.8India 2024 [65]1301336.118.13.8152.35.3HFS, hand–foot syndrome
Table 5 summarizes possible management approaches. Managing HFS induced by CTx and BRAF inhibitors should be symptom grading-based according to CTCAE. Preventive measures (grade 0) include avoiding mechanical or chemical stress, limiting water exposure, wearing appropriately fitted gloves, regular use of emollients, and patient education. Topical diclofenac or short-term oral celecoxib may also be considered. For grade 1 (mild) HFS, observation, continuing same dose chemotherapy, moisturizing, and using keratolytic agents, such as 10% urea cream, are recommended. Grade 2 (moderate) HFS, which limits instrumental activities of daily living (IADL), requires very strong topical corticosteroids (to step-down following improvement), possible chemotherapy dose modification or postponement, and dermatology referral. For grade 3 (severe) HFS, which interferes with self-care, strongest corticosteroids are indicated, with chemotherapy interruption or dose reduction, topical antibiotics if infection is suspected, and mandatory dermatology consultation. Continuous patient education is emphasized across all grades. Table 5. Management of HFS induced by CTx and BRAF inhibitorsGrading of CTCAEManagementFollow upGrade 0 preventionAvoid stressmechanical and chemical stress (excessive exercise and external damage) should be avoidedExcessive exposure to water should be avoided and gloves are recommendedGloves that are tight in size are not recommendedMoisturizingApply evenly throughout the hands and feet. The fingertip should be consideredTopical diclofenacOral celecoxibLimited duration of administration, with caution for adverse eventsContinuous patient educationUntil development of HFSGrade 1 treatmentMinimal skin changes or dermatitis (e.g., erythema, edema, or hyperkeratosis) without painObservation until the symptoms worsenSame dose of chemotherapy should be consideredKeep moisturizing and avoid stress10% urea cream for exfoliationContinuous patient education2 weeksIf the symptom worsens, proceed to the next stepGrade 2 treatmentSkin changes (e.g., peeling, blisters, bleeding, fissures, edema, or hyperkeratosis) with pain; limiting instrumental ADLVery strong or strong class topical steroids. If symptom improves to grade 0 or 1, step down to medium class topical steroidPostponement until symptoms improve to grade 0 or 1 should be consideredDose reduction of chemotherapy should be consideredTopical antibiotics if infection is suspectedContinuous patient educationConsultation with dermatologist2 weeksIf the symptom worsens or does not improve, proceed to the next stepGrade 3 treatmentSevere skin changes (e.g., peeling, blisters, bleeding, fissures, edema, or hyperkeratosis) with pain; limiting self-care ADLTopical strongest class steroidsTreatment discontinuation or postponement until symptoms improve to grade 0 or 1 should be considered. If symptom improves to grade 0 or 1, step down to medium class topical steroidDose reduction of chemotherapy should be consideredTopical antibiotics if infection is suspectedContinuous patient educationConsultation with dermatologist2 weeksHFS, hand–foot syndrome; CTx, cytotoxic agent; CTCAE, Common Terminology Criteria for Adverse Events; ADL, activities of daily living
HFSR induced by MKIs
The only treatment with valid preventive effect evidence against HFSR is hydrocolloid dressings. Although a phase 3 randomized self-controlled study is ongoing [76], the evidence is currently insufficient. Therefore, future trials are warranted. Regarding HFSR treatment, topical steroids and antibiotics may be recommended, similar to CTx-related HFS. However, evidence-based recommendations cannot be made.
Table 6 summarizes possible management approaches. Management of HFSR induced by MKIs should be guided by CTCAE grading. Preventive measures (grade 0) require avoiding mechanical and chemical stress, limiting water exposure, use of appropriately fitted gloves, regular skin care, and continuous patient education. For grade 1 (mild) HFSR, same dose MKI treatment may be maintained. Supportive care includes moisturization, using 10% urea cream, and very strong or strong topical corticosteroids (to step-down to medium potency once improved). Grade 2 (moderate) HFSR, which restricts IADL, requires the strongest topical corticosteroids, potential treatment delay or dose reduction until improvement, and use of topical antibiotics if infection is suspected. Dermatology consultation is recommended, and step-down therapy should be applied once symptoms improve. For grade 3, (severe) HFSR, which interferes with self-care activities, necessitates the strongest class topical corticosteroids, chemotherapy interruption or discontinuation, and MKI dose reduction. Adjunctive measures include topical antibiotics for suspected infection, dermatology referral, and continuing patient education. Overall, patient education and proactive symptom management are emphasized across all grades to optimize adherence to MKI therapy. Table 6. Management of HFSR induced by MKIGrading of CTCAEManagementFollow upGrade 0 preventionAvoid stressmechanical and chemical stress (excessive exercise and external damage) should be avoidedExcessive exposure to water should be avoided and gloves are recommendedGloves that are tight in size are not recommendedMoisturizingSkin care focusing on pressure sensitive areasOral celecoxibLimited duration of administration, with caution for adverse events10% urea creamContinuous patient educationUntil development of HFSGrade 1 treatmentMinimal skin changes or dermatitis (e.g., erythema, edema, or hyperkeratosis) without painSame dose of chemotherapy should be consideredKeep moisturizing and avoid stress10% urea cream for exfoliationTopical very strong class or strong class steroids. If symptom is improved to grade 0, step down to medium class topical steroidContinuous patient education2 weeksIf the symptom worsens, proceed to the next stepGrade 2 treatmentSkin changes (e.g., peeling, blisters, bleeding, fissures, edema, or hyperkeratosis) with pain; limiting instrumental ADLStrongest class topical steroidsIf symptom improves to grade 0 or 1, step down to medium class topical steroidTreatment postponement until symptoms improve to grade 0 or 1 should be consideredDose reduction until symptoms improve to grade 0 or 1 may be consideredTopical antibiotics in case infection is suspectedContinuous patient educationConsultation with dermatologist2 weeksIf the symptom worsens or does not improve, proceed to the next stepGrade 3 treatmentSevere skin changes (e.g., peeling, blisters, bleeding, fissures, edema, or hyperkeratosis) with pain; limiting self-care ADLStrongest class topical steroidsIf symptom improves to grade 0 or 1, step down to medium class topical steroidTreatment discontinuation or postponement until symptoms improve to grade 0 or 1 should be consideredDose reduction of MKI should be consideredTopical antibiotics in case infection is suspectedContinuous patient educationConsultation with dermatologist2 weeksHFSR, hand–foot skin reaction; MKI, multi-kinase inhibitors; CTCAE, Common Terminology Criteria for Adverse Events; HFS, hand–foot syndrome; ADL, activities of daily living
Differences between Asia and other countries’ recommendations
No Asia-specific management guidelines for HFS/HFSR exist. High-potency steroid therapy is recommended for grades 1 and 2 HFS/HFSR in the United States and Europe [13]. However, topical steroids are not recommended for grade 1 HFS in Asian patients. While lidocaine patches and antiseptic solutions (e.g., 1% silver sulfadiazine) are recommended for grade ≥ 3 HFS in the West, evidence and safety data are lacking in Asia; thus, they are not being administered in clinics.
Differences between Asian and other race skin types should be considered. Asian skin has a thin stratum corneum (outermost layer) and dense cells, which are sensitive and may overreact when irritated [85, 86]. In contrast, Asian skin contains more melanin than Western skin, providing natural protection against ultraviolet radiation [87]. However, Westerners with lower melanin content are more prone to hyperpigmentation and may be more prone to 5-flurouracil-induced and steroid-induced hyperpigmentation. Management approaches should differ according to race and skin type.
Future research questions
In future, the prophylactic efficacy of diclofenac against capecitabine-induced HFS should be evaluated using a cream formulation as the base agent. Further evidence on the prophylactic efficacy of hydrocolloid dressing against MKI-induced HFSR is anticipated. A trial examining the efficacy of educational programs and multidisciplinary team approach should be conducted.
Limitations
This review has some limitations. This is not a systematic review, and quality assessment tools such as GRADE or the Cochrane risk-of-bias tool were not applied. In future, it is desirable to establish guidelines based on systematic review findings for patients in Asia, involving ore rigorous protocols. Despite its important region-specific recommendations, some of the suggested approaches, including the use of topical antibiotics, stress avoidance, and moisturizers, lack sufficient evidence to draw robust conclusions. Furthermore, the absence of ongoing trial results, including studies on diclofenac cream and topical steroids, limits our ability to make definitive recommendations. Additionally, there is a critical need for RCTs evaluating the effectiveness of educational programs and multidisciplinary team approaches in managing HFS and HFS/HFSR.
Further research based on differences in skin characteristics between Asian and Western populations is essential to develop treatment strategies that are both regionally appropriate and globally applicable. By addressing these gaps, future studies could contribute to improved patient outcomes and a more effective management of debilitating conditions.
Conclusions
In this review, differences in skin biology between Asian and Western populations suggest the need for skin type-specific approaches to managing HFS/HFSR. No Asia-specific management guidelines for HFS/HFSR exist. High-potency steroid therapy is recommended for grade 1 and 2 HFS/HFSR in the United States and Europe. However, topical steroids are not recommended for HFS in Asian patients because of their different skin type. In addition, some medications, such as lidocaine patches or antiseptic solutions, used for grade ≥ 3, are not recommended for patients in Asia. In addition, diclofenac topical agents are expected to have a preventive effect on capecitabine-induced HFS. Recommendations considering the characteristics of Asian skin should be applied in clinical practice.
This review provides evidence-based recommendations from studies conducted on Asian patients, focusing on the prevention and treatment of HFS/HFSR. By addressing the unique skin characteristics of Asian populations, this review highlights the potential benefits of specific strategies such as the use of topical diclofenac and moisturizers. It also emphasizes the need for tailored approaches because differences between Asian and Western skin types necessitate Asian-specific management strategies that cannot be transferred directly from Western guidelines.