Improved Lung Function With Cyclophosphamide and Rituximab in a Case of Shrinking Lung Syndrome
Shiza Chaudhry, Haider Bokhary, Mark Quinn

TL;DR
A young woman with shrinking lung syndrome showed improved lung function after treatment with cyclophosphamide and rituximab.
Contribution
The paper presents a novel case of SLS successfully treated with a combination of cyclophosphamide and rituximab.
Findings
The patient exhibited hallmark symptoms of SLS, including dyspnea and reduced lung volumes.
Treatment with cyclophosphamide and rituximab led to meaningful recovery in lung function.
Early diagnosis and appropriate treatment may improve outcomes in SLS patients.
Abstract
Shrinking lung syndrome (SLS) is a rare respiratory complication of systemic autoimmune diseases. It is most commonly associated with systemic lupus erythematosus (SLE), often presenting as a diagnostic challenge. It is characterized by hallmark clinical features of dyspnea and pleuritic chest pain, along with radiographic evidence of reduced lung volumes and restrictive lung physiology in the absence of interstitial lung disease. Patients often demonstrate positive antibody serology due to associated underlying autoimmune conditions. In particular, anti-nuclear antibodies (ANA), low complement levels, and, in certain instances, extractable nuclear antigens (ENA) tend to be positive. We present a case of a young lady in her 20s who developed exertional shortness of breath, pleuritic chest pain, and reduced exercise tolerance. In the context of a positive autoimmune profile suggestive of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
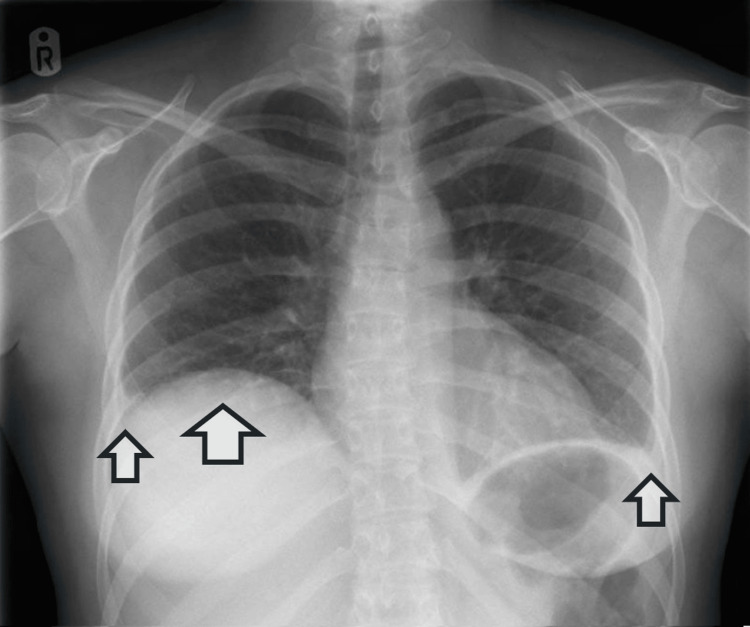 Figure 1
Figure 1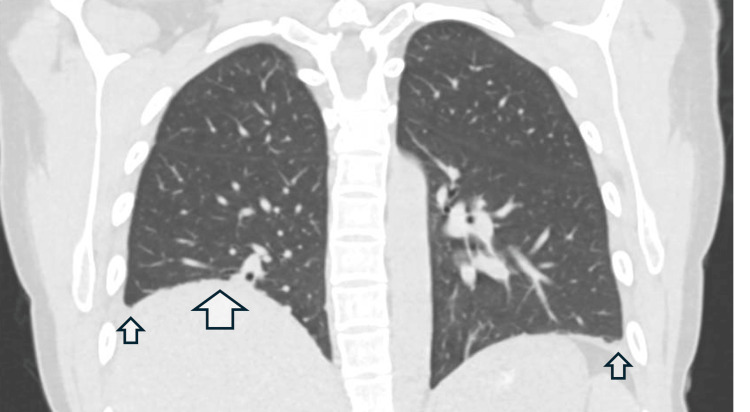 Figure 2
Figure 2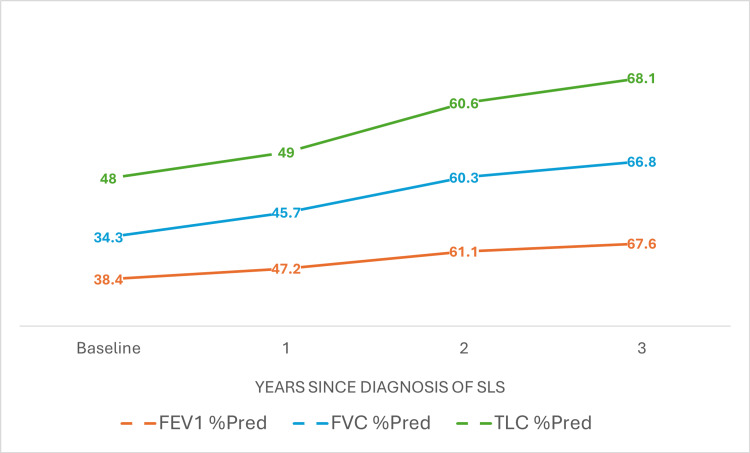 Figure 3
Figure 3| Tests | Patient’s result | Reference range |
| Full blood count | ||
| Hemoglobin | 129 g/L | 115-165 g/L |
| White blood cell count | 3.8x109/L | 4.0-11.0x109/L |
| Neutrophils | 3.1x109/L | 2.0-8.0x109/L |
| Lymphocytes | 0.4x109/L | 0.5-4.5x109/L |
| Monocytes | 0.1x109/L | 0.2-1.2x109/L |
| Platelet count | 374x109/L | 150-450x109/L |
| Mean cell volume | 88 fL | 79-101 fL |
| Inflammatory markers | ||
| CRP | 46 mg/L | 0-5 mg/L |
| ESR | 88 mm/h | 1-15 mm/h |
| Autoimmune serology | ||
| Anti-nuclear antibodies | Homogeneous 1/640 | - |
| Anti-dsDNA | 172.8 IU/L | 0.000-17.300 IU/L |
| Anti-cardiolipin | 14.7 CU | 0.0-20.0 CU |
| B2-glycoprotein IgG | 9.7 CU | 0.0-20.0 CU |
| ANCA | Negative | - |
| Anti-CCP | Negative | - |
| Extractable nuclear antigens (ENA) | ||
| Ro60 | Positive | - |
| Ro52 | Negative | - |
| Anti-RNP | Positive | - |
| Anti-Smith | Positive | - |
| Jo1 | Negative | - |
| Scl70 | Negative | - |
| Complement | ||
| C4 | 0.18 g/L | 0.10-0.40 g/L |
| C3 | 1.52 g/L | 0.90-1.80 g/L |
| Immunoglobulins | ||
| Immunoglobulin A | 2.96 g/L | 0.80-2.80 g/L |
| Immunoglobulin M | 1.72 g/L | 0.50-1.90 g/L |
| Immunoglobulin G | 21.9 g/L | 6.0-16.0 g/L |
| Urinalysis | ||
| Protein | Negative | - |
| Biochemistry | ||
| Sodium | 141 mmol/L | 133-146 mmol/L |
| Potassium | 4.0 mmol/L | 3.5-5.3 mmol/L |
| Creatinine | 60 μmol/L | 45-84 μmol/L |
| eGFR | 120 mL/min/1.73 m2 | Normal >90 mL/min/1.73 m2 |
| Urea | 3.9 mmol/L | 2.5-7.8 mmol/L |
| Variables | Predicted lower limit (in liters) | Actual (in liters) | % Predicted | Standard ratio |
| FEV1 | 3.04 | 1.45 | 38.4 | -4.95 |
| FVC | 3.50 | 1.50 | 34.3 | -5.72 |
| TLC | 4.63 | 2.70 | 48.0 | -4.86 |
| TLCO | 6.59 | 4.36 | 51.4 | -4.61 |
| Studies | Age (years)/sex | Clinical features of SLS | Antibody profile | Chest imaging | Lung function tests | Treatment | Outcomes |
| Chaudhry et al., 2025 (present case) | 20, female | Dyspnea, pleuritic chest pain | ANA, dsDNA, RNP, anti-Smith, Ro62 | Raised right hemidiaphragm, small bilateral pleural effusions, normal lung parenchyma | Restrictive pattern, reduced TLCO | Cyclophosphamide, rituximab | Clinical improvement with improved lung function tests |
| Roostaei et al., 2025 [ | 33, female | Dyspnea, pleuritic chest pain | ANA, dsDNA, anti-phospholipid IgM, reduced C3 and C4 | Raised right hemidiaphragm | Restrictive pattern, reduced TLCO | Corticosteroids, mycophenolate mofetil | Clinical improvement |
| Al-Karaja et al., 2023 [ | 35, female | Dyspnea, pleuritic chest pain | Not available | Bilateral basal atelectasis | Restrictive pattern | Corticosteroids, rituximab | Clinical improvement with improved lung function tests |
| He et al., 2024 [ | 35, female | Dyspnea, chest pain, fever, cough | ANA, dsDNA, anti-Smith, reduced complement | Thickened right pleura on CT | Restrictive pattern, reduced TLCO | Corticosteroids, tofacitinib | Clinical improvement with improved lung function tests |
| Shah et al., 2024 [ | 38, female | Dyspnea, pleuritic chest pain, non-productive cough | ANA, anti-cardiolipin, RNP, beta-2 glycoprotein, anti-Smith, reduced C3 | Raised right hemidiaphragm | Restrictive pattern, reduced TLCO | Intravenous corticosteroids, rituximab | Clinical improvement |
| DeCoste et al., 2021 [ | 11, male | Dyspnea, pleuritic chest pain, non-productive cough | ANA, dsDNA, Ro, anti-Smith, reduced C3 | Reduced lung volumes on HRCT, normal lung parenchyma | Restrictive pattern | Intravenous corticosteroids, rituximab | Clinical improvement |
| Goswami et al., 2016 [ | 38, female | Dyspnea, fever | ANA, Ro52 | Elevated hemidiaphragms bilaterally | Restrictive pattern | Intravenous corticosteroids, rituximab | Clinical improvement, normalization of lung function tests |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Myopathies and Dermatomyositis · Congenital Diaphragmatic Hernia Studies · Systemic Sclerosis and Related Diseases
Introduction
Dyspnea is a common symptom associated with systemic autoimmune diseases, such as systemic lupus erythematosus (SLE). Some more common causes of dyspnea in these patients include pleural disease, pneumonitis, pulmonary hypertension, and interstitial lung disease [1]. Nonetheless, some patients experience unexplained dyspnea despite comprehensive evaluation.
Among the rarer pulmonary manifestations of autoimmune disease is shrinking lung syndrome (SLS). The condition was first described by Hoffbrand and Beck in 1965 [2]. This is most commonly seen in patients with SLE, with an estimated prevalence of 0.5-1.53% in patients with this condition [3]. However, it can also be seen in other autoimmune conditions, such as rheumatoid arthritis, systemic sclerosis, and Sjogren’s disease. There are several theories regarding the etiology of SLS, including diaphragmatic dysfunction, pleural inflammation, and phrenic neuropathy. However, there is no clear evidence to explain the exact pathophysiology of this condition so far [3].
The most common symptoms seen in SLS are exertional dyspnea (99%) and pleuritic chest pain (76%). Fever (19%) and dry cough (8%) are rarely seen in patients with SLS. Patients can have concomitant features of SLE, most commonly arthritis (77%). Tachypnea, reduced chest wall expansion, and use of accessory muscles of respiration are the most frequently seen features on clinical examination. It is common to see a diagnostic delay in this condition, with 48% of patients presenting with over a year of symptoms before being formally diagnosed [4]. Here, we report a case of a young lady with early-onset SLS in the setting of SLE who demonstrated sustained response to combined cyclophosphamide and rituximab therapy.
Case presentation
A young lady in her 20s was under the care of the rheumatology department for inflammatory arthropathy. She initially presented with arthralgias, particularly of the small joints of the hands and feet. On examination, there was an absence of synovitis with normal cardiorespiratory, neurological, and abdominal examinations. Of note, there were no oral ulcers, skin rashes, or pericardial or pleural rub. Her autoimmune profile was positive for anti-nuclear antibodies (ANA) (homogeneous at 1/640), anti-RNP, anti-Smith, anti-dsDNA, and anti-Ro60 antibodies with normal complement levels. At the time of initial presentation, she did not meet the European Alliance of Associations for Rheumatology (EULAR)/American College of Rheumatology (ACR) diagnostic criteria for SLE, scoring 6/12 points for positive anti-dsDNA/anti-Smith antibodies [5]. Joint involvement was not significant enough to be counted towards the score. As such, she was treated for an articular presentation of possible mixed connective tissue disease (MCTD) with reducing dose of prednisolone (starting at 30 mg once daily, reducing by 5 mg every four days), hydroxychloroquine 200 mg twice daily, and oral methotrexate 20 mg once a week.
Several months following her diagnosis of MCTD, she developed exertional dyspnea, pleuritic chest pain, and reduced exercise tolerance. She had been diagnosed with right basal pneumonia on a recent hospital admission and was subsequently treated with multiple courses of oral antibiotics. However, she showed minimal improvement. Interval imaging showed full resolution of the right basal pneumonia, and CT pulmonary angiography showed no evidence of pulmonary embolism.
Three months after treatment of her pneumonia, she remained symptomatic with persistent shortness of breath on minimal exertion, fatigue, and infrequent pleuritic chest pain brought on by coughing. It was noted that around the same time, her joint symptoms significantly worsened. She had developed swelling of her hands and feet, along with morning stiffness that lasted more than an hour. At a follow-up clinic appointment, joint examination revealed polyarticular swelling and stiffness, particularly involving the small joints of her hands and feet, as well as left ankle swelling. On systemic examination, she was also noted to have decreased air entry in both lung bases on auscultation. Neurologically, she had 5/5 power, with normal tone, reflexes, coordination, and sensations in both upper and lower limbs. Cranial nerves were intact. She had unremarkable cardiac and abdominal examinations. A full set of investigations was performed, including full blood count, biochemistry, repeat autoimmune serology, inflammatory markers, and urinalysis. Results of the relevant investigations are detailed in Table 1 below.
Given the bilaterally reduced breath sounds, a chest radiograph was requested to exclude post-inflammatory pleural effusion. The image of the chest X-ray is shown in Figure 1, demonstrating a raised right hemidiaphragm and bilateral small pleural effusions.
Chest X-ray showing raised right hemidiaphragm with bilateral small pleural effusions.Larger arrow denotes raised right hemidiaphragm, and smaller arrows denote bilateral small pleural effusions
As symptoms persisted, a high-resolution computed tomography (HRCT) scan of the chest was also performed, which showed a persistently raised right hemidiaphragm with minimal atelectasis, along with trace pleural effusions bilaterally. It showed an otherwise normal lung parenchyma with no evidence of interstitial lung disease. Figure 2 shows a coronal view of her HRCT.
HRCT of the chest showing raised right hemidiaphragm and bilateral small effusions with otherwise normal lung parenchyma.The larger arrow shows a raised right hemidiaphragm, whereas the smaller arrows show small pleural effusions bilaterally.HRCT: high-resolution computed tomography
She was referred for pulmonary function tests, which confirmed a restrictive picture with reduced forced vital capacity (FVC), 34.3% of predicted, and a preserved FEV/FVC ratio of 1.12 (112%). There was a reduction in total lung capacity (TLC), 48% of predicted, and reduced gas transfer (TLCO), 51.4% of predicted. The relevant results of her pulmonary function tests are shown in Table 2.
A neurological cause of raised hemidiaphragm and restrictive lung physiology was not considered likely, as she had a normal neurological examination. There were also no alarming symptoms reported by the patient, such as weakness, swallowing or speech disturbances, double vision, or a history of spinal or head trauma.
Her immune profile remained unchanged on subsequent follow-ups. However, considering the development of polyarthritis since her initial presentation, her diagnosis of MCTD evolved to SLE as per EULAR/ACR 2019 criteria [5]. In the context of her autoimmune illness and respiratory symptoms, coupled with restrictive lung disease and an elevated hemidiaphragm, she was diagnosed with shrinking lung syndrome.
The first phase of her treatment was immunosuppression with cyclophosphamide and prednisolone over the first three months. She was given prednisolone 15 mg once daily along with a total of six intravenous infusions of cyclophosphamide 800 mg. The first three cyclophosphamide infusions were given at two-weekly intervals, followed by the next three at three-weekly intervals. She was given prophylactic co-trimoxazole 960 mg once daily while on cyclophosphamide. During this phase of three months, her usual methotrexate (20 mg once weekly) was withheld while hydroxychloroquine (200 mg once daily) was continued. The rationale behind holding her methotrexate was to reduce the possibility of liver dysfunction while on cyclophosphamide.
The second phase of her treatment was maintenance with rituximab, which was started a month after completing her course of cyclophosphamide. Two 1 g infusions of rituximab were given two weeks apart every six months for two years. After two years, rituximab was continued as an annual 1 g infusion. Alongside the rituximab, she was recommenced on her usual maintenance oral methotrexate 20 mg once weekly, and continued with hydroxychloroquine 200 mg once daily. After starting rituximab, her oral prednisolone was weaned down by 2.5 mg every month until it was eventually stopped. In addition to immunosuppression, she was advised to incorporate regular aerobic exercise in her daily routine to help improve her exercise tolerance. Over the course of treatment, she reported subjective improvement in her clinical symptoms compared to her initial presentation. Over the next three years, there was a significant improvement in her forced vital capacity from 34.3% to 66.8%, and a marginal increase in lung volumes from 48% to almost 68.1%. Figure 3 shows improvements in all parameters of serial lung function tests performed on a yearly basis since the diagnosis of SLS.
Serial lung function tests done at baseline and over time on a yearly basis since diagnosis of SLS showed an improvement in all parameters.FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLC: total lung capacity; % Pred: percentage predicted; SLS: shrinking lung syndrome
At the time of this report, she remains on extended interval annual rituximab infusions, along with oral methotrexate 20 mg once weekly and hydroxychloroquine 200 mg once daily.
Discussion
The time of onset of SLS as a respiratory complication of SLE is variable, with SLS occurring at any point during the course of the disease. The average age of onset of SLS is four years, but it can also occur as a presenting feature of SLE [6]. Our patient developed symptoms of SLS at around the same time as her diagnosis evolved from MCTD to SLE.
Diagnosis of SLS is usually made on the basis of characteristic features of this condition (dyspnea, chest pain, reduced lung volumes, restrictive lung physiology) and the exclusion of other differential diagnoses. Therefore, laboratory investigations, imaging, and pulmonary function tests play a vital role in the evaluation of these patients. A positive ANA is seen in virtually all patients with SLS; however, it is non-specific. Other blood tests that may support the diagnosis of the underlying connective tissue disease causing SLS include antiphospholipid serology, hypocomplementemia, and a positive ENA test (including SS-A, SS-B, anti-RNP, and anti-Sm) [3]. However, laboratory investigations alone do not confirm the diagnosis. Chest radiography commonly shows unilaterally or bilaterally raised hemidiaphragms, often with reduced lung volumes. CT imaging is useful to rule out the more common differentials, such as interstitial lung disease or pulmonary emboli [7]. Lung function tests typically show a restrictive pattern of lung disease [4]. However, it must be reiterated that SLS remains a diagnosis of exclusion.
There are no standardized guidelines for the management of SLS, and although immunosuppression is the mainstay of treatment, the efficacy of various immunosuppressants remains poorly established. Corticosteroids are usually employed as first-line treatment, although the dosage and duration have not been established in any randomized controlled trials to date. It is most commonly dosed at 0.5-1 mg/kg of prednisolone daily, and carefully adjusted depending on individual patient response [3]. In more refractory cases, steroids are used in adjunct with other immunosuppressive agents such as cyclophosphamide, azathioprine, rituximab, belimumab, or mycophenolate mofetil [4,6,8]. Rituximab appears to be emerging as an effective drug for inducing remission in SLS and was found to be effective in our patient as well [4,9,10-12].
In Table 3 below, we compare our patient’s case with other published cases of SLS occurring in the setting of SLE. We can note that biologic agents, particularly rituximab, have been increasingly used as a treatment option in the last decade, with positive clinical outcomes.
While most patients show an improvement in lung function tests with appropriate treatment, a study evaluating 35 cases of SLS showed that only 20% of the patients were able to achieve a normal vital capacity [8]. It is common for this condition to cause a chronic, mild restrictive deficit despite treatment. Untoward consequences such as respiratory failure, requirement of long-term oxygen, and death from this condition are extremely unlikely with this mild restrictive deficit [4].
Conclusions
Shrinking lung syndrome remains a diagnostic dilemma in the setting of systemic autoimmune diseases, in particular SLE. The present case demonstrates that it can manifest as a pulmonary complication earlier on in the course of the disease. It is imperative to consider SLS as a cause of unexplained dyspnea in a patient with SLE. Timely diagnosis and initiation of appropriate immunosuppression should remain a priority as improvements in restrictive lung deficit and quality of life are achievable goals in the management of SLS. It should, however, be noted that a degree of chronic restrictive lung deficit can be expected in SLS despite treatment. Finally, this study underscores the need for standardized guidelines in the treatment and management of SLS. In particular, the safety and efficacy of biologic agents need to be studied as several reports have demonstrated their clinical benefit in patients with SLS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary respiratory disease in patients with systemic lupus erythematosus: data from the Spanish Rheumatology Society Lupus Registry (RELESSER) cohort Arthritis Res Ther Narváez J Borrell H Sánchez-Alonso F 20201810.1186/s 13075-018-1776-8PMC 629995130567600 · doi ↗ · pubmed ↗
- 2“Unexplained” dyspnoea and shrinking lungs in systemic lupus erythematosus Br Med J Hoffbrand BI Beck ER 12731277119651427881610.1136/bmj.1.5445.1273 PMC 2166064 · doi ↗ · pubmed ↗
- 3Shrinking lung syndrome Stat Pearls [Internet] Colquhoun M Akram S Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 568683/33760442 · pubmed ↗
- 4Shrinking lung syndrome in systemic lupus erythematosus: a case series and review of the literature Medicine (Baltimore) Borrell H Narváez J Alegre JJ 95201610.1097/MD.0000000000004626 PMC 537082727537601 · doi ↗ · pubmed ↗
- 52019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for systemic lupus erythematosus Arthritis Rheumatol Aringer M Costenbader K Daikh D 140014127120193138546210.1002/art.40930 PMC 6827566 · doi ↗ · pubmed ↗
- 6Shrinking lung syndrome as an early manifestation of systemic lupus erythematosus: a case report with literature review Respirol Case Rep Roostaei G Kazemizadeh H Rahimi B Abtahi H Mokri MY Rad NK 13202510.1002/rcr 2.70255 PMC 1223122040625882 · doi ↗ · pubmed ↗
- 7The shrinking lungs syndrome in systemic lupus erythematosus Mayo Clin Proc Warrington KJ Moder KG Brutinel WM 4674727520001080707510.4065/75.5.467 · doi ↗ · pubmed ↗
- 8Tofacitinib treatment in refractory systemic lupus erythematosus with shrinking lung syndrome: a case-based review Biomed J Sci Tech Res He N Feng B Han Y Shen M 542024