Characterization of the mutational landscapes in Japanese patients with early-onset colorectal cancer from comprehensive genomic profiling data
Yutaka Okagawa, Tomohiro Kubo, Shin Ariga, Norito Suzuki, Hiroki Tanabe, Susumu Sogabe, Atsushi Ishiguro, Tatsuru Ikeda, Shinya Minami, Masahiro Hirakawa, Ichiro Kinoshita, Kohichi Takada

TL;DR
This study compares genomic differences in early-onset and late-onset colorectal cancer in Japanese patients, finding specific mutations more common in younger patients.
Contribution
Identifies distinct genomic alterations in early-onset CRC, suggesting potential therapeutic targets in Japanese patients.
Findings
EoCRC patients had higher frequencies of SMAD4, FLT3, and CDK8 alterations compared to LoCRC patients.
Cell cycle pathway alterations were significantly enriched in the EoCRC group.
SMAD4 mutations were associated with poor prognosis in both EoCRC and LoCRC groups.
Abstract
The incidence of early-onset colorectal cancer (EoCRC), defined as a CRC diagnosed in individuals younger than 50 years, has been increasing globally. The clinicopathological differences between EoCRC and late-onset CRC (LoCRC: diagnosed in individuals older than 50 years) are suggestive of distinct genomic landscapes. The aim of this study was to assess the differences in genomic alterations in Japanese patients with EoCRC and LoCRC from multiple institutions across Hokkaido using comprehensive genomic profiling data. The patient’s background, CRC location, pathological findings, clinical stage at presentation, prognosis, and genomic alterations of the EoCRC and LoCRC groups were compared. A total of 317 CRC patients were analyzed, including 61 with EoCRC and 256 with LoCRC. Right-sided CRC and differentiated histology were significantly less common in the EoCRC group. There was no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
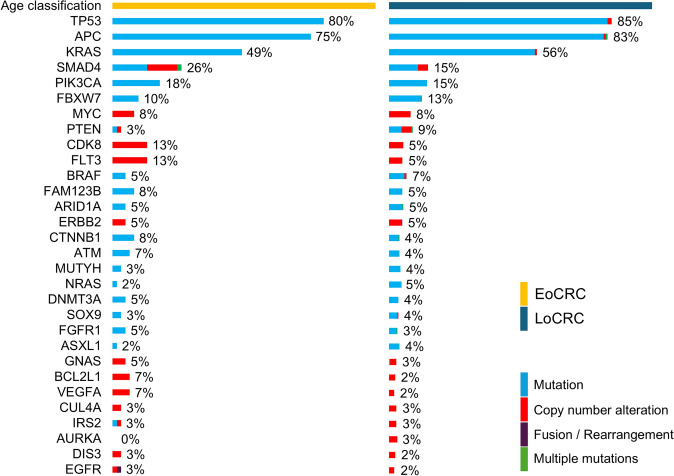 Figure 1
Figure 1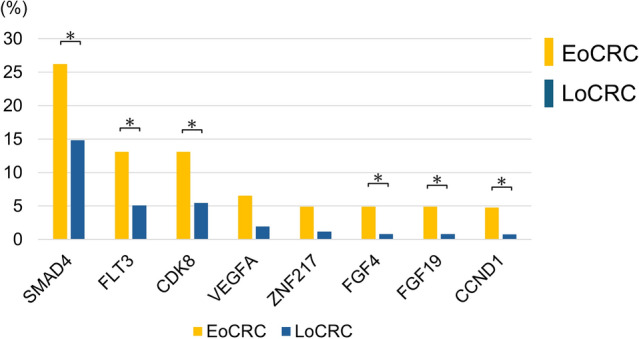 Figure 2
Figure 2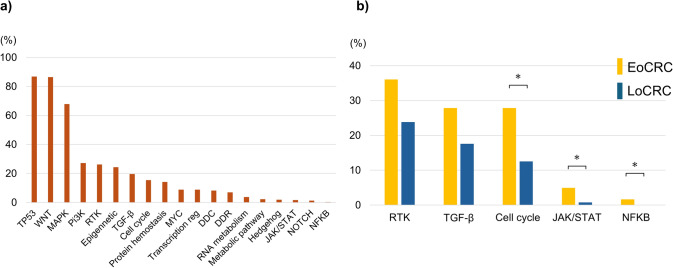 Figure 3
Figure 3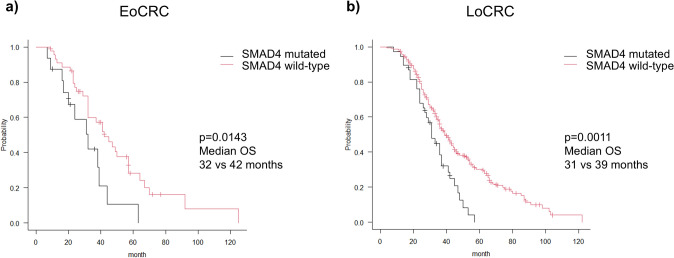 Figure 4
Figure 4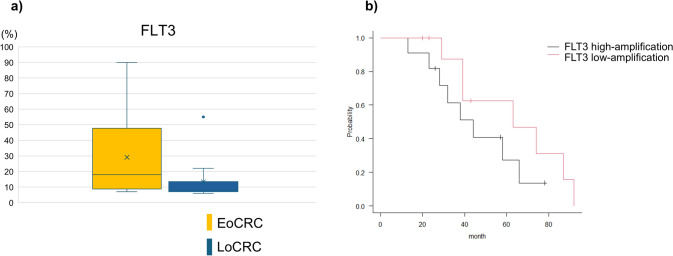 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic factors in colorectal cancer · Colorectal Cancer Treatments and Studies · Colorectal Cancer Screening and Detection
Introduction
The incidence of early-onset colorectal cancer (EoCRC), defined as a CRC diagnosed before the age of 50, has risen globally in recent years [1–3]. Various risk factors have been implicated in the development of EoCRC, such as increased consumption of Western diet, changes in the gut microbiome, alcohol consumption, obesity, genetics, and racial disparities [3–8]. However, the precise mechanisms underlying the pathogenesis of EoCRC remain unclear. EoCRC is often occurs in individuals without a family history of CRC. It frequently arises in the rectum, and is characterized by a higher proportion of poorly differentiated histology, including signet-ring cell carcinoma and mucinous carcinoma [9–12]. Moreover, EoCRC is more likely to be diagnosed at an advanced stage compared to late-onset CRC (LoCRC), which afflicts those aged 50 years or older [10]. While the prognosis for EoCRC is similar to that of LoCRC [13], the increasing incidence of EoCRC is a global public health concern given the profound social and personal impact of cancer diagnosis at a relatively young age. Limited studies have been conducted on EoCRC patients in Japan [14, 15], even though the age-standardized prevalence rate of EoCRC has been rising in the Japanese population [16], and this trend is expected to continue.
A key molecular driver of cancer is the accumulation of genomic and epigenomic alterations. The distinct clinicopathological features of EoCRC and LoCRC suggest differences in genomic alterations as well. Comprehensive cancer genomic profiling (CGP) has enabled systemic identification of genomic alterations in cancer patients, and several studies have assessed the genomic alterations between EoCRC and LoCRC using this approach [17, 18]. Li et al. [17] analyzed the CGP results of CRC patients in China, and identified significantly more genomic alterations in EoCRC, including those in PTCH1, KMT2A, and B2M, compared to LoCRC. Busico et al. [18] analyzed the CGP data of an Italian CRC cohort, and found that RNF43 gene mutations were more prevalent in the pediatrics patients, while the frequency of APC mutations increased with age. Recent studies have also highlighted racial differences in the genomic landscape of various cancers [19].
The aim of this study was to identify the differences in genomic alterations between Japanese EoCRC and LoCRC patients on the basis of CGP data, and provide insights that will contribute to the development of optimal therapeutic strategies for EoCRC patients.
Patients and methods
Study design and patients
The CGP data of advanced CRC patients from multiple centers across Hokkaido, Japan was retrospectively analyzed. Japanese CRC patients who underwent CGP with FoundationOne^®^ CDx genome profiling (F1CDx; Chugai Pharmaceutical, Tokyo, Japan), FoundationOne^®^ Liquid CDx genome profiling (F1LCDx; Chugai Pharmaceutical), OncoGuide™ NCC Oncopanel System (NCC Oncopanel; Sysmex Corporation, Kobe, Japan), Guardant360^®^ CDx (Guardant; Guardant Health Japan Corp, Tokyo, Japan), and GenMineTOP^®^ Cancer Genome Profiling System (GenMineTOP; Konicaminolta, Tokyo, Japan) between June 2019 and October 2024 were consecutively enrolled. The inclusion criterion was a pathological diagnosis of CRC, including patients with unresectable stage IV disease and patients with stage I–III or stage IV disease who developed postoperative recurrence. Patients with congenital anomalies, familial adenomatous polyposis, or inflammatory bowel diseases, or those who refused to provide written informed consent were excluded. The study was conducted as per the guidelines of World Medical Association Declaration of Helsinki, and written informed consent was obtained from all patients.
Genomic analysis
According to a previous report [20], genomic alterations were classified into seven tiers (A to F, and R) of evidence-level classifications. Actionable genomic alterations were defined as alterations at or above evidence level D as previously described [21]. Variants of unknown significance were excluded from the analysis in this study. Signaling pathways were classified according to the Japanese version of the Cancer Genomic Atlas [22].
Outcome measures
The patients were categorized into the EoCRC and LoCRC groups depending on the age at diagnosis. The patient’s background, CRC location, pathological findings, clinical stages at presentation, prognosis, and genomic alterations of the two groups were compared. A family history of CRC was defined as positive CRC diagnosis in a first-degree relative. Based on the predominant histopathological features, the CRC cases were classified as differentiated-type (well differentiated, moderately differentiated, and papillary adenocarcinoma) or undifferentiated-type (poorly differentiated, mucinous adenocarcinoma, and signet-ring cell carcinoma) based on the predominant histology. Clinical stages were classified according to the Union for International Cancer Control (UICC) TNM version 8. Prognosis was evaluated on the basis of overall survival (OS), which was calculated from the date of diagnosis of an unresectable cancer or recurrence until death.
Statistical analysis
All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R version 2.13.0 (R Foundation for Statistical Computing, Vienna, Austria) [23]. Quantitative variables were expressed as median, and categorical variables as absolute numbers and percentages. Pearson’s Chi-squared test and Mann–Whitney U-test were applied as appropriate. Survival rates were calculated using the Kaplan–Meier method and compared by the log-rank test. A p-value of < 0.05 was considered statistically significant.
Results
Patient characteristics and clinicopathological features
A total of 321 patients with CRC were initially enrolled, and four patients were excluded due to congenital anomalies (n = 1), familial adenomatous polyposis (n = 1), and inflammatory bowel diseases (n = 2). Among the remaining 317 patients, 61 (19.2%) were categorized into the EoCRC group and 256 (80.8%) into the LoCRC group (Table 1). The median age at CRC diagnosis was 45 years in the EoCRC group and 64 years in the LoCRC group. The gender distribution was similar in both groups. Similarly, there were no significant differences in the proportion of patients with a medical history of cancer excluding CRC or a family history of CRC (11.5% in the EoCRC group vs. 15.2% in the LoCRC group). Right-sided CRC was less common among the EoCRC patients compared to the LoCRC patients (8.2% vs. 26.2%, p = 0.003), and the proportion of patients with predominantly differentiated-type CRC was significantly lower in the EoCRC group than in the LoCRC group (83.6% vs. 92.6%, p = 0.029). On the other hand, the percentage of patients initially diagnosed with Stage IV disease was similar in both groups (55.7% in the EoCRC vs. 66.8% in the LoCRC group). There was also no significant difference between the two groups regarding the CGP testing methods or tumor sampling sites. The median survival duration was 41 months in the EoCRC group and 37 months in the LoCRC group, and the difference was not statistically significant (p = 0.978) (Supplementary Fig. 1). Table 1. Patient characteristics and clinicopathological featuresEoCRCLoCRCp valuen = 61n = 256Sex (M:F)30:31137:1190.542Past history of malignancy3250.231Family history of CRC7390.455Location Right-side5670.003 Left-side23770.250 Rectum331120.145Histology Differentiated512370.029 Undifferentiated10130.002 Others060.228Initial stage I140.966 II2140.483 III24670.041 IV341710.105Sampling sites Primary tumor321630.106 Metastatic lesions24710.076 Blood5220.921Comprehensive genomic profiling FoundationOne CDx511940.191 FoundationOne Liquid4180.896 OncoGuide NCC5310.387 Guardant360CDx140.966 GenMineTOP090.138CRC colorectal cancer, EoCRC early-onset colorectal cancer, LoCRC late-onset colorectal cancer
Analysis of genomic landscape
Four patients in this cohort had no detectable genomic alterations. The most frequently observed alterations were in tumor protein p53 (TP53: 83.9%), adenomatous polyposis coli (APC: 81.7%), and Kirsten rat sarcoma virus (KRAS: 54.9%). The genomic alterations in the EoCRC and LoCRC groups have been depicted in Fig. 1, and Fig. 2 shows the genes with relatively greater differences in alteration frequency between the two groups. Alterations in the mothers against decapentaplegic homolog 4 (SMAD4) (p = 0.016), FMS-like tyrosine kinase 3 (FLT3) (p = 0.023), and cyclin-dependent kinase 8 (CDK8) (p = 0.035) genes were more prevalent in the EoCRC group compared to the LoCRC group. In addition, fibroblast growth factor 4 (FGF4) (p = 0.02), FGF19 (p = 0.02), and cyclin D1 (CCND1) (p = 0.02) were also more frequently altered in the EoCRC group. Alterations in vascular endothelial growth factor A (VEGFA) (p = 0.052) and zinc finger protein 217 (ZNF217) (p = 0.053) also tended to be more common in the EoCRC group, albeit without statistical significance. Nevertheless, the mean number of actionable genomic alterations in the EoCRC and LoCRC groups were similar (5 vs. 6, p = 0.099). Microsatellite instability-high (MSI-high) was detected in two EoCRC patients (3.3%) and two LoCRC patients (0.8%). Furthermore, two patients (3.3%) in the EoCRC group and 15 patients (5.9%) in the LoCRC group showed high tumor mutation burden (TMB-high). The differences were not significant.Fig. 1. Genomic alterations in EoCRC and LoCRC patients. The top of 30 genomic alterations in the overall CRC cohort are shown, with the type of each alteration indicatedFig. 2Differences in genomic alterations between EoCRC and LoCRC groups. Comparison of the frequency of specific genomic alterations between EoCRC and LoCRC groups
Pathway alteration analysis
The TP53 (86.8%), WNT (86.4%), and MAPK (67.8%) pathways were the most commonly altered signaling pathways in the entire cohort (Fig. 3a). As shown in Fig. 3b, cell cycle pathway (27.9% vs. 12.5%, p = 0.003), JAK/STAT and NF-κB signaling pathway were more frequently altered in the EoCRC group compared to the LoCRC group. Although the receptor tyrosine kinase (RTK) and TGF-β signaling pathways were also more commonly altered in the EoCRC (RTK: 36.1%, TGF-β: 27.9%) group than in the LoCRC group (RTK: 23.8%, TGF-β: 17.6%), the difference was not significant.Fig. 3. Signaling pathway alterations in CRC. a Distribution of altered signaling pathways in the overall cohort. b Comparison of pathway alterations between EoCRC and LoCRC groups
SMAD4 and FLT3 alterations
We next analyzed the clinical and prognostic significance of SMAD4 and FLT3 alterations in the EoCRC and LoCRC groups. SMAD4 mutations were more frequently associated with colon tumors as opposed to rectal tumors in the EoCRC group, whereas no anatomical preference was observed in the LoCRC group (Table 2). Furthermore, SMAD4 mutation-positive patients exhibited significantly worse prognosis compared to patients lacking SMAD4 mutations in both groups (Fig. 4a, b). However, no significant difference was observed in the prognosis of EoCRC and LoCRC patients harboring SMAD4 mutations. Table 2. Comparison of clinicopathological features based on SMAD4 mutation statusEoCRCp-valueLoCRCp-valueSMAD4 mutatedSMAD4 wild-typeSMAD4 mutatedSMAD4 wild-typen = 16n = 45n = 38n = 218Sex Male10200.218211160.815Location Right-side140.74310570.983 Left-side10130.01813640.548 Rectum5280.03415970.566Histology Differentiated14370.627342030.430Initial stage IV8260.594241470.606EoCRC early-onset colorectal cancer, LoCRC late-onset colorectal cancerFig. 4Overall survival analysis of patients with SMAD4 mutations. a Overall survival of SMAD4 mutation-positive and -negative patients in the EoCRC group. b Overall survival of SMAD4 mutation-positive and -negative patients in the LoCRC group
Likewise, FLT3 amplification did not show any significant association with patient characteristics or prognosis in either group (Supplementary Table 1). Notably, co-amplification of CDK8 was identified in 75% of FLT3 amplification-positive EoCRC patients and in 84.6% of LoCRC patients, and this association was statistically significant (p < 0.01). Furthermore, a higher proportion of EoCRC patients harbored ≥ 10 copies of FLT3 compared to LoCRC patients (75% vs. 38.5%; Fig. 5a), although the difference was not significant (p = 0.086). Additionally, patients with higher copy number of FLT3 tended to have worse prognosis compared to those with fewer copies (median OS; 44 vs. 63 months), albeit without statistical significance (p = 0.206; Fig. 5b). Interestingly, a more pronounced difference was observed between the prognosis of FLT3-high and FLT3-low amplification subgroups among patients with FLT3 and CDK8 co-amplification; however, the difference did not reach statistical significance (Supplementary Fig. 2).Fig. 5FLT3 amplification analysis. a Distribution of FLT3 copy number alterations in EoCRC and LoCRC patients. b Overall survival of patients with high-amplification and low-amplification of FLT3
Discussion
This study is the first to evaluate the differences in genomic alterations between EoCRC and LoCRC in Japanese patients. Importantly, we found that genomic alterations such as FLT3 and CDK8, which have not been reported previously, were significantly more common in EoCRC. These findings suggest that Japanese EoCRC may harbor unique genomic features compared with Western and Chinese cohorts.
Alterations in PTCH1, KMT2A, and ZNF43, which have been previously reported in EoCRC [17, 18], were not detected in this cohort. In contrast, SMAD4, FLT3, and CDK8 were more frequently altered in EoCRC patients compared to the LoCRC patients. The discrepancies in genomic alterations observed in this study compared to previous reports are most likely due to ethnic background differences. In addition, the results may have been affected by variations in the detectable genes depending on the CGP testing platforms, as well as by differences in disease stage arising from patient selection criteria.
SMAD4 mutations have been detected in 5–24.2% of CRC cases [24], particularly in the advanced stages, and more often in the colon relative to the rectum. Furthermore, these mutations associated with poor prognosis [24]. A previous study reported higher frequency of SMAD4 alterations in younger CRC patients [25], which is consistent with our findings and suggests that SMAD4 mutations may play a role in the pathogenesis of EoCRC. In addition, EoCRC patients with SMAD4 alterations in our cohort demonstrated a significantly higher incidence of tumors in the colon -as opposed to the rectum- compared to the SMAD4 alteration-negative patients, which is consistent with previous reports. Additionally, the presence of SMAD4 alterations was significantly associated with poor prognosis. SMAD4 is a tumor suppressor gene and acts as a mediator of the TGF-β signaling pathway, and SMAD4 mutations contribute to tumor progression by disrupting cellular differentiation and proliferation. In fact, the TGF-β/SMAD4 signaling pathway has been implicated in CRC progression and warrants further investigation as a potential therapeutic target [26, 27]. Alterations in the TGF-β pathway were also more common in EoCRC patients, which corresponded to the higher incidence of SMAD4 alterations in this group. Although EoCRC overall is more frequently located in the rectum, SMAD4-mutated EoCRC cases were more commonly found in the colon. Various molecular and biological differences have been reported between colon and rectal cancers [28], and SMAD4 may play a more prominent role in the development of colon cancer in EoCRC, potentially through dysregulation of the TGF-β/SMAD4 signaling pathway. Further studies are needed to clarify the underlying mechanisms.
FLT3 encodes a receptor tyrosine kinase (RTK) that plays a key role in hematopoiesis, and is overexpressed in MLL-rearranged acute lymphoblastic leukemia [29]. While FLT3 amplification has been reported at low frequencies in CRC [30, 31], previous studies have suggested a potential inverse relationship between FLT3 copy number and patient prognosis [31]. In this study, FLT3 amplification was not significantly associated with prognosis, which may be attributed to the limited sample size. Furthermore, in line with previous findings, high- amplification of FLT3 showed a trend towards worse overall survival. Altogether, these findings raise the possibility that FLT3 may act as a potential oncogenic driver in CRC, thereby warranting further studies regarding its biological and therapeutic significance in EoCRC.
CDK8 encodes a cell cycle-related kinase, and is frequently overexpressed in various cancers and has been identified as a prognostic biomarker in CRC [32]. In this study, cell cycle alteration was more common in the EoCRC group, likely due to the higher frequency of CDK8 amplification. Notably, both FLT3 and CDK8 alterations were amplification events, and co-amplification was observed in the majority of FLT3-amplified cases. This can be attributed to their genomic proximity, as FLT3 and CDK8 are both located on chromosome 13q12. A previous case report has also highlighted the amplification of both FLT3 and CDK8 in CRC [33]. The effects of FLT3 and CDK8 inhibitors on CRC cells have been investigated [34, 35]. Further functional analyses and therapeutic evaluations are necessary to explore the clinical utility of these alterations in precision medicine strategies for EoCRC.
There were several limitations in this study that ought to be considered. First, there was selection bias because we only included patients with CGP data. As CGP testing is typically performed for unresectable or recurrent patients, mutations in non-advanced CRC could not be analyzed. Therefore, our cohort is not entirely representative of all CRC patients. In addition, this study included only Japanese patients, which limits the generalizability of the findings. Second, the sample size, especially that of the EoCRC group, was small, thereby warranting further studies with larger sample size for more accurate results. Third, the use of different CGP testing platforms, each characterized by distinct gene panels, detection sensitivities, and analytical algorithms, may have introduced variability in the results and limited the direct comparability of genomic findings. Furthermore, we were not able to ascertain whether the genomic alterations detected with high frequency in the EoCRC group, particularly FLT3 and CDK8 amplification, are oncogenic. Therefore, functional studies are needed in future to elucidate their biological roles.
In conclusion, this study demonstrated that SMAD4, FLT3, and CDK8 alterations are enriched in Japanese EoCRC patients, distinguishing them from previously reported Western and Chinese cohorts. Because these genes represent potentially actionable targets, our findings provide novel insights with important clinical implications.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (TIF 709 kb)Supplementary file2 (TIF 592 kb)Supplementary file3 (DOCX 15 kb)