Long-term effectiveness of the trabecular micro-bypass (iStent): 3-year real world data in glaucoma and ocular hypertension
Stafford Sansome, Ujjwal Banerjee, Benjamin Griffin, Sara Issa, Cristina Ginés-Gallego, Madalina Pavel, Mo Abu-Bakra, Sameer Trikha, Avi Kulkarni, Gerassimos Lascaratos, Obeda Kailani

TL;DR
A 3-year study shows that combining iStent inject® with cataract surgery significantly lowers eye pressure and reduces medication use in glaucoma patients.
Contribution
Provides real-world, long-term data on the effectiveness and safety of iStent inject® in diverse glaucoma patients over 3 years.
Findings
Mean intraocular pressure dropped by 19.1% three years after surgery.
24% of patients were medication-free at three years, up from 3% preoperatively.
67% of patients achieved qualified success with or without medication at three years.
Abstract
This study evaluates the effectiveness and safety profile of the iStent inject® combined with cataract surgery, with 3 years of follow-up in a large patient cohort (n = 464) of various glaucoma phenotypes and disease severity. This retrospective, single-arm, multi-surgeon study included eyes undergoing iStent inject® with cataract surgery. Inclusion criteria was symptomatic cataract in addition to uncontrolled intraocular pressure (IOP) on ≥ 2 IOP lowering agents or contraindication and/or intolerance to IOP lowering medication. IOP, medications, safety profile and cumulative success rates were assessed. The mean IOP was 14.8 ± 4.5 mmHg at 3 years, compared to 18.3 ± 5.8 mmHg preoperatively, an IOP reduction of 19.1% (P < 0.001). The mean number of IOP lowering medications was 1.84 ± 1.40 at 3 years, compared to 2.49 ± 1.12 medications preoperatively. At 3 years 24% of eyes were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
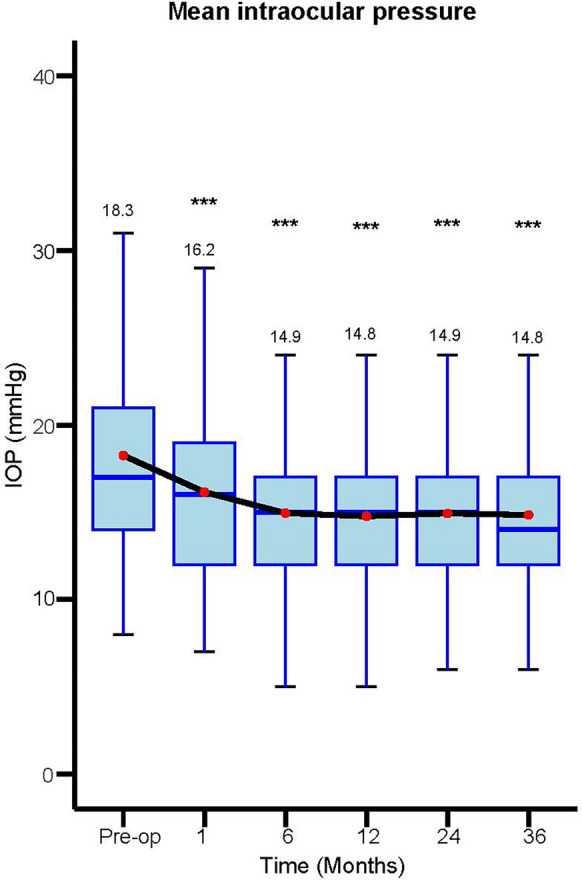 Figure 1
Figure 1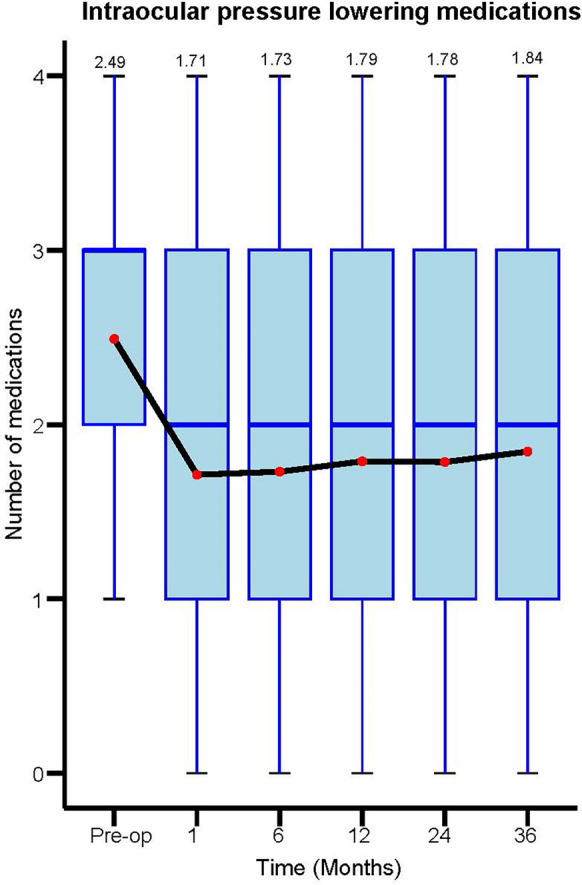 Figure 2
Figure 2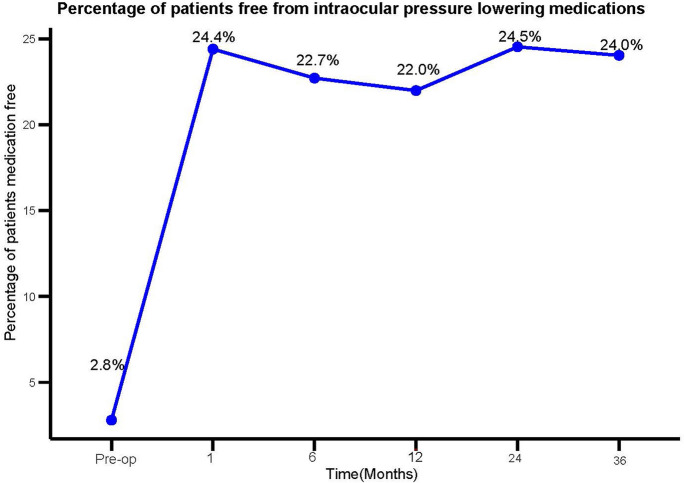 Figure 3
Figure 3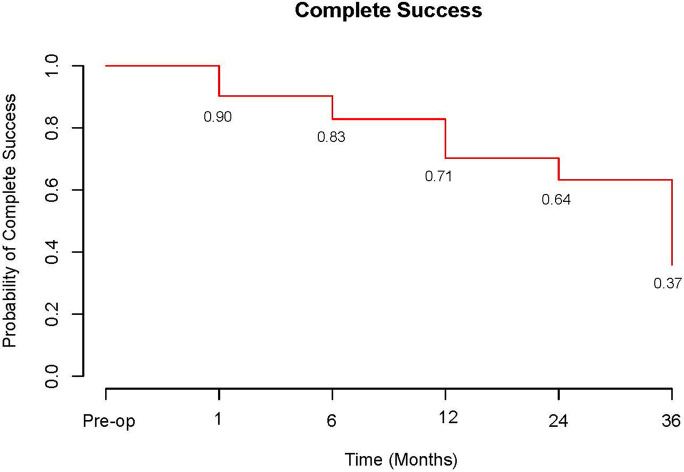 Figure 4
Figure 4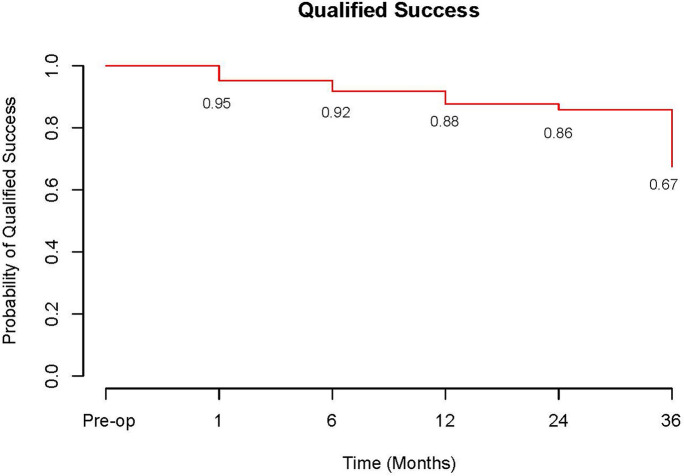 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Retinal Diseases and Treatments · Retinal and Macular Surgery
Introduction
The burden of glaucoma on the global population is well known, with primary open angle glaucoma (POAG) the leading cause of irreversible blindness worldwide [1]. As global life expectancy continues to increase, so does the prevalence of glaucoma and the need to optimise management of these patients to preserve vision throughout their lifetime [2]. Management of glaucoma is focussed on intraocular pressure (IOP) control with topical medications, laser treatment and filtration surgery the traditional measures used to lower IOP [3]. The advent of microinvasive glaucoma surgery (MIGS) has created another modality for the treatment of glaucoma patients [4]. Although more modest IOP reductions are typically achieved with MIGS procedures than filtration surgery, they have a significantly lower risk profile [4–11]. They can also be used as an alternative or adjunct to topical medication or employed before escalating to filtration surgery following a consideration of the risk–benefit profile for a given patient.
The iStent inject® (Glaukos, San Clemente, CA, USA) is a trabecular micro-bypass stent, the original version (iStent®) was the first MIGS device receiving approval for use in 2012 [12]. It can be used as a standalone device or combined with cataract surgery; two heparin coated titanium stents are injected directly through the trabecular meshwork under direct visualisation with a gonioscopy lens [12]. There have been numerous publications to date which have demonstrated the effectiveness of iStent inject® and iStent® in addition to favourable safety profiles in primary open angle glaucoma and ocular hypertension (OHT) [5–11, 13–19].
In this study, we provide data on the effectiveness and safety profile of iStent inject® combined with cataract surgery, with 3 years of postoperative follow-up in a large patient cohort.
Methods
Study design and participants
This was a retrospective, single-arm, multi-centre, multi-surgeon study of eyes that underwent iStent inject® implantation combined with phacoemulsification and intraocular lens (IOL) implantation, evaluating the clinical effectiveness and safety profile in various glaucoma phenotypes and OHT. Data was collected over a 6-year period across a single NHS Foundation Trust from surgery performed at 2 sites, between September 2017 and July 2023.
Inclusion criteria were symptomatic cataract in addition to uncontrolled IOP on ≥ 2 IOP lowering agents or contraindication and/or intolerance to IOP lowering medication. Uncontrolled IOP was defined by that above clinician set individual IOP targets according to disease severity. Patients required a diagnosis of a subtype of glaucoma, primary angle closure (PAC), OHT or be considered a glaucoma suspect (as defined by European Glaucoma Society Terminology and Guidelines for Glaucoma) [20]. Patients were excluded if they had undergone previous invasive glaucoma surgery (trabeculectomy, aqueous tube or shunt or any form of MIGS). Patients with uveitic, neovascular or traumatic glaucoma were excluded, due to abnormal angle morphology which precludes insertion of iStent inject® into the trabecular meshwork. Additional exclusion criteria included any patient undergoing an additional procedure at the time of cataract and iStent implantation such as endoscopic cyclophotocoagulation (ECP) or goniosynechialysis (GSL). Patients with less than 12-month postoperative follow-up data were also excluded. The observation period was ended for any patient undergoing filtration surgery or cyclodiode laser after cataract surgery with iStent; no further IOP or medication data was recorded after this time.
Surgical device and implantation technique
All iStents were performed by 5 different glaucoma consultants or their senior fellows via a temporal approach following phacoemulsification. The nasal angle was visualised using a direct gonioscopy lens and two iStents were inserted into the nasal trabecular meshwork approximately 2 clock hours apart. Postoperatively, IOP lowering medications were modified at the surgeon’s discretion following evaluation of pre-operative IOP and disease severity. Follow up was arranged between one and four weeks post-operatively.
Data analysis
Data was obtained from the hospital electronic patient records (Medisoft Ltd, Leeds, United Kingdom) and identifiable data were anonymised and categorised in Excel (Microsoft, Washington, USA) spreadsheets. The study was performed in line with the principles of the Declaration of Helsinki. Statistical analysis was done with base R statistics functionality using the “tidyverse” package [21]. Survival analysis was done using the “survival” package [22]. P-values were calculated using paired t-test with Bonferroni correction (due to different sample sizes). Results were considered statistically significant for p-values < 0.05. Complete and qualified success rates were determined by the proportion of eyes achieving ≥ 20% IOP reduction and an IOP of 6–21 mmHg after surgery without or with medication, respectively.
Results
Study population and baseline characteristics
A total of 464 eyes underwent iStent inject® combined with cataract surgery in this retrospective cohort, each with a minimum of 12 months follow up data. Preoperative demographics and ocular characteristics are displayed in Table 1. The mean age at the time of surgery was 77.5 ± 8.7 years with 54.1% of patients being female. Baseline IOP was 18.3 ± 5.8 mmHg with the mean number of IOP lowering medications at 2.49 ± 1.12. Preoperatively 3% of eyes were medication free. Baseline BCVA was 0.38 LogMAR and mean deviation (MD) of visual field − 7.68 ± 8.36 dB. The most common diagnosis was POAG (63%) followed by PACG (14%) and OHT (11%).Table 1. Baseline demographicsN = 464*Age (Years)Mean ± SD77.5 ± 8.7Range45–97Gender (%)*Female54.1%*Eye (%)OD48.1%Mean IOP at baseline (mmHg)Mean ± SD18.3 ± 5.895% CI17.7–18.8Range8–41BCVA at baseline (LogMAR)Mean0.3895% CI0.34–0.43Range− 0.20–2.00Number of IOP lowering agents at BaselineMean ± SD2.49 ± 1.1295% CI2.39–2.59Range0–4Mean deviation at baseline (dB)Mean ± SD− 7.68 ± 8.36Diagnosis (%)*Primary open angle glaucoma63.0%Primary angle closure glaucoma14.0%Ocular hypertension11.0%Glaucoma suspect3.5%Primary angle closure3.3%Normal tension glaucoma3.0%Pseudoexfoliative glaucoma1.3%Pigmentary glaucoma0.9%SD, Standard deviation; CI, Confidence interval; OD, Left eye; IOP, Intraocular pressure; mmHg, Millimetres of mercury; BCVA, Best corrected visual acuity; dB, Decibels
Intraocular pressure and medication use
There was a statistically significant reduction in IOP at all time points postoperatively (P < 0.001). The mean IOP was 14.8 ± 4.5 mmHg at 3 years follow up, compared to 18.3 ± 5.8 mmHg preoperatively, representing an IOP reduction of 19.1%. Figure 1 provides mean IOP data at various timepoints up to 3 years of follow up.Fig. 1. Mean intraocular pressure over time. Pre-op n = 464, 1 month n = 418, 6 months n = 460, 12 months n = 461, 24 months n = 461, 36 months n = 175. Abbreviations: *** = p value < 0.001, IOP = intraocular pressure
There was a statistically significant reduction in the number of IOP lowering medications at all time points postoperatively (P < 0.001). The mean number of IOP lowering medications was 1.84 ± 1.40 at 3 years follow up, compared to 2.49 ± 1.12 medications preoperatively, representing a mean reduction of 0.65 medications per eye. Figure 2 provides data on the mean number of IOP lowering medications at various timepoints up to 3 years of follow up. At 3 years 24% of eyes were medication free compared to 3% of eyes preoperatively (P < 0.001). The percentage of eyes that remained medication free was statistically significant at all time points of follow up which is outlined in Fig. 3.Fig. 2. Mean number of intraocular pressure (IOP) lowering medications over time. Pre-op n = 464, 1 month n = 455, 6 months n = 458, 12 months n = 464, 24 months n = 265, 36 months n = 129Fig. 3Percentage of patients free from intraocular pressure lowering medications over time. Pre-op n = 464, 1 month n = 455, 6 months n = 458, 12 months n = 464, 24 months n = 265, 36 months n = 129
Success rates
At 3 years follow up the cumulative probability of eyes achieving complete success; an IOP reduction of ≥ 20% and IOP 6–21 mmHg without medication was 37% (Fig. 4). Cumulative probability of achieving this with medication (qualified success) was 67% (Fig. 5). The probability of complete success was 71% at 1 year and 64% at 2 years compared to the probability of qualified success which was 88% at 1 year and 86% at 2 years.Fig. 4. Complete success over time. Defined as an intraocular pressure reduction of ≥ 20% and IOP 6–21 mmHg without medicationFig. 5Qualified success over time. Defined as an intraocular pressure reduction of ≥ 20% and IOP 6–21 mmHg with medication
Subgroup analysis
Subgroup analysis was also performed. Severity of glaucoma classified by early (MD > − 6D), moderate (MD − 6 to − 12 dB) and severe (MD < − 12 dB) showed no statistically significant difference between these groups with regards to IOP or medication reduction across the various timepoints.
Comparison of IOP and medication reduction between glaucoma (POAG/NTG) and glaucoma suspects and OHT subgroups was performed (with data up to 2 years given small dataset available for OHT and glaucoma suspect patients at 3 years follow up). The mean IOP reduction in glaucoma eyes was 15.9% at 2 years (14.8 ± 4.56 mmHg at 2 years vs 17.6 ± 5.22 mmHg preoperatively) with a mean IOP reduction in glaucoma suspect and OHT eyes of 15.7% at 2 years (15.6 ± 3.76 mmHg at 2 years vs 18.5 ± 5.17 mmHg preoperatively). There was a statistically significant difference in reduction of IOP lowering medications between glaucoma and glaucoma suspect and OHT eyes at 2 years (P < 0.05). The mean number of IOP lowering medications for glaucoma eyes were reduced by 23.4% (0.61 drops) at 2 years (2.00 ± 1.32 at 2 years vs 2.61 ± 1.12 preoperatively) with medications for glaucoma suspect and OHT eyes reduced by 34.5% (0.69 drops) at 2 years (1.31 ± 1.26 at 2 years vs 2.00 ± 1.13 preoperatively). At 2 years 18% of glaucoma eyes were medication free (2% preoperatively) compared to 39% of glaucoma suspect and OHT eyes that were medication free at 2 years (6% preoperatively) (p < 0.05).
Safety data
There was a statistically significant post-operative improvement in BCVA at all time points before 3 years. At 12 moths BCVA was 0.19 compared to 0.38 preoperatively. Vision loss equivalent to ≥ 2 lines on Snellen occurred in 0.9% of eyes (4/464). Intra-operative complications recorded were hyphaema 0.6% (3/464), iris trauma or prolapse 0.6% (3/464), vitreous loss 0.4% (2/464), endothelial damage 0.4% (2/464) and phacoemulsification wound burn 0.2% (1/464). Post-operative complications recorded were uveitis 3.7% (17/464), macular oedema 2.2% (10/464), corneal oedema 1.7% (8/464), hyphaema 0.9% (4/464), iris to wound 0.2% (1/464) and wound leak 0.2% (1/464). One eye required an anterior chamber washout due to a persistent hyphaema with a raised IOP. No cases of endophthalmitis or hypotony were recorded. There were no cases of corneal decompensation recorded at any time point. A total of 5% of eyes (28/464) required further glaucoma procedures. Preserflo MicroShunt was subsequently performed in 2.2% of eyes (10/464), Trabeculectomy in 1.3% of eyes (6/464), Selective Laser Trabeculoplasty (SLT) in 1.1% (5/464) and cyclodiode laser in 0.4% (2/464).
Discussion
In this retrospective, single-arm, multi-centre, multi-surgeon study we report the effectiveness and safety profile of the iStent inject® combined with cataract surgery in a large cohort with 3 years follow up data. These 464 eyes include various glaucoma subtypes and severity of glaucoma, along with a high pre-operative medication burden. A significant and sustained reduction in IOP along with a reduction in IOP lowering medication was demonstrated throughout the 3 years of post-operative follow up, with favourable safety data.
The baseline characteristics of this study’s population were heterogenous with regards to disease severity, baseline IOP and medication burden as well as the subtype of glaucoma. There was a relatively high baseline IOP (18.3 mmHg), high pre-operative medication burden (2.49 medications) and significant degree of baseline visual field loss (MD − 7.68 Db). Inclusion criteria were broad and there were few indications for exclusion, in contrast to many studies in the literature which have narrow and pre-defined inclusion criteria. Therefore, this provides clinically relevant data reflective of a diverse glaucoma population with significant disease burden which can help to inform patients and surgeons with regards to evaluating glaucoma treatment options.
Our cohort achieved a statistically significant reduction in IOP maintained at 3 years follow up with an average reduction of 19.1% (from a baseline of 18.3–14.8 mmHg at 3 years). This was in addition to a 0.65 reduction in use of IOP lowering medications per eye (1.84 at 3 years vs 2.49 at baseline). At 3 years 24% of eyes were medication free compared to 3% of eyes preoperatively, which represents a sevenfold increase from baseline. These outcomes align to those of a 3 year multicentre, retrospective study of 273 eyes by Clement et al. [10]. This included various glaucoma subtypes or OHT with eyes undergoing iStent inject® combined with cataract surgery. There was a mean IOP reduction in this cohort of 15.5% (from a baseline of 16.4–13.9 mmHg at 3 years) and a 1.03 reduction in use of IOP lowering medications per eye (0.48 at 3 years vs 1.51 at baseline). At 3-years 71% of eyes were medication-free (versus 21.6% pre-operatively). Another comparable study was carried out by Salimi et al. who published 3 year outcomes of 124 eyes with various glaucoma subtypes undergoing iStent inject® combined with cataract surgery [11]. This demonstrated a 22% reduction in IOP from 16.9 mmHg at baseline to 13.2 mmHg at 3 years, along with a decrease in IOP medication burden of 1.22 medications (1.16 at 3 years vs 2.38 at baseline). Liu et al. also published 3 year outcomes of 150 eyes with open angle glaucoma and OHT who underwent iStent inject® combined with cataract surgery [9]. A significant reduction in IOP was demonstrated at all time points with IOP reducing by 8.7% at 3 years (16.98 mmHg at baseline vs 15.51 mmHg at 3 years) but there was no significant reduction in IOP lowering medication at 3 years form a baseline of 2.54 medications (2.76 medications at 3 years).
The outcomes we demonstrate in our show a considerable reduction in IOP of 19.1% at 3 years which compares favourably to that of many other studies in the literature. This may in part be due to a relatively high baseline IOP of 18.3 mmHg, however our cohort also included patients with normal tension glaucoma (NTG) which would conversely impact the postoperative reduction in IOP that could be expected to be achieved. The relatively high baseline IOP indicates a greater disease burden in our cohort which is likely more reflective of the realities of day-to-day clinical practice compared to studies containing strict inclusion criteria leading to less representative cohorts. Despite our cohort showing a significant reduction in IOP lowering medication use, this was more modest than many other studies. Again, given the higher disease burden of our cohort, it could be expected that IOP lowering medication would be less likely to be discontinued post-operatively, regardless of the surgical outcome, owing to a more advanced glaucoma status requiring a lower IOP target.
The subgroup analysis carried out demonstrated differences in outcomes according to the disease phenotype. Although a comparable IOP reduction was seen in glaucoma (POAG/NTG) eyes compared to glaucoma suspect and OHT eyes (15.9% vs 15.7% respectively), there was a significantly greater reduction in medication burden in glaucoma suspect and OHT eyes compared to glaucoma eyes (34.5% vs 23.4% drop reduction and 39% vs 18% eyes medications free respectively). These findings could represent a tendency for clinicians to be more willing to reduce IOP medications in those without an established glaucoma diagnosis as opposed to those with established glaucoma who would have a lower target IOP. Despite this, similar IOP reductions were obtained and therefore it is possible that eyes without established glaucoma may obtain greater benefit from iStent in the presence of a ‘healthier’ trabecular meshwork and Schlemm’s canal. This is an area that warrants further investigation.
Favourable safety data from our cohort is in keeping with that of existing studies [5–11, 13–19]. An improvement in BCVA was seen in the first 2 years post-operatively (maintained thereafter), recorded minor intra-operative and post-operative complications were only marginally above the incidence seen in cataract surgery alone as per the National Ophthalmology Database audit [23]. Filtration surgery for glaucoma was subsequently required in 3.5% of eyes over 3 years (trabeculectomy or Preserflo MicroShunt). There are few studies on the rates of patients undergoing filtration surgery for glaucoma, those available demonstrate rates of 4.2% at 4 years and 5.3% at 5 years in patients newly diagnosed with POAG [24–26]. These are relatively aligned to our findings especially given many patients within our study likely had long established glaucoma diagnoses.
Despite their established safety and efficacy, IOP lowering medications have numerous drawbacks, specifically their dependence of patient adherence, local adverse effects and impact upon patients’ quality of life [27–30]. Studies have also demonstrated that a higher glaucoma medication intensity is a predictor for failure of glaucoma filtration surgery [31]. Consequently, our findings of a reduced medication burden and increase in medication free eyes post-surgery, demonstrate clear potential benefits for glaucoma patients who can achieve a given IOP with fewer potential side effects and impact upon their quality of life from their glaucoma medications in addition to possible improved outcomes if subsequent filtration surgery is required. Furthermore, many glaucoma services are shifting towards providing more ‘virtual’ clinic appointments to provide greater capacity, with recent research indicating comparable running costs to face to face clinics [32]. Medication free patients post iStent inject® combined with cataract surgery would be good candidates for ongoing review in these clinics and therefore have the potential to maximise capacity and provide benefits for service delivery. Further research is therefore warranted to establish if the use of iStent inject® combined with phacoemulsification translates in better long-term quality of life outcomes for patients, in addition to service delivery benefits for glaucoma departments.
We acknowledge that there are several limitations to our study. The absence of a control group restricts comparison between the effects of iStent inject® and that of cataract surgery alone. Studies have shown that cataract surgery alone can lower IOP by greater than 20% [33–35], however this effect wears off over time with studies demonstrating a reduction in the IOP lowering effect of cataract surgery alone as early as 12 months post-operatively [33, 34, 36]. Our study demonstrates a sustained reduction in IOP at 3 years which indicates iStent inject® may have a role in sustaining IOP reductions beyond that of cataract surgery alone. Furthermore, studies directly comparing combined iStent and cataract surgery to that of cataract surgery alone have shown greater reductions in IOP and reduced medication burden in those undergoing iStent combined with cataract surgery [14–16]. The efficacy of iStent inject alone has also been demonstrated in a recent 7 year prospective study with similar results to that of iStent inject combined with cataract surgery [8].
Another limitation is that no pre-operative medication washout was performed (of IOP lowering medications), which could potentially decrease the IOP lowering effect and reduction in medication burden post-operatively. However, real-world practice often necessitates the continuation of IOP lowering medication, given the risk of progression especially in patients with moderate to advanced glaucoma whilst awaiting surgery and in the immediate post-operative period. Although no cases of corneal decompensation were recorded, corneal endothelial cell counts were not measured pre and post operatively. This is an area that requires more research to understand the impact of angle surgery such as iStent inject® on the cornea (a protocol has now been introduced in our institution to measure pre and post operative endothelial cell counts for all patients undergoing MIGS or filtration surgery). Finally, the cohort of patients followed up to 3 years was significantly smaller than earlier time points. With healthcare service pressures and limited appointment availability there is a possibility longer follow up is biased towards patients with suboptimal IOP control as opposed to stable patients who require less frequent or even community follow up.
Conclusions
This large, real-world cohort demonstrates a significant and sustained IOP reduction with a marked improvement in medication burden 3 years after combined iStent inject® implantation and phacoemulsification. An excellent safety profile was displayed with a low rate of further glaucoma surgery required. These findings were demonstrated in a diverse patient cohort including both open and closed angle glaucoma with varying disease severity and OHT. Further research is warranted to establish if the use of iStent inject® combined with phacoemulsification translates in better long-term quality of life outcomes for patients, in addition to service delivery benefits for glaucoma departments.