Splenic Torsion in a Patient with Polysplenia Syndrome and Dorsal Pancreatic Agenesis: A Case Report
Kensuke Kishida, Hiroshi Nemoto, Hideki Sarukawa, Ryu Matsunaga, Hajime Miyaji, Naoki Yazawa, Kunihiko Shimura, Taku Miyamae

TL;DR
A 30-year-old woman with a rare condition involving multiple spleens and a missing part of the pancreas experienced a rare complication of partial spleen twisting, which was surgically treated.
Contribution
This is the first reported case of splenic torsion in polysplenia syndrome with agenesis of the dorsal pancreas in an adult.
Findings
The patient had 5 spleens, one of which showed torsion and was surgically removed.
A vascular variation resembling Adachi type VI was identified as a contributing factor to the torsion.
This case expands the understanding of anatomical risks in polysplenia syndrome.
Abstract
Partial splenic torsion in polysplenia syndrome is an extremely rare condition. We encountered and performed surgery for a case of partial splenic torsion in a patient with polysplenia syndrome coexisting with agenesis of the dorsal pancreas. A 30-year-old woman with heterotaxy syndrome presented with intermittent epigastric and right lateral abdominal pain persisting for 2 weeks. She was referred to our hospital. Abdominal contrast-enhanced CT revealed multiple spleens on the right side, a right-sided stomach, and agenesis of the dorsal pancreas. One of the 5 spleens showed no contrast enhancement. Suspecting torsion or infarction, we opted for surgical intervention. Intraoperative findings revealed a small spleen with poor coloration and 180-degree torsion, which we removed. Additionally, we identified another poorly anchored spleen and performed splenopexy to secure this wandering…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
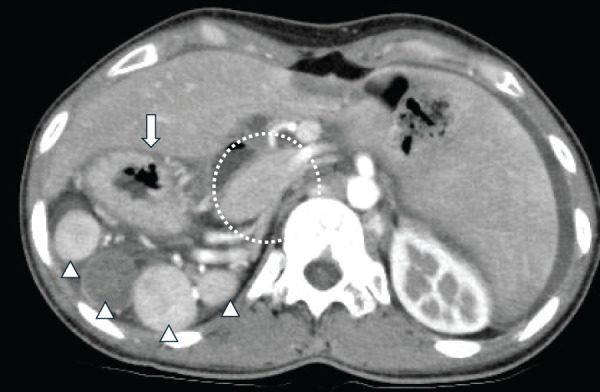 Fig. 1
Fig. 1 Fig. 2
Fig. 2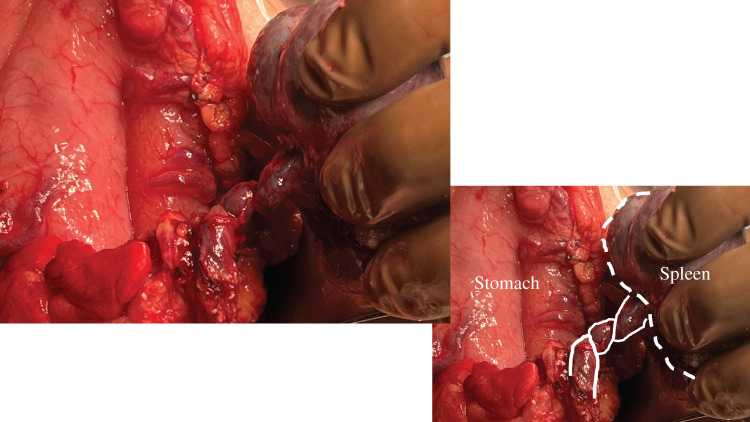 Fig. 3
Fig. 3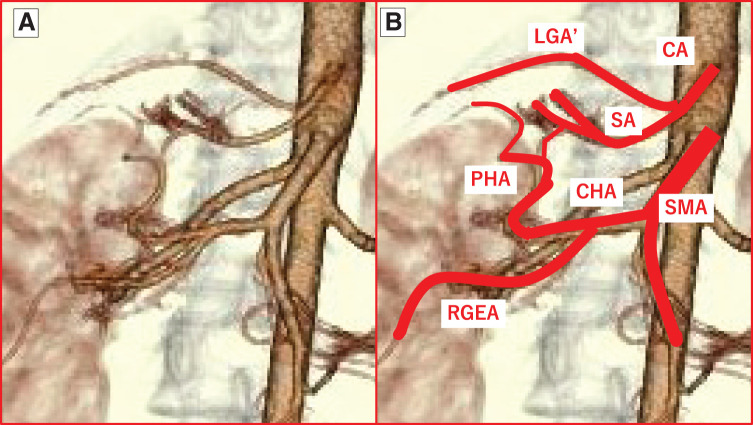 Fig. 4
Fig. 4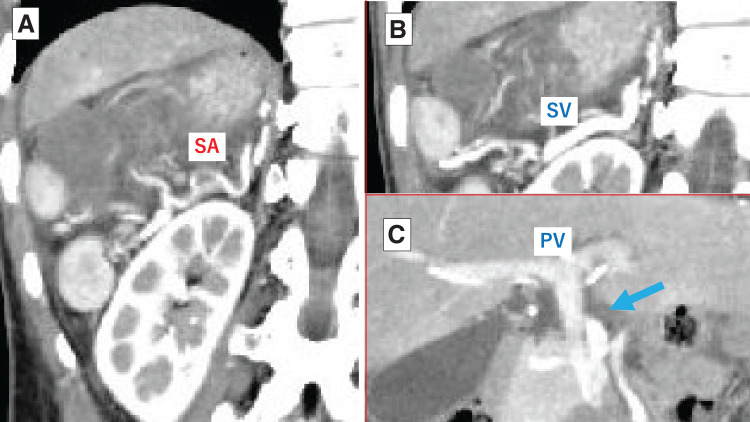 Fig. 5
Fig. 5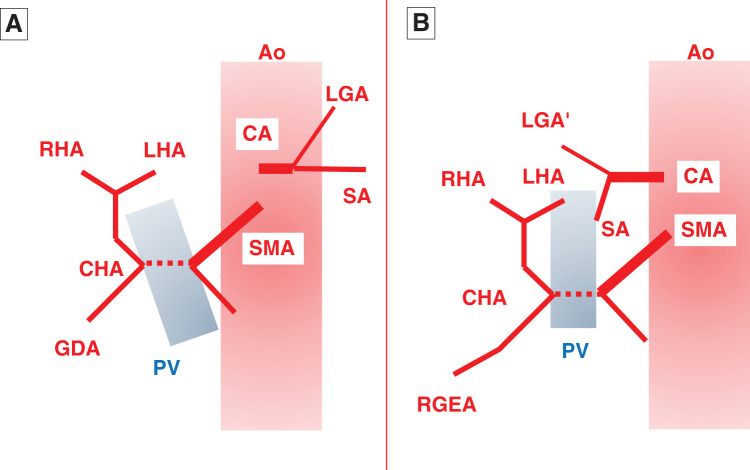 Fig. 6
Fig. 6| Authors | Year | Sex | Age | Spleen position | Numbers of torsed/total spleens | Malformation of pancreas | Other malformations and disorders |
|---|---|---|---|---|---|---|---|
| Ackerman et al. | 1982 | Female | 7 months | Right | 1/3 | AC, ML, IM, VSD | |
| Griffiths and Marshall | 1984 | Female | 23 years | Right | 2/2 | LL | |
| Lachmann et al. | 2006 | Female | 9 years | Right | 1/ND | ML, RS | |
| Rasool and Mirza | 2011 | Female | 2 days | Right | 1/7 | LL, RS, jejunal atresia | |
| Dash et al. | 2013 | Male | 12 years | Right | 1/5 | LL, RS | |
| Fujiwara et al. | 2019 | Female | 10 years | Left | 1/2 | AVSD, BA, ML | |
| Kubo et al. | 2019 | Female | 21 years | Left | 1/3 | ND | |
| Kennedy et al. | 2021 | Female | 9 years | Left | 5/7 | AP | AC, IM, preduodenal PV |
| Draghmeh et al. | 2022 | Female | 13 years | Left | 1/5 | AC, BBL, IM, ML, bicornuate uterus | |
| Cheang et al. | 2022 | Male | 8 years | Right | 1/6 | AC, ML, levocardia | |
| Present case | 2025 | Female | 30 years | Right | 1/5 | ADP | AC, BA, BBL, ML, RS, double IVC |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Congenital Heart Disease Studies · Intestinal Malrotation and Obstruction Disorders
Abbreviations
PV portal vein SA splenic artery SMA superior mesenteric artery
INTRODUCTION
Splenic torsion induced by various causes is a rare condition.^1)^ The spleen is normally anchored within the abdominal cavity by several ligaments, including the gastrosplenic, splenorenal, splenocolic, and phrenicosplenic ligaments. Among reported cases of splenic torsion, some involve torsion of a wandering spleen, which results from congenital or acquired abnormalities leading to weakened or deficient suspensory ligaments.^2,3)^ Furthermore, partial splenic torsion in the context of polysplenia syndrome—considered a specific type of wandering spleen—has also been documented, though only 10 such cases have been reported in the English literature to date.^4–13)^ These cases suggest that some spleens in patients with polysplenia syndrome may exist in a partially wandering state. We report a surgical case of partial splenic torsion in a very rare instance of polysplenia syndrome coexisting with agenesis of the dorsal pancreas.
CASE PRESENTATION
A 30-year-old woman experienced intermittent epigastric and right lateral abdominal pain that had persisted for 2 weeks. Although her family doctor performed CT and esophagogastroduodenoscopy, the cause of her abdominal pain remained unclear. She had been diagnosed with polysplenia syndrome in childhood and had a pacemaker implanted 6 years earlier for bradyarrhythmia in another hospital. She had no history of pregnancy. Because the pain had intensified the day before presentation, she was referred to our hospital. Physical examination revealed significant tenderness in the right lower quadrant without rebound tenderness. Her initial vital signs were nearly normal, and laboratory findings were unremarkable except for elevated C-reactive protein (11.19 mg/dL) and lactic acid (1.20 mmol/L).
Abdominal contrast-enhanced CT revealed multiple spleens on the right side, a right-sided stomach, midline liver, and agenesis of the dorsal pancreas (Fig. 1). One of the 5 spleens showed no contrast enhancement (Fig. 2), raising suspicion of torsion or infarction, and we decided to proceed with surgery.
CT findings of the abdomen. This image shows multiple spleens on the right side (white arrowheads), a right-sided stomach (white arrow), a midline liver, and the head of the pancreas without the dorsal pancreas (dotted circle).
Multiple spleens on CT. In the right upper quadrant of the abdomen, 3 enhanced small spleens are visible (white arrowheads), along with 1 non-enhanced spleen (black arrowhead).
The laparotomy was performed through an upper midline incision under general anesthesia. The stomach was identified in the upper right abdomen, after which the greater omentum was opened to access the omental bursa. Among the multiple spleens present, 1 small spleen appeared discolored. Because of a 180-degree twist of its splenic vessels, this spleen was ligated and excised at the hilum (Fig. 3). Another spleen was found to be poorly anchored. After confirming adequate blood flow with indocyanine green fluorescence imaging, splenopexy was performed using absorbable sutures. The remaining 3 spleens were firmly fixed to the retroperitoneum. The operation lasted 109 minutes, with a total blood loss of 50 mL. The postoperative course was uneventful, and the patient was discharged on the 5th POD.
Intraoperative findings revealed splenic torsion.
DISCUSSION
Heterotaxy syndrome, also known as situs ambiguus, is a defect in the left–right axis arrangement of the thoracic or abdominal organs, without forming a complete mirror image configuration as in situs inversus.^14)^ Right isomerism is characterized by symmetrical development of the right-sided organs and an absence of the spleen, and it is therefore referred to as asplenia syndrome. By contrast, left isomerism involves symmetrical development of the left-sided organs and the presence of multiple spleens and is known as polysplenia syndrome. Although some associated genes have been identified, the exact cause of heterotaxy syndrome remains unknown.^15)^ Numerous cardiovascular abnormalities have been reported in association with left isomerism, including interrupted inferior vena cava, atrioventricular septal defect, and single ventricle, among others.^14)^
Peoples et al.^16)^ have reported 146 cases of polysplenia syndrome, in which at least half of the patients had cardiac malformations, and 75% of them died before the age of 5 years. In the absence of severe cardiac abnormalities, however, patients with polysplenia syndrome may survive into adulthood. In polysplenia syndrome, the spleens are typically located along the greater curvature of the stomach and are often situated on the right side.^16,17)^
To date, 11 cases of splenic torsion associated with polysplenia syndrome, including the present case, have been reported in the English-language literature. These patients comprised 9 females and 2 males, ranging in age from the 2nd day of life to 30 years, with only 3 adult cases reported (Table 1). The current case represents the oldest patient among them. Detailed information on the patient’s clinical course from birth to the present—particularly concerning the cardiovascular system—was unavailable. However, we believe that the absence of severe congenital heart disease, which likely enabled survival into adolescence, may have contributed to the development of splenic volvulus at this age. Of the 11 patients, 7 had spleens located on the right and 4 on the left. In 7 of the patients for whom the number of spleens was described, 2 had multiple spleens that underwent torsion.^5,11)^ In our case as well, there was a possibility that 2 spleens could have twisted simultaneously. It is believed that among multiple spleens, those with looser fixation and longer feeding vessels are more prone to torsion. In all cases, the twisted spleen was surgically removed. In our patient, however, we also performed preventive fixation of another free spleen—an approach not described in the previous 10 cases.
As in the present case, there have been reports of polysplenia syndrome coexisting with agenesis of the dorsal pancreas.^18)^ However, among such cases, this is the 1st reported instance involving splenic torsion. Normally, the pancreas develops from 2 embryologic buds: a ventral anlage, which forms the uncinate process and pancreatic head, and a dorsal anlage, which gives rise to the body and the tail. Both the dorsal pancreas and the spleen develop within the dorsal mesogastrium, so concurrent anomalies in both organs can occur in patients with polysplenia syndrome.^18,19)^ Ongoing research into the relationship between agenesis of the dorsal pancreas and certain gene mutations may further clarify their association with polysplenia syndrome.^20,21)^
In cases of dorsal pancreatic agenesis, the fixation of vessels between the ventral pancreas and spleen may be compromised. However, in our case, although the ventral pancreas was in a normal position, the spleen was abnormally located on the right side. With the stomach also situated on the right, the stomach, duodenal bulb, descending portion of the duodenum, and pancreatic head were clustered in the upper right abdomen. Therefore, the splenic artery (SA) anatomy was likely abnormal as well, although it remains unclear whether the agenesis of the dorsal pancreas directly caused the torsion.
In fact, our patient exhibited 2 notable anatomical features. First, the complex variations of the celiac artery, superior mesenteric artery (SMA), and portal vein (PV) systems were clustered within the narrow space of the upper right abdomen. After coursing toward the right posterior side, the celiac trunk divided into an upper branch—presumed to be a variant left gastric artery—which supplied the proximal stomach, and a lower branch, the SA (Fig. 4). The SA appeared to branch into multiple vessels, forming an arterial arcade in the periphery and distributing blood to each spleen. The splenic vein ran along the right dorsal side, anterior to the SA, and joined from the left to form the PV (Fig. 5). The SMA divided into right and left branches. The right branch represented the common hepatic artery, which coursed along the dorsal side of the PV and then split into upper and lower branches on its right. The upper branch curved in an arc toward the head and became the proper hepatic artery, while the lower branch coursed caudally, passing through the pancreatic head before continuing as the right gastroepiploic artery. Except for the right-sided SA and the variant left gastric artery, this arterial pattern resembled Adachi type VI (group 24), reported in approximately 1.5% of normal individuals^22)^ (Fig. 6). Similar to the current case, 3 reports of heterotaxy syndrome have described the common hepatic artery arising from the SMA.^23–25)^ Matsuda et al.^25)^ suggested that this feature—specifically, the proper hepatic artery originating from the SMA—may be characteristic of patients with situs ambiguus accompanied by polysplenia syndrome. Notably, all of these cases, including ours, had spleens located on the right side, suggesting an association with a right-sided SA.
3D CT angiography of abdominal vasculature. (A) Front view after discharge. (B) The CA and SMA are highlighted with red lines. After coursing toward the right posterior side, the CA divides into an upper branch—presumed to be an LGA’—and a lower branch, the SA. The SMA divides into right and left branches. The right-hand branch represents the CHA, which further divides into upper and lower branches. The upper branch curves in an arc toward the head and continues as the PHA, while the lower branch passes caudally through the pancreatic head and becomes the RGEA.CA, celiac artery; CHA, common hepatic artery; LGA, left gastric artery; LGA’, variant left gastric artery; PHA, proper hepatic artery; RGEA, right gastroepiploic artery; SA, splenic artery; SMA, superior mesenteric artery
Contrast-enhanced CT on admission. (A) The SA branches into multiple vessels, forming an arterial arcade in the periphery that supplies each spleen. (B) The SV runs along the right dorsal side, anterior to the SA. (C) The SV joins from the left to form the PV (blue arrow).PV, portal vein; SA, splenic artery; SV, splenic vein
Schematic diagrams of the CA and SMA. (A) Type VI (group 24) of Adachi’s classification. The gastro-splenic and hepatomesenteric trunks independently originate from the Ao. The CHA passes dorsal to the PV and then divides into the PHA (which further branches into the RHA and LHA) and the GDA. (B) Current case. The gastro-splenic trunk, which courses to the right, and the hepatomesenteric trunk independently originate from the Ao. The CA runs rightward and then branches into an upper branch (LGA’) and a lower branch (SA). The CHA passes dorsal to the PV and divides into the PHA and the RGEA.Ao, aorta; CA, celiac artery; CHA, common hepatic artery; GDA, gastroduodenal artery; LGA’, variant left gastric artery; LHA, left hepatic artery; PHA, proper hepatic artery; PV, portal vein; RGEA, right gastroepiploic artery; RHA, right hepatic artery; SA, splenic artery; SMA, superior mesenteric artery
Second, among the 5 spleens, the centrally and dorsally positioned spleen (Fig. 2) was twisted and lacked fixation. Based on this, we hypothesize that splenic torsion in this case was caused by the floating central spleen and its relatively elongated SA. While each previously described patient may have had unique anatomical features, prior reports have not provided detailed descriptions of pancreatic or splenic vascular anomalies. Aside from our case, the only mention of coexisting pancreatic malformation was a case involving annular pancreas.^11)^ Going forward, it will be of great interest to analyze polysplenia syndrome with a focus on pancreatic anomalies and splenic vasculature. Such analyses may help identify patterns contributing to splenic torsion, potentially enabling preventive strategies in high-risk patients.
Acquired wandering spleen is more commonly observed in young women, and hormonal influences are considered as 1 contributing factor.^26)^ Thus, acquired factors cannot be ruled out in our case. When performing splenectomy, postoperative complications must be considered, especially overwhelming post-splenectomy infection. However, in this and other reported cases of splenectomy in polysplenia syndrome, many spleens were preserved, suggesting retained splenic function. Indeed, in patients with biliary atresia who underwent partial splenectomy, no fulminant infections were observed during long-term follow-up.^27)^ Nonetheless, because functional asplenia has been reported in a patient with polysplenia syndrome, careful long-term observation remains essential.^28)^
CONCLUSIONS
We encountered a rare case of splenic torsion associated with polysplenia syndrome. To date, no prior literature has suggested a relationship between pancreatic malformations and splenic torsion in such cases. Accumulation of additional cases is needed to clarify the potential relationship between pancreatic malformations and splenic torsion, as well as to assess the long-term outcomes following splenectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bough GM, Gargan KE, Cleeve SJ, et al. Diagnosis, management and outcome of splenic torsion; a systematic review of published studies. Surgeon 2022; 20: e 296–305.34666939 10.1016/j.surge.2021.08.006 · doi ↗ · pubmed ↗
- 2Koliakos E, Papazarkadas X, Sleiman M-J, et al. Wandering spleen volvulus: a case report and literature review of this diagnostic challenge. Am J Case Rep 2020; 21: e 925301.32868755 10.12659/AJCR.925301 PMC 7483514 · doi ↗ · pubmed ↗
- 3Ahmed M, Nasir M, Negash A, et al. Wandering spleen with splenic torsion: unusual cause of acute abdomen. Int Med Case Rep J 2022; 15: 625–30.36388241 10.2147/IMCRJ.S 388271 PMC 9642092 · doi ↗ · pubmed ↗
- 4Ackerman NB Jr., Smith MD, Strobel CT, et al. Splenic torsion in the polysplenia syndrome. South Med J 1982; 75: 897–8.7089667 10.1097/00007611-198207000-00043 · doi ↗ · pubmed ↗
- 5Griffiths JD, Marshall VC. Torsion of the spleen in the polysplenia syndrome. Aust N Z J Surg 1984; 54: 571–3.6596079 10.1111/j.1445-2197.1984.tb 05449.x · doi ↗ · pubmed ↗
- 6Lachmann R, Loff S, Düber C, et al. Visceral heterotaxia with polysplenia syndrome and haemorrhagic splenic infarction as a rare cause of the acute paediatric abdomen. Pediatr Radiol 2006; 36: 572–3.16534584 10.1007/s 00247-006-0111-8 · doi ↗ · pubmed ↗
- 7Rasool F, Mirza B. Polysplenia syndrome associated with situs inversus abdominus and type I jejunal atresia. APSP J Case Rep 2011; 2: 18.22953285 PMC 3418020 · pubmed ↗
- 8Dash MR, Upasani AV, Chandna SB, et al. Splenic torsion in a child with polysplenia and situs inversus: a very rare presentation. Indian J Surg 2013; 75(Suppl 1): 236–7.24426576 10.1007/s 12262-012-0668-4PMC 3693351 · doi ↗ · pubmed ↗