Clinical characteristics of Treponema denticola-associated lung abscess diagnosed by metagenomic next-generation sequencing: a case series analysis
Hangdi Xu, Yueqing Xu, Jing Gu, Xiaoling Wang, Bo Liao, Pengpeng Zhou, Shengjun Wu, Ran Tao, Ying Fu

TL;DR
This study reports on seven cases of lung abscess caused by Treponema denticola, highlighting the importance of metagenomic sequencing for accurate diagnosis and effective treatment.
Contribution
The study identifies T. denticola as a cause of lung abscess and demonstrates the diagnostic value of mNGS over traditional methods.
Findings
Seven patients with T. denticola lung abscess were diagnosed using mNGS, all with oral disease and chronic symptoms.
Conventional cultures failed to detect T. denticola, emphasizing the need for mNGS in anaerobic infections.
β-lactams and tetracyclines showed better treatment responses compared to fluoroquinolones in some cases.
Abstract
Treponema denticola is an oral anaerobic bacterium commonly associated with periodontitis, but its role in lower respiratory tract infections (e.g., lung abscess) has long been overlooked. For bacteria that grow anaerobically, traditional culture methods exhibit low detection rates, which directly lead to the mis-diagnosis of anaerobic infection. With the ultilization of metagenomic next-generation sequencing (mNGS) in clinical practice, we studied the clinical features and treatment strategies of T. denticola-associated lung abscess. A retrospective analysis was conducted on patients confirmed with T. denticola lung abscess by mNGS from October 2023 to October 2024. Routine aerobic bacterial culture and stains were used. Histopathological analysis and Warthin-Starry silver staining was completed on samples from lung tissue. A literature review was performed using PubMed and CNKI (up…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
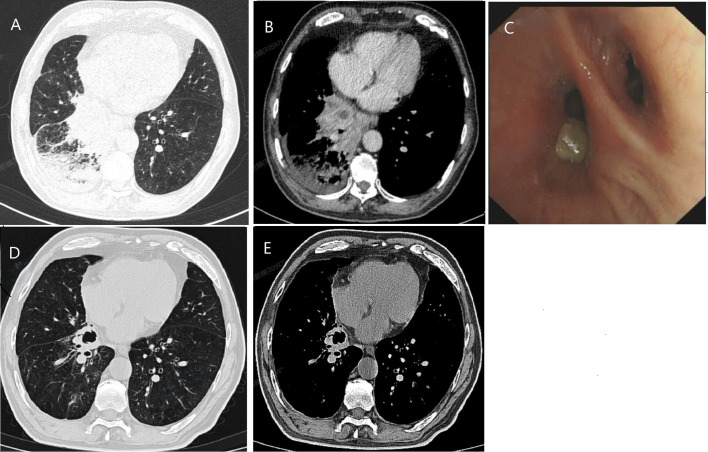 Figure 1
Figure 1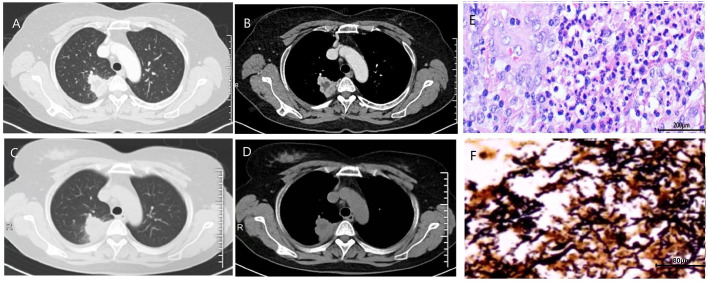 Figure 2
Figure 2| Case | Age | Sex | Underlying disease | Smoking/ drinking | Poor oral hygiene | Symptoms | Time | WBC 109/L | NEU 109/L | Hgb g/L | PCT ng/mL | CRP mg/L | Lesion site | Lesion size (mm) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 69 | male | HPT | Y/Y | Y | Cough and sputum, hemoptysis | 5M | 5.8 | 4.08 | 97 | – | 51.6 | Right upper lung mass with necrosis and cavity | 55*54 |
| 2 | 60 | male | – | Y/N | Y | Fever, cough and sputum, hemoptysis | 2M | 10.7 | 9.63 | 105 | <0.04 | 59 | Left lower lung mass with necrosis and cavity | 51*48 |
| 3 | 55 | male | DM | N/N | Y | Cough and sputum, hemoptysis | 3M | 10 | 8.98 | 139 | <0.04 | 1.1 | Right lower lung mass with necrosis and cavity | 21*14 |
| 4 | 61 | female | – | N/N | Y | Cough and chest pain | 3M | 5.7 | 3.42 | 127 | <0.04 | 10.2 | Right upper lung mass with necrosis and cavity | 45*26 |
| 5 | 77 | male | – | N/N | Y | Cough and hemoptysis | 10M | 5.1 | 2.43 | 122 | – | 6 | Right upper lung mass with cavity | 43*23 |
| 6 | 47 | male | – | Y/N | Y | Cough and sputum, hemoptysis | 1.5M | 10.6 | 7.85 | 147 | – | 1.6 | lingular segment mass with necrosis | 28*22 |
| 7 | 67 | male | DM, HPT | N/N | Y | Hemoptysis, dyspnea | 1M | 11.9 | 9.67 | 147 | <0.04 | 125 | Right lower lung mass with necrosis and cavity | 67*54 |
| Case | Samples for mNGS test | mNGS Results | Bacterial culture results | WS | Medication treatment | Surgical intervention | Prognosis | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Pathogens (genus) | Relative abundance (%) | Specific metagenomic reads | ||||||||
| 1 | BALF |
| 44.48 | 135174 | / | NF | + | Levofloxacin 0.5g once a day for 10 days, Sitafloxacin 50mg every 12 hours for 3months. | Yes | Cured with resection |
|
| 12.70 | 33514 | / | |||||||
|
| 7.53 | 45309 | 22.2% | |||||||
|
| 1.25 | 4541 | / | |||||||
|
| 31.98 | 176368 | / | |||||||
| 2 | Lung tissue |
| 22.53 | 83 | / | ND | – | Levofloxacin 0.5g once a day for 1 months | Yes | Cured with resection |
|
| 14.29 | 91 | 42.9% | |||||||
|
| 10.44 | 78 | / | |||||||
|
| 7.69 | 33 | / | |||||||
|
| 6.59 | 36 | / | |||||||
| 3 | BALF |
| 83.37 | 10433 | 52.0% | NF | / | Moxifloxacin 0.4g once a day for 2 months | No | Co-infected with |
|
| 6.48 | 889 | / | |||||||
|
| 2.45 | 283 | / | |||||||
| 4 | Lung tissue |
| 54.59 | 2153430 | / | ND | + | Levofloxacin 0.5g for 1 month, Cefmetazole 1g every 8 hours for 10 days. | Yes | Cured with resection |
|
| 26.78 | 897923 | / | |||||||
|
| 15.65 | 555456 | 26.3% | |||||||
|
| 1.65 | 75130 | / | |||||||
| 5 | Lung tissue |
| 87.72 | 6105122 | 60.9% |
| + | Doxycycline 0.1g every 12 hours for 7 months | No | Cured with medicines |
|
| 4.11 | 549318 | / | |||||||
|
| 3.09 | 196958 | / | |||||||
|
| 2.56 | 150297 | / | |||||||
| 6 | BALF |
| 18.68 | 139200 | 44.8% | NF | / | Amoxicillin clavulanate 375mg every 8 hours for 2 months | No | Cured with medicines |
|
| 1.54 | 7509 | / | |||||||
|
| 1.83 | 8454 | / | |||||||
|
| 66.52 | 469101 | / | |||||||
| 7 | BALF |
| 54.78 | 182982 | 47.0% | NF | / | Moxifloxacin 0.4g once a day for 2 months, Sitafloxacin 50mg every 12 hours for 6 months | No | Cured with medicines |
|
| 7.50 | 26533 | / | |||||||
|
| 6.38 | 16934 | / | |||||||
|
| 4.21 | 5908 | / | |||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Oral and Craniofacial Lesions · Sinusitis and nasal conditions
Introduction
1
Treponema denticola (T. denticola) is a Gram-negative, obligate-anaerobic spirochete that is widely distributed in human subgingival plaque (Ishihara, 2010; Goetting-Minesky et al., 2021). It is classically associated with periodontitis and can form intricate biofilms with other oral anaerobes—such as Porphyromonas gingivalis and Tannerella forsythia—thereby synergistically amplifying pathogenicity and promoting the development of periodontal abscesses (Dashper et al., 2011; Ng et al., 2019). When host immunity is compromised or the oral microbiota becomes dysbiotic, oropharyngeal organisms can be aspirated or disseminated hematogenously to the lower respiratory tract, resulting in pulmonary infection and abscess formation (Bartlett, 2005). Although the role of T. denticola in periodontitis is well established, its contribution to lung infections has long been overlooked. This neglect stems largely from the fastidious culture requirements of anaerobes-conventional culture methods demonstrate remarkably low detection rates for anaerobic spirochetes. Studies report positive culture rates below 30% for sputum or pus specimens, with some series reporting 0% in positive rate (Su et al., 2022; Zhang et al., 2025).
Metagenomic next-generation sequencing (mNGS) has revolutionized the diagnosis significantly, especially in anaerobic infections. Clinical data demonstrate that mNGS achieves 67.7% positive rate in etiological diagnosis of lung abscesses, markedly higher than that of traditional culture (Su et al., 2022; Zhang et al., 2025). Notably, mNGS boosts anaerobic pathogen detection to 93.8%-100%, with particular diagnostic advantages for sterile-site specimens like biopsy tissues or pleural fluid (Chen et al., 2021b).
In contrast to the absence of reported cases in our hospital over the previous five years, we report seven cases of T. denticola -associated lung abscesses diagnosed during the first year following the introduction of mNGS. We further analyzed their clinical manifestations, diagnostic approaches, and treatment strategies. In addition, we conducted a comprehensive review and in-depth analysis of previously reported cases through a systematic literature search. Our findings not only expand the current understanding of T. denticola-associated pulmonary abscesses but also provide evidence to support the optimization of management strategies for refractory cases.
Patients and methods
2
Patients
2.1
This retrospective study screened patients with lung abscesses treated at Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University from October 2023 to October 2024. mNGS of bronchoalveolar lavage fluid (BALF) or lung biopsy specimens were collected for pathogenic identification, consistent with clinical evidence. The association between lung abscess and T. denticola was confirmed by two senior pulmonologists and one senior laboratory physician. The study ultimately enrolled seven patients with T. denticola-associated lung abscesses. Comprehensive clinical data were collected, including demographic characteristics (age, sex), underlying diseases, clinical manifestations, disease progression, laboratory and radiological findings, molecular diagnostic results, treatment regimens, and prognosis.
Assessment of oral health status
2.2
All patients underwent a clinical oral examination performed by a dentist, including assessments for dental caries, periodontal status, dental plaque, and dental calculus. The diagnosis of periodontitis was based on the criteria established at the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions (Papapanou et al., 2018). Dental calculus and plaque were evaluated according to the Chinese Stomatological Association’s guideline, “Standard of periodontal examination and evaluation during oral diagnosis and treatment” (Society of Periodontology, 2021). Poor oral hygiene was defined as a Plaque Index score ≥3 (Society of Periodontology, 2021; Lertpimonchai et al., 2017) or a Calculus Index score ≥2, which indicates the presence of subgingival calculus.
Traditional microbiological methods
2.3
Different processing procedures were applied to BALF and lung tissue samples. For BALF samples, centrifugation at 3500 rpm was performed prior to culture and staining, and the resulting pellet was used for subsequent analyses. Lung tissue samples were used directly for further detection. Three types of culture media (Bioivd Biotechnology [Zhengzhou] Co., Ltd.) were used for bacterial isolation and identification, including Columbia Blood Agar, Haemophilus influenzae Agar (HAE), and Sabouraud Dextrose Agar (SDA). All plates were incubated under 5% CO^2^ at 35 ± 2°C for up to seven days. Suspected colonies growing on the plates were subsequently subcultured and subjected to species-level identification using Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS; bioMérieux Shanghai Biotech Co., Ltd.). In addition, Gram staining, fungal fluorescence staining, and acid-fast staining (Wuhan Baso Medical Device Co., Ltd.) were performed for the detection of bacteria, fungi, and Mycobacterium spp., respectively. Anaerobic culture was not involved. The identification and interpretation of suspected colonies isolated from BALF were performed according to the IDSA/ATS guidelines (Kalil et al., 2016). The interpretation of pathogens and normal flora are based on references from The ABX Guide and Manual of Clinical Microbiology (11th Edition) (University., 2024; David et al., 2015).
mNGS test
2.4
BALF or lung tissue samples were collected and then transported on dry ice to clinical laboratory within 4 hours for mNGS testing. Following the established protocol, cellular materials in samples were lysed and enriched. Total nucleic acid extraction kits and mNGS DNA library preparation kits (Tiangen Biotech Co., Ltd, China) were used for sequencing library construction. Metagenomic sequencing was performed on the BGISEQ platform, and bioinformatic analysis was conducted following the standardized mNGS protocol established by Dian Diagnostics Group Co., Ltd (Hangzhou, China) (Sun et al., 2024), with additional species-specific validation steps for T. denticola. Briefly, the raw sequencing data were processed through quality control using fastp (v0.24.1) to remove adapter sequences and filter out low-quality reads. Host-derived sequences were subsequently removed by alignment to human reference genomes (hg38, YH genome, and T2T-CHM13) using BWA-MEM (v0.7.17-r1188). Non-human reads were taxonomically classified by alignment against an in-house pathogenic microorganism database using BWA-MEM. For T. denticola confirmation, candidate reads were aligned to the reference genome of the T. denticola type strain (GenBank accession: NC_002967.9) using BWA-MEM. Read counts were quantified using custom in-house scripts. To ensure species specificity, pathogen-specific reads were further validated by BLASTn against the NCBI nucleotide (nt) database. Detection reliability was ensured through the inclusion of negative control. Metagenomic libraries for each sample yielded ≥ 20 million high-quality reads, with a mean Q30 score ≥ 90%. The relative abundance of T. denticola was first calculated as the proportion of its mapped reads among the total microbial reads. No T. denticola signal was detected in the seven negative controls processed within the same batch.
Histopathological analysis
2.5
Lung tissue specimens were fixed in 10% neutral buffered formalin for at least 24 hours. Following fixation, the tissues were dehydrated through a graded ethanol series, cleared in xylene, and embedded in paraffin. Sections were cut at a thickness of 4-5 μm using a microtome and subsequently stained with hematoxylin and eosin (H&E) according to standard protocols (Dunn et al., 2024). For the histopathological detection of spirochetes, Warthin-Starry staining was conducted following an established laboratory protocol based on the method of Graham et al (Graham et al., 2018).
Literature review
2.6
To comprehensively identify all published studies on lung abscess associated with T. denticola, two investigators (Hangdi Xu and Ying Fu) independently searched PubMed and China National Knowledge Infrastructure (CNKI) up to June 30, 2025. The search terms were the following key words: (“odontogenic flora” or “Treponema denticola” or “T. denticola” or “red-complex”) and (“lung abscess” or “lung infection” or “pneumonia”).
Results
3
General clinical features
3.1
The basic characteristics of the seven patients in our cohort are summarized in Table 1. The cohort predominantly consisted of elderly males (age range: 47–77 years), with five patients aged over 60 years. None of the patients had documented immunodeficiencies or histories of immunosuppressive therapy. Three patients had underlying comorbidities, including diabetes mellitus, coronary heart disease, and hypertension. All patients exhibited poor oral hygiene (as defined in the methods) with significant dental plaque (mean index: 3.57) and calculus accumulation (mean index: 1.71) (Supplementary Table 1). Patients with T. denticola-associated lung abscess typically present with a chronic disease course, demonstrating an average diagnostic delay of 3.6 months from symptom onset to definitive diagnosis. The clinical manifestations are mainly respiratory symptoms such as cough and sputum production, while systemic inflammatory responses are relatively mild, with only one case accompanied by fever. It is worth noting that over 85% of patients (6/7 cases) experienced hemoptysis.
Laboratory tests, chest CT and bronchoscopy
3.2
The results of routine blood tests upon admission showed that 4 patients had a mild increase in white blood cell count, while the remaining 3 patients had normal results, with a median of 8.5 × 10 ^9^/L (5.1-10.6 × 10 ^9^/L). CRP levels were normal or mildly elevated (<60 mg/L) in 6 patients, with only one case exceeding 100 mg/L (36.2 mg/L, 1.1–125 mg/L). The procalcitonin (PCT) levels of the patients are normal.
Chest CT demonstrated mass-like opacities with necrosis in all seven cases, among which five exhibited cavitation without air-fluid levels (Figures 1, 2). The lesions were distributed in Right upper lobe (3 cases), Right lower lobe (2 cases), Left lingular lobe (1 case), and Left lower lobe (1 case). The bronchoscopic manifestations included congestion and edema of the affected bronchial mucosa with purulent discharge within partial bronchial lumina (Figure 1).
The initial chest CT of case 7 demonstrated mass-like opacities and necrosis (A, lung window; B, soft tissue window). After 6 months of treatment, a follow-up lung CT scan showed significant absorption and improvement of the lung lesion, with residual cavities (D, lung window; E, soft tissue window). Bronchoscopy examination shows purulent discharge in the lumen of the basal segment branch of the right lower lobe (C).
The initial chest CT of case 4 demonstrated mass-like opacities and necrosis (A, lung window; B, soft tissue window). After 1 month of treatment with levofloxacin and 10 days of treatment with cefmetazole, the patient’s lung lesions enlarged (C, lung window; D, soft tissue window). Histopathological examination of the surgically resected lesions revealed characteristic features of chronic lung abscess (E). Warthin-Starry silver staining revealed numerous black, spiral-shaped bacteria, confirming the presence of spirochetes (F).
Microbiological examinations
3.3
The microbiological etiology of the seven patients is summarized in Table 2. mNGS performed on four BALF or three lung tissue samples revealed a spectrum of oral anaerobic pathogens. Bacteria belonging to the Treponema genus were identified in all seven cases. Furthermore, in six cases, the Treponema genus constituted one of the three most abundant microbial groups in the community. A critical finding was that T. DeNicola represented a substantial proportion (ranging from 22.2% to 60.9%) of the total Treponema population in the cases where this specific quantification was available, underscoring its dominance within this genus (Supplementary Table 2). In contrast, conventional pathogen cultures of BALF or sputum were overwhelmingly negative, with Streptococcus constellatus isolated in only a single case (Table 2).
Histopathological validation by Warthin-Starry staining
3.4
To obtain direct morphological evidence of spirochete presence, we performed Warthin-Starry silver staining on archived formalin-fixed, paraffin-embedded lung tissue samples from four patients who underwent surgical resection or biopsy (Cases 1, 2, 4, and 5). Notably, three of these four cases (Cases 1, 4, and 5) demonstrated positive staining, revealing abundant black, spiral-shaped bacteria within the necrotic cores of the pulmonary abscesses (Figure 2).
Treatment and prognosis
3.5
One patient achieved near-complete radiographic resolution after a 2-month course of amoxicillin-clavulanate, while another case showed significant improvement with residual fibrous streaks following 7 months of doxycycline therapy. The remaining 5 patients were initially treated with quinolone drugs (levofloxacin or moxifloxacin), with divergent clinical outcomes. Among them, 3 cases were converted to surgical resection of the lesion due to poor response to medical therapy, including one case complicated by massive hemoptysis. All surgical specimens exhibited histopathological features of chronic lung abscess, including dense neutrophilic and lymphocytic infiltration with micro-abscess formation, alveolar histiocyte accumulation, and organizing pneumonia (Figure 2). These patients achieved complete recovery post-resection. One patient developed concomitant nontuberculous mycobacterial (NTM) infection during moxifloxacin treatment, necessitating conversion to a regimen of rifampin, ethambutol, and azithromycin, though with persistent infection. Another case showed marked improvement after switching from ineffective moxifloxacin to a 6-month sitafloxacin course, ultimately achieving infection control with residual cavitary changes (Figure 1).
Literature review
3.6
Systematic literature retrieval identified one documented case of T. denticola-associated lung abscess in each of PubMed and CNKI databases, with both cases presenting poor periodontal health and active dental disease (Guo et al., 2019; Bao and Tang, 2021). Hemoptysis was the predominant symptom in both cases. Chest CT imaging revealed typical lung abscess formation. mNGS analysis of biopsy tissues suggests T. denticola is very possible as one of the potential pathogens. The initial treatment of one case was moxifloxacin, and there was no significant clinical improvement. Following diagnosis, intravenous penicillin G was administered for a 6-week (Bao and Tang, 2021). Follow-up imaging revealed marked abscess resolution. The other patient received a 2-month course of metronidazole plus oral amoxicillin/clavulanate, with subsequent significant reduction in pulmonary mass size post-treatment (Guo et al., 2019).
Discussion
4
Reports of Treponema denticola-associated lung abscess are exceedingly rare, with only two documented cases worldwide to date (Guo et al., 2019; Bao and Tang, 2021). Clinicians’ understanding of this condition remains highly limited. This study presents seven cases of Treponema denticola lung abscess confirmed by metagenomic next-generation sequencing (mNGS), systematically analyzing their clinical manifestations, diagnostic approaches, and treatment outcomes. These findings provide crucial insights for the diagnosis and management of this rare infection.
It is reported that patients with poor oral health (periodontal disease) and compromised immune systems are more likely to develop lung abscesses (Guo et al., 2019; Takayanagi et al., 2010), with over 60% of lung abscess patients found to have periodontal disease. As a common anaerobic bacterium in the oral cavity, T. denticola may translocate to the lungs through micro-aspiration, potentially establishing infection in the setting of impaired host defenses (Zhang et al., 2024; Shao et al., 2023). In this series of seven cases, none of the patients had significant immunosuppression, but all exhibited poor oral hygiene with significant dental plaque and calculus accumulation, which can lead to dysbiosis of the oropharyngeal microbiota and increase the risk of colonization and proliferation of opportunistic pathogens. Moreover, our patients were predominantly elderly (with an average age of 62.3 years), as age-related declines in both cough reflex sensitivity and immune competence create favorable conditions for opportunistic pulmonary infections. Interestingly, although alcohol abuse has been established as a recognized risk factor for lung abscess (Vaarst et al., 2023; Mohapatra et al., 2018), it did not emerge as a significant contributor in our series, with only one male patient reporting substantial alcohol consumption.
The clinical presentation of *T. denticola-*associated lung abscesses demonstrates several distinctive features. Patients typically exhibit non-specific respiratory symptoms, with cough and sputum production being predominant manifestations, while systemic inflammatory responses remain relatively mild. The disease course tends to be indolent, as evidenced by our cohort’s mean diagnostic delay of 3.6 months. Such mild inflammatory parameters (normal or slightly elevated biomarkers) frequently lead to misdiagnosis as non-infectious conditions (e.g., tuberculosis or lung cancer), likely reflecting the low virulence and chronic infection patterns characteristic of T. denticola.
Radiologically, chest CT mainly presents as pulmonary mass accompanied by liquefactive necrosis and small cavity formation, typically without air-fluid levels - a potentially distinguishing feature from conventional pyogenic abscesses. A striking clinical observation was the high prevalence of hemoptysis (85.7%, 6/7 cases), including one case of life-threatening massive hemoptysis. This incidence markedly exceeds the 21.7% hemoptysis rate reported in typical lung abscesses (Montméat et al., 2024), a finding corroborated by the two previously reported cases where hemoptysis was also the cardinal symptom (Guo et al., 2019; Bao and Tang, 2021).
The development of tissue necrosis and hemoptysis in T. denticola infections likely results from a complex interplay of bacterial virulence factors and host inflammatory responses. Key virulence determinants, including major surface protein (MSP) and chymotrypsin-like protease complex (CTLP), directly compromise cellular integrity through degradation of extracellular matrix (ECM) components, leading to substantial tissue damage (Dashper et al., 2011). Additionally, CTLP, MSP, lipooligosaccharides, and the cysteine-desulfhydrase enzymes HlyA (also known as Cystalysin) contribute to the pathogenic process by exhibiting cytotoxic effects that promote cellular dysfunction and death (Chu et al., 1999). Concurrently, T. denticola infection elicits a robust local inflammatory response characterized by macrophage activation and elevated secretion of proinflammatory mediators, particularly IL-6, IL-8, and RANTES. This inflammatory cascade is further amplified through activation of multiple intracellular signaling pathways, including PKA, ERK2, JNK, and p38, which collectively enhance production of inflammatory cytokines (Kimizuka et al., 2003; Asai et al., 2003; Deng et al., 2001; Nixon et al., 2000). The combined effects of direct bacterial cytotoxicity and sustained inflammatory stimulation result in significant microvascular injury, manifested by increased vascular permeability, capillary damage, and ultimately vascular rupture.
As an anaerobic pathogen, T. denticola has posed significant diagnostic challenges due to its fastidious growth requirements and the technical difficulties associated with anaerobic specimen collection and transport (Fenno, 2012). Conventional culture methods frequently yield false-negative results, particularly when analyzing sputum or upper respiratory secretions that are often contaminated with oral commensal flora (Gao et al., 2025). These limitations have contributed to the underrecognition of anaerobic organisms in pulmonary abscess etiology. Comparing to traditional techniques, mNGS provides an unbiased detection of all microbial nucleic acids in clinical samples, encompassing bacteria, viruses, fungi, and parasites, which proves particularly valuable for identifying anaerobic bacteria, rare organisms, and polymicrobial infections (Li et al., 2018; Shi et al., 2023; Lee et al., 2025). The detection rate of anaerobic bacteria in traditional sputum culture is only 20% -30%, while the detection rate of anaerobic bacteria in mNGS can reach over 80% (Huang et al., 2020; Chen et al., 2021a) While mNGS represents a transformative diagnostic tool for rare pathogens, its clinical application requires careful interpretation (Zhang et al., 2024). Our histopathological findings provide tangible morphological support for the mNGS results. The detection of spiral-shaped bacteria via Warthin-Starry staining in three of four tested cases offers independent visual confirmation of spirochetes within the abscess material (Figure 2). Although this special stain cannot specifically identify T. denticola at the species level, the combination of positive staining with the species-specific mNGS data creates a compelling chain of evidence. This multi-methodological approach significantly strengthens the etiological linkage between T. denticola and the observed pulmonary pathology.
The interpretation of mNGS results in the context of polymicrobial infections warrants careful consideration. In our series, T. denticola was detected as the predominant organism in three cases (Cases 3, 5& 7), suggesting a primary pathogenic role. However, in the majority of cases, it was co-detected with other recognized oral pathogens, such as P. gingivalis and S. constellatus. In these instances, the relative abundance of T. denticola varied and was sometimes lower than that of its partners. This finding aligns with the established model of polymicrobial synergy in periodontal disease, particularly within the ‘red complex’ (Mahendrarajan et al., 2025). Within this complex, T. denticola, though not always the most abundant, may facilitate infection through its potent virulence factors, such as CTLP, which disrupts host tissues and enables co-colonization by other pathogens (Mahendrarajan et al., 2025; Kamarajan et al., 2024). Therefore, the clinical significance of T. denticola likely extends beyond its relative abundance in sequencing data, encompassing its key role in initiating and sustaining a dysbiotic, pathogenic consortium.
T. denticola demonstrates susceptibility to multiple classes of antimicrobial agents. In vitro studies by Pawar et al. revealed that various Treponema species maintain sensitivity to penicillin, tetracycline, imipenem, cefoperazone, clindamycin, and moxifloxacin, while exhibiting partial resistance to metronidazole (Pawar et al., 2024). Kazuko et al. demonstrated that doxycycline, minocycline, azithromycin, and erythromycin exhibit consistent activity against T. denticola, T. socranskii, and T. vincentii. Notably, fluoroquinolones showed limited efficacy, demonstrating activity only against T. socranskii while remaining ineffective against both T. denticola and T. vincentii (Okamoto-Shibayama et al., 2017). This laboratory findings align with our clinical observations. Patients treated with amoxicillin-clavulanate or doxycycline regimens demonstrated favorable therapeutic responses. Conversely, fluoroquinolones (moxifloxacin or levofloxacin) appear to have limited clinical utility against this pathogen. Notably, one representative case showed disease progression during moxifloxacin treatment but subsequently responded well to sitafloxacin (STFX). This observation aligns with the antimicrobial susceptibility findings reported by Kazuko et al., who documented STFX’s superior anti-treponema activity, demonstrating MIC values 4–8 times lower than those of ofloxacin and levofloxacin (Okamoto-Shibayama et al., 2017). The development of quinolone resistance in T. denticola appears mediated through multiple molecular mechanisms, including genetic mutations in DNA gyrase and topoisomerase IV, coupled with ATP-binding cassette (ABC) transporter-mediated efflux systems (Okamoto-Shibayama et al., 2017; Hooper and Jacoby, 2016). These findings suggest that while β-lactam/tetracycline-based regimens remain first-line options, the potential role of STFX in quinolone-resistant cases warrants further investigation. Therefore, we should search for the pathogen as early as possible for a clear diagnosis, choose antibiotic treatment that is sensitive to the identified pathogen, and achieve the transition from empirical treatment to targeted treatment. In addition, the results of this study showed that T. denticola are prone to co infection with other anaerobic bacteria, enhancing their resistance to antibiotics and host immunity, resulting in poor anti infection effects. Pulmonary abscess caused by T. denticola often presents as a chronic disease course with a relatively long overall treatment time. For patients with ineffective internal medicine treatment or massive hemoptysis, surgical resection of the lesion is an effective means of controlling bleeding and clearing the source of infection. In this group of 3 patients (42.9%), the infected lesions were ultimately completely removed through surgical intervention.
Several limitations should be considered about our findings. Firstly, the small sample size (n=7) may introduce selection bias and limit the generalizability of our observations. Furthermore, T. denticola was co-detected with other oral commensal bacteria in some cases. However, the limited number of cases precluded further investigation into how such co-infections influence clinical presentation or therapeutic outcomes. A key methodological limitation was the absence of anaerobic culture. Although this reflects real-world clinical challenges, it means we could not obtain cultured isolates for phenotypic confirmation. However, this limitation was mitigated by the histopathological evidence from Warthin-Starry staining, which confirmed the physical presence of spirochetes within the lesions in the majority of tested cases, thereby providing independent validation that aligns with the mNGS results.
Conclusion
5
This study represents the first case series analysis of T. denticola-associated lung abscesses, providing valuable insights into the diagnosis and management of this uncommon clinical entity. Our findings demonstrate that T. denticola lung abscess typically affects individuals with poor oral health, presenting as indolent infections with prominent hemoptysis. Typical CT findings include a mass-like lesion with cavitation but no air–fluid level. Traditional microbiological methods frequently fail detection, establishing mNGS as the diagnostic cornerstone. The antibiotics including β-lactams and tetracyclines represent optimal antimicrobial choices, while fluquinolones demonstrate restricted utility. Surgical management remains crucial for refractory cases or life-threatening hemoptysis. Though providing valuable insights into this uncommon infection, our findings warrant corroboration through larger-scale investigations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asai Y. Jinno T. Ogawa T. (2003). Oral treponemes and their outer membrane extracts activate human gingival epithelial cells through toll-like receptor 2. Infect. Immun. 71, 717–725. doi: 10.1128/IAI.71.2.717-725.2003, PMID: 12540550 PMC 145376 · doi ↗ · pubmed ↗
- 2Bao X. Tang N. (2021). A case of hemoptysis caused by Treponema denticola pneumonia. Chin. J. Respir. Crit. Care Med. 20, 889–891. doi: 10.7507/1671-6205.202103032 · doi ↗
- 3Bartlett J. G. (2005). The role of anaerobic bacteria in lung abscess. Clin. Infect. Dis. 40, 923–925. doi: 10.1086/428586, PMID: 15824980 · doi ↗ · pubmed ↗
- 4Chen Y. Feng W. Ye K. Guo L. Xia H. Guan Y. . (2021 a). Application of metagenomic next-generation sequencing in the diagnosis of pulmonary infectious pathogens from bronchoalveolar lavage samples. Front. Cell Infect. Microbiol. 11, 541092. doi: 10.3389/fcimb.2021.541092, PMID: 33777827 PMC 7991794 · doi ↗ · pubmed ↗
- 5Chen Y. H. Zheng H. Y. Li Z. X. Wu Y. C. Niu Z. X. Peng Y. H. . (2021 b). Distribution of bacteria infected by metagenomic sequencing technology in maxillofacial space. Hua Xi Kou Qiang Yi Xue Za Zhi 39, 475–481. doi: 10.7518/hxkq.2021.04.016, PMID: 34409806 PMC 8381121 · doi ↗ · pubmed ↗
- 6Chu L. Ebersole J. L. Kurzban G. P. Holt S. C. (1999). Cystalysin, a 46-k Da L-cysteine desulfhydrase from Treponema denticola: biochemical and biophysical characterization. Clin. Infect. Dis. 28, 442–450. doi: 10.1086/515164, PMID: 10194060 · doi ↗ · pubmed ↗
- 7Dashper S. G. Seers C. A. Tan K. H. Reynolds E. C. (2011). Virulence factors of the oral spirochete Treponema denticola. J. Dent. Res. 90, 691–703. doi: 10.1177/0022034510385242, PMID: 20940357 PMC 3144123 · doi ↗ · pubmed ↗
- 8David W. Warnock G. F. James H. Jorgensen Michael A. Pfaller, Marie L. . (2015). Manual of Clinical Microbiology. 11th ed (Washington, DC: ASM Press).